Embed Size (px)
Citation preview
©2012, the Lumenis Group of Companies. All rights reserved. Lumenis, its logo, UltraPulse and SurgiTouch are trademarks or registered trademarks of the Lumenis Group of Companies. Specifications are subject to change without notice. PB-1143470 Rev. A
Technique Guide | September 2012 | Page 1 of 6
CASE INTRODUCTION
Anatomy & Definition:
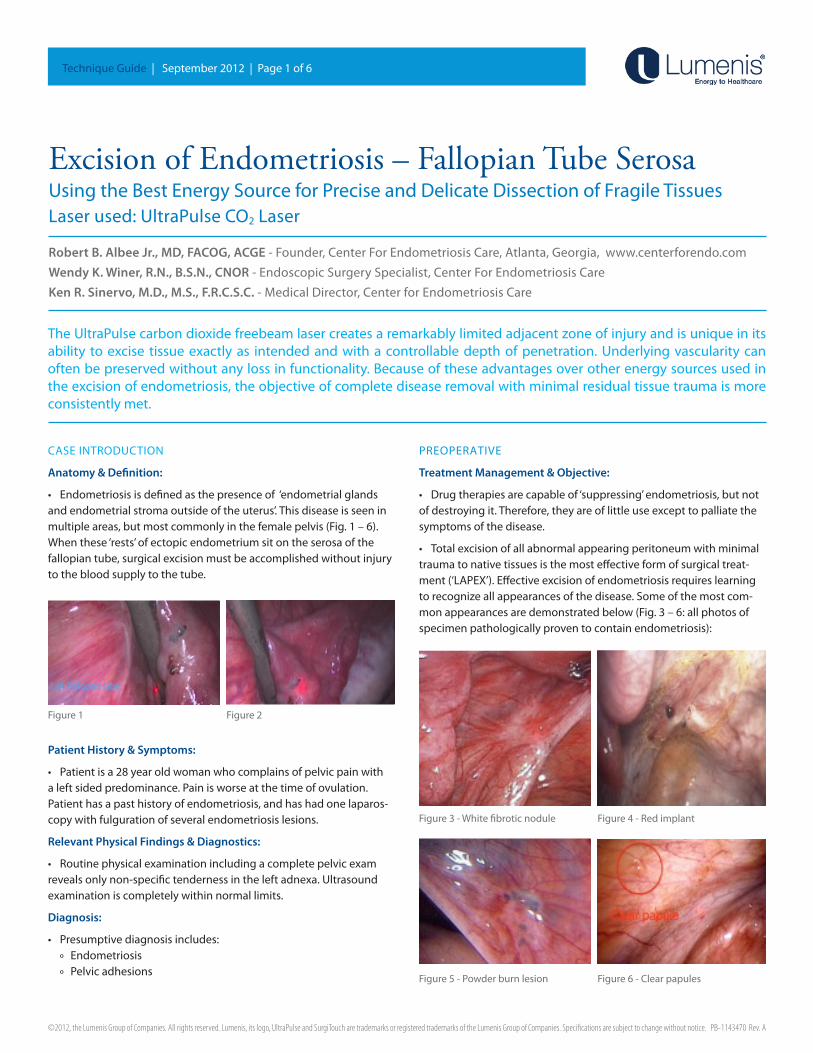
• Endometriosisisdefinedasthepresenceof‘endometrialglandsandendometrialstromaoutsideoftheuterus’.Thisdiseaseisseeninmultipleareas,butmostcommonlyinthefemalepelvis(Fig.1–6).Whenthese‘rests’ofectopicendometriumsitontheserosaofthefallopiantube,surgicalexcisionmustbeaccomplishedwithoutinjurytothebloodsupplytothetube.
Patient History & Symptoms:
• Patientisa28yearoldwomanwhocomplainsofpelvicpainwithaleftsidedpredominance.Painisworseatthetimeofovulation.Patienthasapasthistoryofendometriosis,andhashadonelaparos-copywithfulgurationofseveralendometriosislesions.
Relevant Physical Findings & Diagnostics:
• Routinephysicalexaminationincludingacompletepelvicexamrevealsonlynon-specifictendernessintheleftadnexa.Ultrasoundexaminationiscompletelywithinnormallimits.
Diagnosis:
• Presumptivediagnosisincludes:
º Endometriosis
º Pelvicadhesions
PREOPERATIVE
Treatment Management & Objective:
• Drugtherapiesarecapableof‘suppressing’endometriosis,butnotofdestroyingit.Therefore,theyareoflittleuseexcepttopalliatethesymptomsofthedisease.
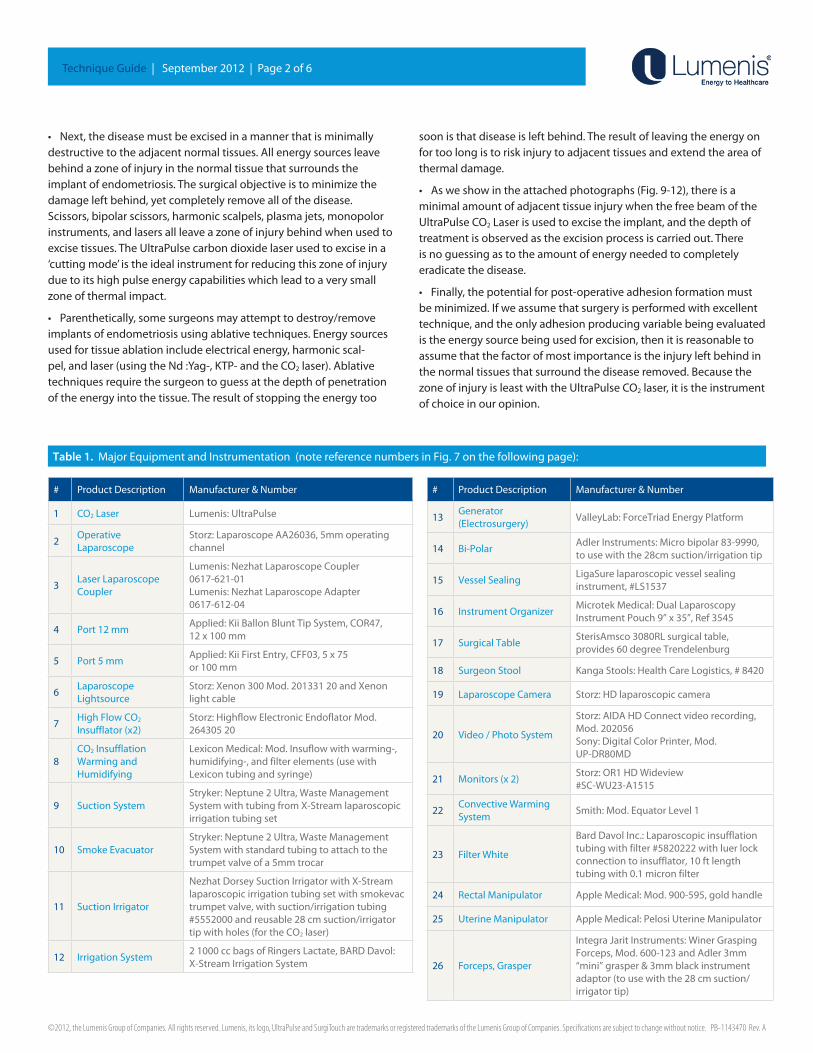
• Totalexcisionofallabnormalappearingperitoneumwithminimaltraumatonativetissuesisthemosteffectiveformofsurgicaltreat-ment(‘LAPEX’).Effectiveexcisionofendometriosisrequireslearningtorecognizeallappearancesofthedisease.Someofthemostcom-monappearancesaredemonstratedbelow(Fig.3–6:allphotosofspecimenpathologicallyproventocontainendometriosis):
Excision of Endometriosis – Fallopian Tube SerosaUsingtheBestEnergySourceforPreciseandDelicateDissectionofFragileTissuesLaserused:UltraPulseCO2Laser
Robert B. Albee Jr., MD, FACOG, ACGE-Founder,CenterForEndometriosisCare,Atlanta,Georgia,www.centerforendo.com
Wendy K. Winer, R.N., B.S.N., CNOR-EndoscopicSurgerySpecialist,CenterForEndometriosisCare
Ken R. Sinervo, M.D., M.S., F.R.C.S.C.-MedicalDirector,CenterforEndometriosisCare
Figure1 Figure2
Figure3-Whitefibroticnodule Figure4-Redimplant
Figure5-Powderburnlesion Figure6-Clearpapules
TheUltraPulsecarbondioxidefreebeamlasercreatesaremarkablylimitedadjacentzoneofinjuryandisuniqueinitsability toexcise tissueexactlyas intendedandwithacontrollabledepthofpenetration.Underlyingvascularitycanoftenbepreservedwithoutanylossinfunctionality.Becauseoftheseadvantagesoverotherenergysourcesusedintheexcisionofendometriosis,theobjectiveofcompletediseaseremovalwithminimalresidualtissuetraumaismoreconsistentlymet.
©2012, the Lumenis Group of Companies. All rights reserved. Lumenis, its logo, UltraPulse and SurgiTouch are trademarks or registered trademarks of the Lumenis Group of Companies. Specifications are subject to change without notice. PB-1143470 Rev. A
Technique Guide | September 2012 | Page 2 of 6
• Next,thediseasemustbeexcisedinamannerthatisminimallydestructivetotheadjacentnormaltissues.Allenergysourcesleavebehindazoneofinjuryinthenormaltissuethatsurroundstheimplantofendometriosis.Thesurgicalobjectiveistominimizethedamageleftbehind,yetcompletelyremoveallofthedisease. Scissors,bipolarscissors,harmonicscalpels,plasmajets,monopolorinstruments,andlasersallleaveazoneofinjurybehindwhenusedtoexcisetissues.TheUltraPulsecarbondioxidelaserusedtoexciseina‘cuttingmode’istheidealinstrumentforreducingthiszoneofinjuryduetoitshighpulseenergycapabilitieswhichleadtoaverysmallzoneofthermalimpact.
• Parenthetically,somesurgeonsmayattempttodestroy/removeimplantsofendometriosisusingablativetechniques.Energysourcesusedfortissueablationincludeelectricalenergy,harmonicscal-pel,andlaser(usingtheNd:Yag-,KTP-andtheCO2laser).Ablativetechniquesrequirethesurgeontoguessatthedepthofpenetrationoftheenergyintothetissue.Theresultofstoppingtheenergytoo
soonisthatdiseaseisleftbehind.Theresultofleavingtheenergyonfortoolongistoriskinjurytoadjacenttissuesandextendtheareaofthermaldamage.
• Asweshowintheattachedphotographs(Fig.9-12),thereisaminimalamountofadjacenttissueinjurywhenthefreebeamoftheUltraPulseCO2Laserisusedtoexcisetheimplant,andthedepthoftreatmentisobservedastheexcisionprocessiscarriedout.There isnoguessingastotheamountofenergyneededtocompletelyeradicatethedisease.
• Finally,thepotentialforpost-operativeadhesionformationmustbeminimized.Ifweassumethatsurgeryisperformedwithexcellenttechnique,andtheonlyadhesionproducingvariablebeingevaluatedistheenergysourcebeingusedforexcision,thenitisreasonabletoassumethatthefactorofmostimportanceistheinjuryleftbehindinthenormaltissuesthatsurroundthediseaseremoved.BecausethezoneofinjuryisleastwiththeUltraPulseCO2laser,itistheinstrumentofchoiceinouropinion.
# ProductDescription Manufacturer & Number
1 CO2Laser Lumenis:UltraPulse
2OperativeLaparoscope
Storz:LaparoscopeAA26036,5mmoperatingchannel
3LaserLaparoscopeCoupler
Lumenis:NezhatLaparoscopeCoupler 0617-621-01Lumenis:NezhatLaparoscopeAdapter 0617-612-04
4 Port 12 mmApplied:KiiBallonBluntTipSystem,COR47, 12x100mm
5 Port5mmApplied:KiiFirstEntry,CFF03,5x75 or 100 mm
6LaparoscopeLightsource
Storz:Xenon300Mod.20133120andXenonlightcable
7HighFlowCO2 Insufflator(x2)
Storz:HighflowElectronicEndoflatorMod.26430520
8CO2InsufflationWarming and Humidifying
LexiconMedical:Mod.Insuflowwithwarming-,humidifying-,andfilterelements(usewithLexicontubingandsyringe)
9 SuctionSystemStryker:Neptune2Ultra,WasteManagementSystemwithtubingfromX-Streamlaparoscopicirrigationtubingset
10 SmokeEvacuatorStryker:Neptune2Ultra,WasteManagementSystemwithstandardtubingtoattachtothetrumpetvalveofa5mmtrocar
11 Suction Irrigator
NezhatDorseySuctionIrrigatorwithX-Streamlaparoscopicirrigationtubingsetwithsmokevactrumpetvalve,withsuction/irrigationtubing#5552000andreusable28cmsuction/irrigatortipwithholes(fortheCO2laser)
12 IrrigationSystem21000ccbagsofRingersLactate,BARDDavol:X-StreamIrrigationSystem
# ProductDescription Manufacturer & Number
13Generator (Electrosurgery)
ValleyLab:ForceTriadEnergyPlatform
14 Bi-PolarAdlerInstruments:Microbipolar83-9990,tousewiththe28cmsuction/irrigationtip
15 VesselSealingLigaSurelaparoscopicvesselsealinginstrument,#LS1537
16 InstrumentOrganizerMicrotekMedical:DualLaparoscopyInstrumentPouch9”x35”,Ref3545
17 SurgicalTableSterisAmsco3080RLsurgicaltable,provides60degreeTrendelenburg
18 SurgeonStool KangaStools:HealthCareLogistics,#8420
19 LaparoscopeCamera Storz:HDlaparoscopiccamera
20 Video/PhotoSystem
Storz:AIDAHDConnectvideorecording,Mod.202056Sony:DigitalColorPrinter,Mod. UP-DR80MD
21 Monitors(x2)Storz:OR1HDWideview #SC-WU23-A1515
22ConvectiveWarmingSystem
Smith:Mod.EquatorLevel1
23 FilterWhite
BardDavolInc.:Laparoscopicinsufflationtubingwithfilter#5820222withluerlockconnectiontoinsufflator,10ftlengthtubingwith0.1micronfilter
24 RectalManipulator AppleMedical:Mod.900-595,goldhandle
25 UterineManipulator AppleMedical:PelosiUterineManipulator
26 Forceps,Grasper
IntegraJaritInstruments:WinerGraspingForceps,Mod.600-123andAdler3mm“mini”grasper&3mmblackinstrumentadaptor(tousewiththe28cmsuction/irrigatortip)
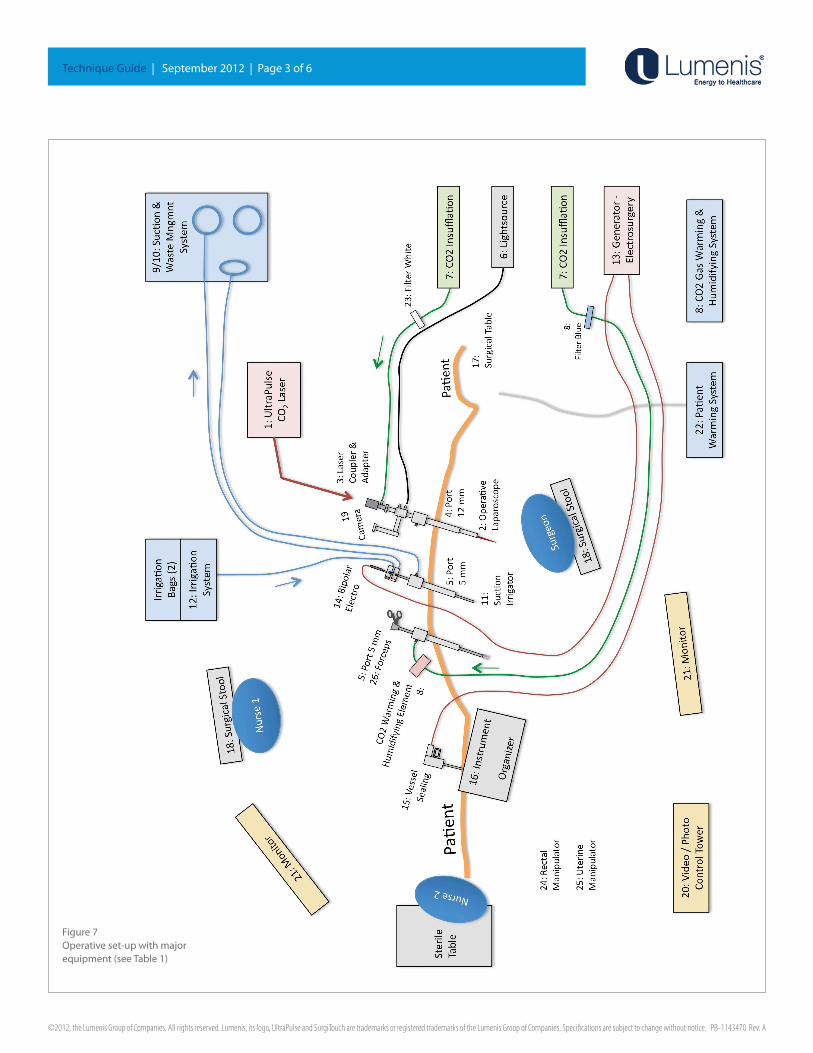
Table 1.MajorEquipmentandInstrumentation(notereferencenumbersinFig.7onthefollowingpage):
©2012, the Lumenis Group of Companies. All rights reserved. Lumenis, its logo, UltraPulse and SurgiTouch are trademarks or registered trademarks of the Lumenis Group of Companies. Specifications are subject to change without notice. PB-1143470 Rev. A
Technique Guide|September2012|Page3of6
Figure7Operativeset-upwithmajor equipment(seeTable1)
©2012, the Lumenis Group of Companies. All rights reserved. Lumenis, its logo, UltraPulse and SurgiTouch are trademarks or registered trademarks of the Lumenis Group of Companies. Specifications are subject to change without notice. PB-1143470 Rev. A
Technique Guide|September2012|Page4of6
PATIENT PREPARATION
• Anesthesia:Ageneralanesthesiaisadministeredbytheanesthesiadepartment.Thepatientisintubatedandmuscleparalysisisusedtocontrolrespirations.
• PatientPositioning:(seeAORN2012RecommendedGuidelines).Thepatientispositionedonastandardsurgicaltableinthesemi-lithotomyposition.ThetablemattressisvelcroedtothetabletopreventslidingduringtheTrendelenburgpositioning.Thearmsarecarefullywrappedforprotectionandplacedbesidethetrunktoallowthesurgeontoworkatthelevelofthepatientsshoulders.Protectiveboots(AllenMedicalSystemsPALstirrupswithfeatherlift,#10023)areusedtocushionthepatient’sfeet,ankles,andcalves.Pneumaticcompressiondevices(ALPalternatinglegpressureforDVTprophy-laxis,40-60mmHg)areusedonthepatientscalvesandthighs.
• Pelvicexaminationisthenperformed,andthecervixgentlydilatedtoan21Prattdilator.Asingletoothtenaculumisplacedontheante-riorlipofthecervixanda‘Pelosi’uterinemanipulatoristheninsertedintotheuterusandaffixedtoasingletoothtenaculum.
• Arectalmanipulator(AppleMedical,900-575,goldhandle)isthenplacedintherectumforlatermanipulationasneeded.
• PatientDraping:(seeAORN2012RecommendedGuidelinesforpatientdrapingandpreppingofthesurgicalsite).AfteraChloraprep(withtint,Carefusion,Leawood,KS)skinprepiswidelydoneoverthesurgicalsite,a‘laparoscopy’drape(KimberlyClark”LaparoscopyPack”)isthenusedtomaintainasterileoperatingfield.Adisposableinstrumentorganizerisusedonthepatientsleftlegtokeepthemostoftenusedlaparoscopicinstrumentswithinreachofthesurgeon.
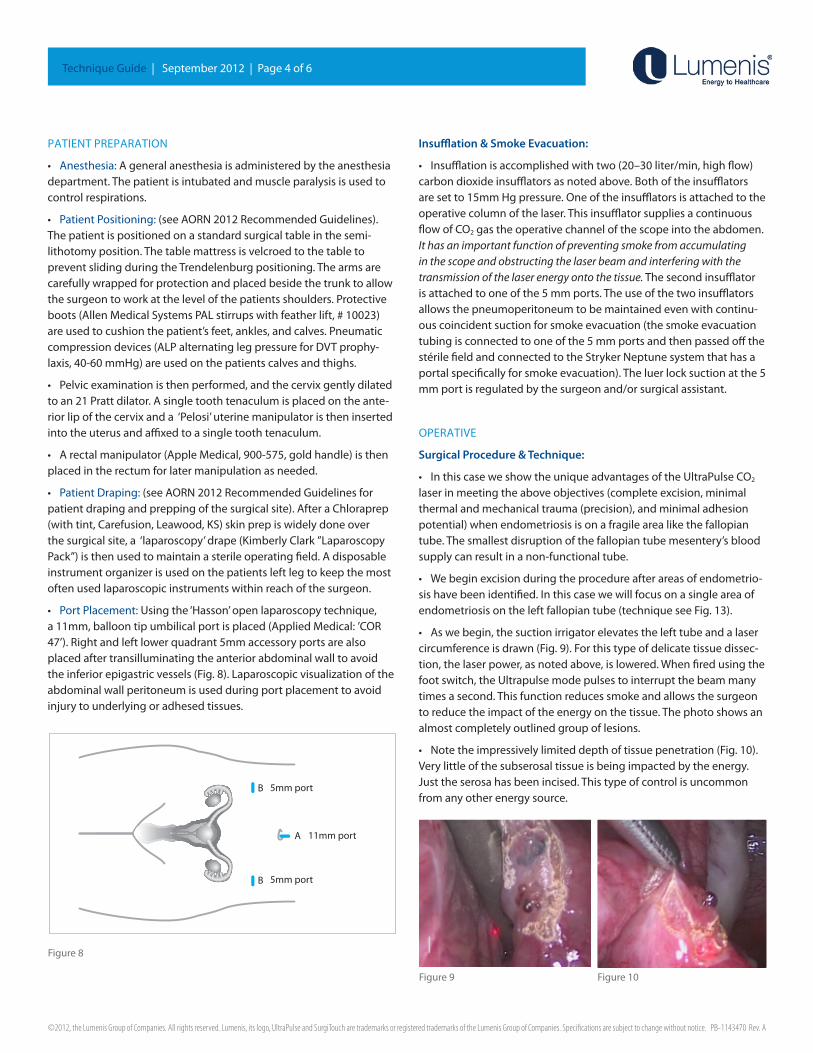
• PortPlacement:Usingthe‘Hasson’openlaparoscopytechnique,a11mm,balloontipumbilicalportisplaced(AppliedMedical:’COR47’).Rightandleftlowerquadrant5mmaccessoryportsarealsoplacedaftertransilluminatingtheanteriorabdominalwalltoavoidtheinferiorepigastricvessels(Fig.8).Laparoscopicvisualizationoftheabdominalwallperitoneumisusedduringportplacementtoavoidinjurytounderlyingoradhesedtissues.
Insufflation & Smoke Evacuation:
• Insufflationisaccomplishedwithtwo(20–30liter/min,highflow)carbondioxideinsufflatorsasnotedabove.Bothoftheinsufflatorsaresetto15mmHgpressure.Oneoftheinsufflatorsisattachedtotheoperativecolumnofthelaser.ThisinsufflatorsuppliesacontinuousflowofCO2gastheoperativechannelofthescopeintotheabdomen.It has an important function of preventing smoke from accumulating in the scope and obstructing the laser beam and interfering with the transmission of the laser energy onto the tissue.Thesecondinsufflatorisattachedtooneofthe5mmports.Theuseofthetwoinsufflatorsallowsthepneumoperitoneumtobemaintainedevenwithcontinu-ouscoincidentsuctionforsmokeevacuation(thesmokeevacuationtubingisconnectedtooneofthe5mmportsandthenpassedoffthestérilefieldandconnectedtotheStrykerNeptunesystemthathasaportalspecificallyforsmokeevacuation).Theluerlocksuctionatthe5mmportisregulatedbythesurgeonand/orsurgicalassistant.
OPERATIVE
Surgical Procedure & Technique:
• InthiscaseweshowtheuniqueadvantagesoftheUltraPulseCO2 laserinmeetingtheaboveobjectives(completeexcision,minimalthermalandmechanicaltrauma(precision),andminimaladhesionpotential)whenendometriosisisonafragilearealikethefallopiantube.Thesmallestdisruptionofthefallopiantubemesentery’sbloodsupplycanresultinanon-functionaltube.
• Webeginexcisionduringtheprocedureafterareasofendometrio-sishavebeenidentified.Inthiscasewewillfocusonasingleareaofendometriosisontheleftfallopiantube(techniqueseeFig.13).
• Aswebegin,thesuctionirrigatorelevatesthelefttubeandalasercircumferenceisdrawn(Fig.9).Forthistypeofdelicatetissuedissec-tion,thelaserpower,asnotedabove,islowered.Whenfiredusingthefootswitch,theUltrapulsemodepulsestointerruptthebeammanytimesasecond.Thisfunctionreducessmokeandallowsthesurgeontoreducetheimpactoftheenergyonthetissue.Thephotoshowsanalmostcompletelyoutlinedgroupoflesions.
• Notetheimpressivelylimiteddepthoftissuepenetration(Fig.10).Verylittleofthesubserosaltissueisbeingimpactedbytheenergy.Justtheserosahasbeenincised.Thistypeofcontrolisuncommonfromanyotherenergysource.
A
B
B
11mm port
5mm port
5mm port
Figure8
Figure9 Figure10
©2012, the Lumenis Group of Companies. All rights reserved. Lumenis, its logo, UltraPulse and SurgiTouch are trademarks or registered trademarks of the Lumenis Group of Companies. Specifications are subject to change without notice. PB-1143470 Rev. A
Technique Guide|September2012|Page5of6
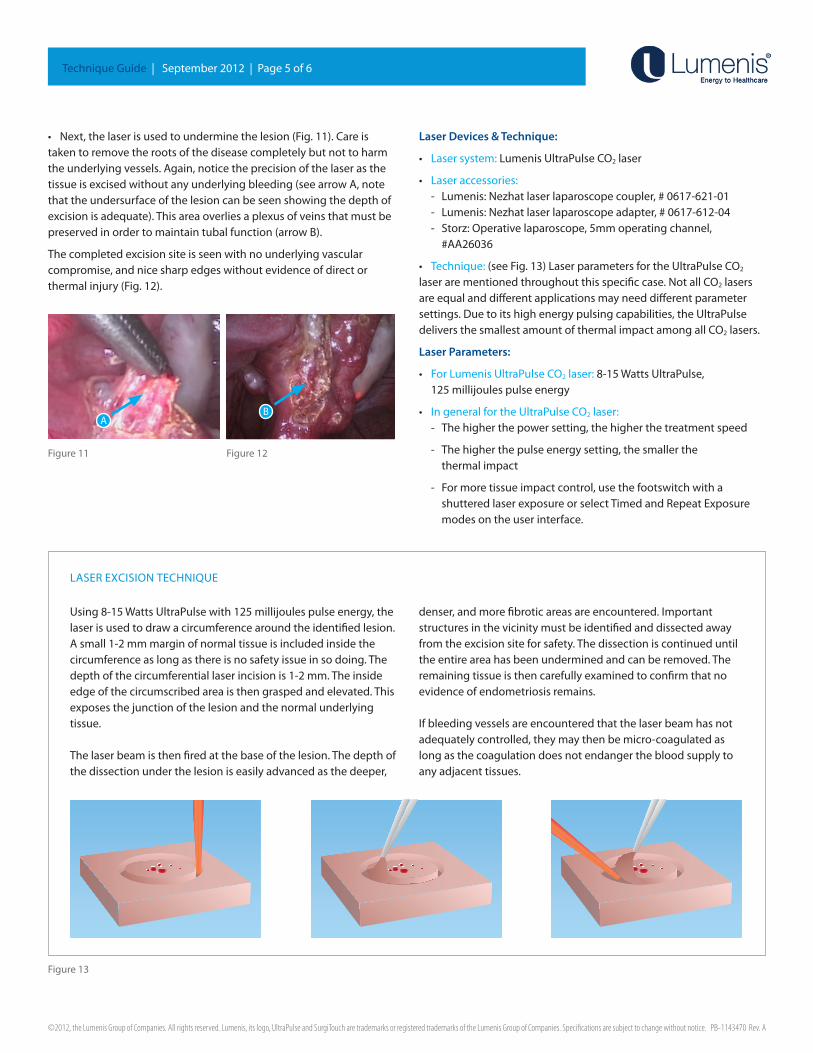
• Next,thelaserisusedtounderminethelesion(Fig.11).Careistakentoremovetherootsofthediseasecompletelybutnottoharmtheunderlyingvessels.Again,noticetheprecisionofthelaserasthetissueisexcisedwithoutanyunderlyingbleeding(seearrowA,notethattheundersurfaceofthelesioncanbeseenshowingthedepthofexcisionisadequate).Thisareaoverliesaplexusofveinsthatmustbepreservedinordertomaintaintubalfunction(arrowB).
Thecompletedexcisionsiteisseenwithnounderlyingvascular compromise,andnicesharpedgeswithoutevidenceofdirectorthermalinjury(Fig.12).
Laser Devices & Technique:
• Lasersystem:LumenisUltraPulseCO2laser
• Laseraccessories: - Lumenis:Nezhatlaserlaparoscopecoupler,#0617-621-01 - Lumenis:Nezhatlaserlaparoscopeadapter,#0617-612-04- Storz:Operativelaparoscope,5mmoperatingchannel,#AA26036
• Technique:(seeFig.13)LaserparametersfortheUltraPulseCO2 laserarementionedthroughoutthisspecificcase.NotallCO2lasersareequalanddifferentapplicationsmayneeddifferentparametersettings.Duetoitshighenergypulsingcapabilities,theUltraPulsedeliversthesmallestamountofthermalimpactamongallCO2lasers.
Laser Parameters:
• ForLumenisUltraPulseCO2laser:8-15WattsUltraPulse,125millijoulespulseenergy
• IngeneralfortheUltraPulseCO2laser:- Thehigherthepowersetting,thehigherthetreatmentspeed
- Thehigherthepulseenergysetting,thesmallerthethermalimpact
- Formoretissueimpactcontrol,usethefootswitchwitha shutteredlaserexposureorselectTimedandRepeatExposuremodesontheuserinterface.
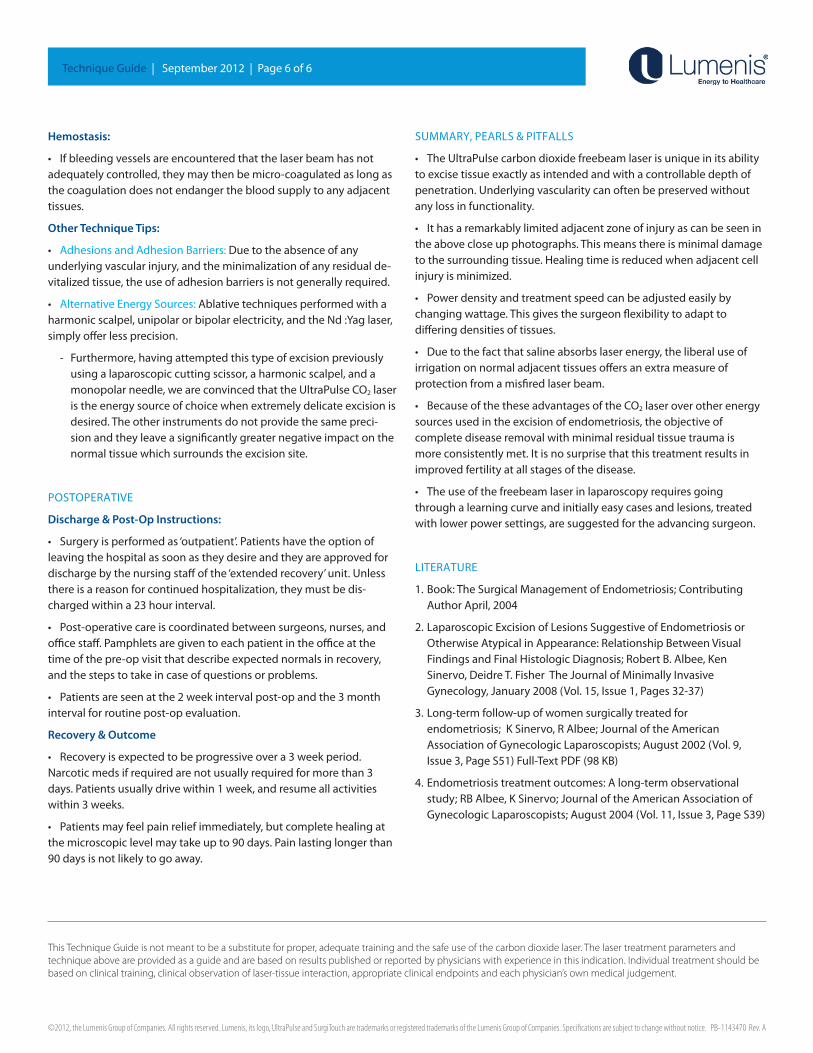
Using8-15WattsUltraPulsewith125millijoulespulseenergy,thelaserisusedtodrawacircumferencearoundtheidentifiedlesion.Asmall1-2mmmarginofnormaltissueisincludedinsidethecircumferenceaslongasthereisnosafetyissueinsodoing.Thedepthofthecircumferentiallaserincisionis1-2mm.Theinsideedgeofthecircumscribedareaisthengraspedandelevated.Thisexposesthejunctionofthelesionandthenormalunderlyingtissue.
Thelaserbeamisthenfiredatthebaseofthelesion.Thedepthofthedissectionunderthelesioniseasilyadvancedasthedeeper,
denser,andmorefibroticareasareencountered.Importantstructuresinthevicinitymustbeidentifiedanddissectedawayfromtheexcisionsiteforsafety.Thedissectioniscontinueduntiltheentireareahasbeenunderminedandcanberemoved.Theremainingtissueisthencarefullyexaminedtoconfirmthatnoevidenceofendometriosisremains.
Ifbleedingvesselsareencounteredthatthelaserbeamhasnotadequatelycontrolled,theymaythenbemicro-coagulatedaslongasthecoagulationdoesnotendangerthebloodsupplytoanyadjacenttissues.
Figure13
LASEREXCISIONTECHNIqUE
Figure11 Figure12
AB
©2012, the Lumenis Group of Companies. All rights reserved. Lumenis, its logo, UltraPulse and SurgiTouch are trademarks or registered trademarks of the Lumenis Group of Companies. Specifications are subject to change without notice. PB-1143470 Rev. A
Technique Guide | September 2012 | Page 6 of 6
Hemostasis:
• Ifbleedingvesselsareencounteredthatthelaserbeamhasnotadequatelycontrolled,theymaythenbemicro-coagulatedaslongasthecoagulationdoesnotendangerthebloodsupplytoanyadjacenttissues.
Other Technique Tips:
• AdhesionsandAdhesionBarriers:Duetotheabsenceofanyunderlyingvascularinjury,andtheminimalizationofanyresidualde-vitalizedtissue,theuseofadhesionbarriersisnotgenerallyrequired.
• AlternativeEnergySources:Ablativetechniquesperformedwithaharmonicscalpel,unipolarorbipolarelectricity,andtheNd:Yaglaser,simplyofferlessprecision.
- Furthermore,havingattemptedthistypeofexcisionpreviouslyusingalaparoscopiccuttingscissor,aharmonicscalpel,andamonopolarneedle,weareconvincedthattheUltraPulseCO2laseristheenergysourceofchoicewhenextremelydelicateexcisionisdesired.Theotherinstrumentsdonotprovidethesamepreci-sionandtheyleaveasignificantlygreaternegativeimpactonthenormaltissuewhichsurroundstheexcisionsite.
POSTOPERATIVE
Discharge & Post-Op Instructions:
• Surgeryisperformedas‘outpatient’.Patientshavetheoptionofleavingthehospitalassoonastheydesireandtheyareapprovedfordischargebythenursingstaffofthe‘extendedrecovery’unit.Unlessthereisareasonforcontinuedhospitalization,theymustbedis-chargedwithina23hourinterval.
• Post-operativecareiscoordinatedbetweensurgeons,nurses,andofficestaff.Pamphletsaregiventoeachpatientintheofficeatthetimeofthepre-opvisitthatdescribeexpectednormalsinrecovery,andthestepstotakeincaseofquestionsorproblems.
• Patientsareseenatthe2weekintervalpost-opandthe3monthintervalforroutinepost-opevaluation.
Recovery & Outcome
• Recoveryisexpectedtobeprogressiveovera3weekperiod.Narcoticmedsifrequiredarenotusuallyrequiredformorethan3days.Patientsusuallydrivewithin1week,andresumeallactivitieswithin3weeks.
• Patientsmayfeelpainreliefimmediately,butcompletehealingatthemicroscopiclevelmaytakeupto90days.Painlastinglongerthan90daysisnotlikelytogoaway.
SUMMARY,PEARLS&PITFALLS
• TheUltraPulsecarbondioxidefreebeamlaserisuniqueinitsabilitytoexcisetissueexactlyasintendedandwithacontrollabledepthofpenetration.Underlyingvascularitycanoftenbepreservedwithoutanylossinfunctionality.
• Ithasaremarkablylimitedadjacentzoneofinjuryascanbeseenintheabovecloseupphotographs.Thismeansthereisminimaldamagetothesurroundingtissue.Healingtimeisreducedwhenadjacentcellinjuryisminimized.
• Powerdensityandtreatmentspeedcanbeadjustedeasilybychangingwattage.Thisgivesthesurgeonflexibilitytoadaptto differingdensitiesoftissues.
• Duetothefactthatsalineabsorbslaserenergy,theliberaluseofirrigationonnormaladjacenttissuesoffersanextrameasureof protectionfromamisfiredlaserbeam.
• BecauseofthetheseadvantagesoftheCO2laseroverotherenergysourcesusedintheexcisionofendometriosis,theobjectiveof completediseaseremovalwithminimalresidualtissuetraumaismoreconsistentlymet.Itisnosurprisethatthistreatmentresultsinimprovedfertilityatallstagesofthedisease.
• Theuseofthefreebeamlaserinlaparoscopyrequiresgoingthroughalearningcurveandinitiallyeasycasesandlesions,treatedwithlowerpowersettings,aresuggestedfortheadvancingsurgeon.
LITERATURE
1.Book:TheSurgicalManagementofEndometriosis;ContributingAuthorApril,2004
2.LaparoscopicExcisionofLesionsSuggestiveofEndometriosisorOtherwiseAtypicalinAppearance:RelationshipBetweenVisualFindingsandFinalHistologicDiagnosis;RobertB.Albee,KenSinervo,DeidreT.FisherTheJournalofMinimallyInvasiveGynecology,January2008(Vol.15,Issue1,Pages32-37)
3.Long-termfollow-upofwomensurgicallytreatedforendometriosis;KSinervo,RAlbee;JournaloftheAmericanAssociationofGynecologicLaparoscopists;August2002(Vol.9,Issue3,PageS51)Full-TextPDF(98KB)
4.Endometriosistreatmentoutcomes:Along-termobservationalstudy;RBAlbee,KSinervo;JournaloftheAmericanAssociationofGynecologicLaparoscopists;August2004(Vol.11,Issue3,PageS39)
This Technique Guide is not meant to be a substitute for proper, adequate training and the safe use of the carbon dioxide laser. The laser treatment parameters and technique above are provided as a guide and are based on results published or reported by physicians with experience in this indication. Individual treatment should be based on clinical training, clinical observation of laser-tissue interaction, appropriate clinical endpoints and each physician’s own medical judgement.





























