Embed Size (px)
DESCRIPTION
Endocrine Response on Stress and Injury
Citation preview

Endocrine Response :To Stress and Injury
Stress is the ‘wear and tear on the body’…
-Hans Selye

The men who STRESSED us:
Hans Selye researched the effects of stress on rats and other animals by exposing them to unpleasant or harmful stimuli introduced the stress response mechanism known as General Adaptation Syndrome in 1936

Richard Lazarus
published in 1974 a model dividing stress into eustress and distress. His model argues that cognitive processes of appraisal are central in determining whether a situation is potentially threatening or harmful

What is stress??
Stress is a feeling experienced when a person thinks that "the demands exceed the personal and social resources the individual is able to mobilize.”
-Richard S Lazarus

Homeostasis
the term used which means the harmonious equilibrium of many physical and emotional factors that permit the body to maintain a steady state of health
Stress is a departure from homeostasis and caused by stressors.

Stressors include:
-physical (heat, cold)-chemical (no oxygen)-physiological (exercise)-psychological, emotional (fear,
anxiety)-social (personal conflicts)

Reaction of the body to stress

Type of Stress?
Eustress comes from good sources; (+) stress It arises at points of increased physical
activity, enthusiasm, creativity and when motivation and inspiration is needed.
Examples: Winning the lottery Passing an exam

STRESS!!!!!!
Distress comes from bad sources; (-) stress the stress that the mind and body
undergoes when the normal routine is constantly adjusted and altered.
Ex: being carnapped holdapped and kidnapped all in a day
There are actually two types of distress: acute stress and chronic stress.

Types of Stress cont’
Acute stress usually for short time and may be due to work
pressure, meeting deadlines pressure or minor accident, over exertion, increased physical activity, searching something but you misplaced it, or similar things.
Symptoms of this type of tension are headaches, back pain, stomach problems, rapid heartbeat, muscle aches or body pain.

Types of Stress cont’
Chronic Stress prolonged stress that exists for weeks,
months, or even years. This stress is due to poverty, broken hearts, stressed families and failed marriages, chronic illness and successive failures in life.
People suffering from this type of stress get used to it and may even not realize that they are under chronic stress.
It is very harmful to their health.

Stress Response
General adaptation syndrome, or GAS
(FIGHT or FLIGHT system)universal response to the stressors involved two major systems of the body,
the nervous system and the endocrine (or hormonal) system.

Three distinctive stages :
Stage 1: Alarm reaction (AR)the immediate reaction to a stressor
(physical or psychological) the body releases adrenaline and a
variety of other psychological mechanisms to combat the stress and to stay in control that is, to bring about the fight or flight response.

Fight or Flight responses
Increased heart rate Constriction of blood vessels of most viscera and
skin Dilation of blood vessels of heart, lungs and skeletal
muscles Contraction of spleen Conversion of glycogen into glucose in liver Sweating Dilation of airways Decrease in digestive activities Water retention and elevated blood pressure

Stage 2: Stage of resistance (SR)
might also be named the stage of adaptation, instead of the stage of resistance
during this phase, if the stress continues, the body adapts to the stressors it is exposed to
Changes at many levels take place in order to reduce the effect of the stressor

Resistance ResponsesCortisol Lypolysis (breakdown of fat stored in fat cells ) Glyconeogenesis (metabolic pathway that results in the
generation of glucose from non-carbohydrate carbon substrates such as pyruvate, lactate, glycerol, and glucogenic amino acids)
Protein catabolism Sensitive blood vessels Reduce inflammationIGF Lipolysis Glycogenolysis (the catabolism of glycogen by cleavage of a
glucose monomer through cleavage with inorganic phosphate to produce glucose-1-phosphate)
TH increased use of glucose to produce ATP

Stage 3: Stage of exhaustion (SE)
the body has run out of its reserve of body energy and immunity.
mental, physical and emotional resources suffer heavily.
body experiences "adrenal exhaustion". blood sugar levels dec. as the adrenals
become depleted, leading to decreased stress tolerance, progressive mental and physical exhaustion, illness and collapse.
In both cases, your body can not adapt & thus exhaustion follows.

Summary of Stress Response !?


Components of Nervous SystemDuring the Stress Response
1. Hypothalamus
2. Pituitary gland
-anterior
-posterior
3. Adrenal gland
-medulla
-cortex

Hypothalamus
Regulates homeostatic functions:-body temperature-thirst/urine output-food intake
Influences emotional and behavioral patterns-changes physiological responses basedon emotional stimuli (ie: anxiety - heartbeat)
Links the nervous system with the endocrine system-anterior pituitary-posterior pituitary


Interaction of hypothalamus with pituitary
Posterior Pituitary:Direct connectionthrough neurosecretory neurons
Anterior Pituitary:Hormones are transported throughportal system

Sympathetic Nervous System- controlled by bunches of
nerves called ganglions.-branches from the spine
throughout the body.-during the stress response, functions to
divert energy away from
processes such as digestion, immune function,etc.

Endocrine Response
Start of response: Hypothalamus – detects stress begins
alarm phase Autonomic Nervous System - provides the
rapid response to stress commonly known as the fight or flight response
- engages sympathetic division of the nervous system
Sympathetic nerves release adrenaline

Adrenaline Rush effects….

In cases of blood lost from injury, kidney
help minimize loss..
How?
1. Hypothalamus release (1.)antidiuretics hormone (ADH)
Purpose: to make the kidney take water from the urine and put it back into the
blood
2. Adrenal glands can also make the kidneys move fluid from the urine back into the blood.
Fix whatever is causing the stress.

What makes them do it? The kidney itself located just below them
Renin - release by the kidney when their blood supply is reduced during alarm phase.
Renin + other protein in the blood = angiotensin (which means "blood vessel constricting").
Aldosterone – release by the adrenal cortex of the adrenal gland due to stimulation of angiotensin
- makes the kidneys secrete potassium into the urine and reabsorb sodium and water into the blood.
The hypothalamus and adrenal cortex work together in the resistance phase to replace lost blood volume and send food to damaged cells.

Stress Continuation
To heal damaged cell: It uses up its stored glucose. It will need to use
its stored carbohydrates, fat, and proteins Hypothalamus and adrenal glands – serve as
instructors a.Hypothalamus releases growth hormone
b.adrenal cortex releases cortisol *Both of these hormones tell the body to release
stored compounds from body fat, muscles, and the liver.

Hypothalamus indirectly orders adrenals to release cortisol via the corticotropin releasing hormone (CRH).
Why indirect? CRH goes to the pituitary gland sends the message on to the adrenals by releasing adrenocorticotropic hormone (ACTH)
When ACTH reaches the adrenals, the adrenal cortex releases cortisol into the blood. Cortisol makes the body release stored chemicals into the blood.
With ADH and aldosterone helping the body preserve blood volume, and cortisol and growth hormone providing food for the cells, the body should recover. But if this isn't enough help, the body could become exhausted and suffer organ damage.
Hypothalamic-pituitary-adrenal axis

Hypothalamic-pituitary-adrenal axis

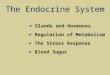
Flow Diagram of Stress Response

Stressors (stimulate)
Hypothalamus
•GRH
•GHRH
•TRH
Anterior Pituitary
•TSH
•hGH
•ACTH
Sympathetic centers in spinal cord
Sympathetic nerves
Adrenal medulla
Visceral factors
Epinephrine and norepinephrine
Stress responses (Fight-or-flight
responses)
ACTH
Adrenal cortex
Cortisol
hGH
Liver
IGFs
TSH
Thyroid gland
Thyroid hormones (T3 and T4)
Stress responses (Resistance reaction)
Key:
CRH=Corticotropin-releasing hormone ACTH=Adrenocorticotropic hormone GHRH=Growth hormone-releasing hormone hGH=Human growth hormone TRH=Thyrotropin-releasing hormone TSH=Thyroid-stimulating hormone

Major Hormone Changes DuringStress Response


Journals

Adrenal Insufficiency Vivian A. Fonseca, M.D.
Primary adrenal insufficiency is due to adrenal gland failure and thus both baseline and post stimulation concentrations are abnormal.
Secondary adrenal insufficiency is due to hypothalamic or pituitary failure and, in the acute setting, the adrenal glands respond well to stimulation while the baseline cortisol concentration is low.
(Clinical Endocrinology, March 2001)

The impact of the nonpeptide corticotropin-Releasing Hormone Antagonist Antalarmin on Behavioral and Endocrine Responses to Stress.
CRH is a 41-amino acid peptide initially identified as a hypothalamic factor responsible for stimulating ACTH from the anterior pituitary (1). Stressors induce the synthesis and release of CRH from cells of the paraventricular nucleus, into the portal blood, initiating the hypothalamopituitary-
adrenal (HPA) response to stressors. CRH isalso involved in the mediation of autonomic and behavioral sequelae of exposure to stressors.
The intracerebroventricular (icv) administration of CRH produces autonomic activation and many of the same behavioral, neurochemical, and electrophysiological alterations that are produced by stressors.
Furthermore, the icv administration of CRH antagonists, such as a helical CRH9–41 and D-Phe CRH, can blunt or block these stress-induced alterations in behavior and autonomic activity.
(Endocrine Society, April 1998)

Posttraumatic Inflammation Is a Complex Response Based on the Pathological Expression of the Nervous, Immune, and Endocrine Functional Systems M. A. Aller et al.
The nervous, immune and endocrine functional system integrates with each other to play important roles in local and systemic posttraumatic acute inflammatory response. In the nervous functional system, the phenomenon of ischemia-revascularization secondary to arteriolar vasomotor activity which involves vasoconstriction and vasodilatation would produce interstitial edema and permit selective cellular nutrition by diffusion.
(Medline Journals, October 2003)

What is injury?
damage or harm caused to the structure or function of the body caused by an outside agent or force, which may be physical or chemical.
-Medical Encyclopedia

INTRODUCTION
Accidental/Deliberate Injury
Series Of Changes At Site Of Injury & Within The Body
Generally
Restore The Body To Its Pre-injury Condition

FACTORS MEDIATING THE METABOLIC RESPOSE TO INJURY
ACUTE INFLAMMATORY RESPONSE -Inflammatory cells (macrophages, monocytes, neutrophils) -Proinflammatory cytokines & other inflammatory mediators
ENDOTHELIAL CELL ACTIVATION -Adhesion of inflammatory cells -Vasodilatation -Increased Permeability
AFFERENT NERVE STIMULATION
RELEASE OF STRESS HORMONES
BACTERIAL INFECTION&ENDOTOXIN

Endocrine response to injury
Main goal
to initiate reflexes that lead to the release of substances that are directed towards the restoration of the effective circulating volume and the delivery of critical energy substrates

Endocrine Response cont..
Activated by afferent neuronal impulses from the site of injury
These impulses travel along sensory nerve roots through the dorsal root of the spinal cord, up to the spinal cord to the medulla to activate the hypothalamus.
In 1950’s, it was postulated that there might be ‘wound hormones’ produced in the in injured tissues which activated the pituitary-adrenal axis

Neuro-endocrine response to injury
Phases of injuryStimuli for neuroendocrine reflexNeurohumural mediators of the
injury responseRequires an intact CNSPrincipal signal that starts NE
response are hypovolemia and painCytokines and other mediators

Phases of injury
Ebb phase-occurs immediately after injury with decrease in energy expenditure, reduction of effective circulating volume
Flow phase- (Early Anabolic Phase – period of compensation, increase in metabolic rate, restitution of blood volume, shift to anabolic pathway, wound healing period
Late Anabolic Phase

Stimuli for neuroendocrine reflex
Effective circulating volume- stimulates baroreceptor and stretch receptors, maximal NE response is when the effective circulating volume has been decreased by 30-40%, further decrease cannot be handled be compensatory systems, and shock follows
Decrease in oxygen, increase in carbon dioxide and hydrogen ions chemoreceptor activation causes an increase in heart rate and cardiac contractility.
Pain-NE response is not activated unless the neural pathways are intact

Stimuli for neuroendocrine reflex
EmotionDecrease in energy substrates,
particularly glucoseExtremes of temperature-changes in
core temperature activate NE pathwayWound-both sterile and dirty wounds
activate NE pathway through the action of inflammatory

Neuro-humoral mediation of the injury response
Requires an intact CNS Principal signal that starts the
neuroendocrine (NE) response are HYPOVOLEMIA AND PAIN
1.Autonomic and central nervous system
2.Hormonal

A. Hormone under the pituitary control
1.CRH (hypothalamus) – ACTH (anterior pituitary, Cortisol (adrenal cortex)
Persistent elevations of serum cortisol is associated with decreased survival
Secretion of cortisol is directly associated with magnitude of injury
Action of cortisolIncrease availability of glucosePotentiates the action of glucagons
and epinephrine Increases lipolysisDecrease the glucose intakeDecrease the action of insulin

2. TRH (hypothalamus) – TSH (anterior pituitary) – T3 and T4 (thyroid gland) – no significant increase
3. Growth hormone (hypothalamus) – promotes protein synthesis enhance breakdown of carbohydrate and lipid stores
4. Gonadotrophins (hypothalamus) and sex hormones – no significant increase

Arginine vasopressin (hypothalamus)
– formerly known as antidiuretic hormone, stimulated by changes in effective circulating volume.
Causes peripheral vasoconstrictionPreserves intravascular volume by
absorbing solute-free water in the distal tubules
Causes hepatic glycogenolysis

B. Hormones under autonomic control
1. Catecholamines – epinephrine (adrenal medulla) and norepinephrine (axon terminals of sympatheticpostganglionic neurons)
2. Aldosterone (adrenal medulla) – increase Na and Cl reabsorption.
- Secreted in response to angiotemsinogen II and
ACTH

3. Renin (renal afferent arterioles) – angiotensin (liver)
Renin activates angiotemsinogen into angiotensin which is then converted into angiotension II in the liver By the angiotensin converting enzyme
Potential vasoconstrictorIncreases cardiac contractility, increases
heart rate increases vascular permeability

4. Insulin (pancreas) – primary anabolic hormone, no significant increase
5. Glucagon (pancreas) –promotes hyperglycemia by stimulating hepatic glycogenolysis and gluconeogenesis
- promotes lypolysis and ketogenesis
6. Somatostatin (pancreas) – potent inhibitor of GH, TSH, insulin

7. Insulin like growth hormone –formerly known as somatomedins.
Stimulate proteoglycans synthesisIncrease hepatic protein synthesis
and glucose uptakePromote synthesis of skeletal muscle

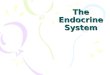
Endocrine Response to injurydiagram

Journals

The neuroendocrine response (NER) is an essential component of the adaptive process to trauma, brain injury, and
major surgery Chiolero R, et al.
While receiving additive humoral and neural afferent inputs, the brain nuclei responsible for the NER act mainly by efferent pathways to the hypothalamic-pituitary-adrenal (HPA) axis and the sympathoadrenal system, the activations of which induce subsequent circulatory and metabolic responses.
The outcome after brain injury is closely correlated with the intensity of these changes, particularly with catecholamine plasma levels and the severity of the low triiodothyronine syndrome.
Alterations of the thyroid hormones are largely related to a reduction in peripheral deiodination of thyroxin. Recent research shows that increased free-radical production and decreased selenium (an antioxidant) serum levels play an important role in thyroid metabolism.
(Endocrine Review, October 2004)

Hypopituitarism after traumatic brain injury Bondanelli Marta et al.
• Traumatic brain injury (TBI) is from an external mechanical insult on the cephalic area that can direct mechanical injury to pituitary gland, stalk or hypothalamus and can lead into temporary or permanent neurological dysfunction, resulting to impairment of cognitive, physical and psychosocial functions.
• Pituitary dysfunction can follow after a TBI and can be classified into two namely, functional alterations during the acute phase post-TBI, which result in a temporary increase or decrease in blood pituitary hormone concentrations, alterations in pituitary hormone secretion that may occur at any time after TBI, resulting in permanent hypopituitarism caused by damage at pituitary and/or hypothalamic level. Changes in the circulating hormone levels such as adrenocorticotropin (ACTH), prolactin (PRL) and growth hormone (GH) levels increase and luteinizing hormone (LH), follicle-stimulating hormone (FSH) and thyrotropin (TSH) levels may either decrease or remain unchanged, associated with a decreased activity of their target organ become apparent during the first hours or days after trauma, and may persist for the duration of the acute critical illness.
• (Medline, July 2001)

Growth hormone deficiency occurs in approximately 20% of all
individuals who suffer from a moderate to severe traumatic brain injury
This study shows that individuals with traumatic brain injury with normal GH secretion have below normal aerobic capacity and those patients who have GH insufficiency/deficiency are further deconditioned. Studies of GH replacement in these subjects should be conducted to assess whether GH therapy can improve cardiorespiratory fitness and prevent secondary disability.
(The Journal of Clinical Endocrinology & Metabolism, July 2008)

Sevoflurane improves the neuroendocrine stress response during laparoscopic pelvic surgery.
ACTH and cortisol are sensitive indicators of stress: plasma increase of ACTH and the subsequent increase of plasma cortisol are known to correlate with the severity of surgical injury.These hormones cause specific metabolic alterations (the best known is an increase of muscle catabolism, with net negative nitrogen balance), but also affect humoral and cellular immune responses)
(American Society of Anesthesiologist, July 2000)

Incidence of adrenal insufficiency after severe traumatic brain injury varies according to definition used: clinical implications Bernard Francis et al.
The stress response to surgery comprise a number of hormonal changes initiated by neuronal activation of the hypothalamic-pituitary-adrenal axis. The overall metabolic effect is one of catabolism of stored body fuels. In general, the magnitude and duration of the response are proportional to the surgical injury and development of complications such as sepsis. Other changes also occur following surgery, notably an increase in cytokine production which is triggered locally as a tissue response to injury.
Regional anaesthesia with local anaesthetic agents inhibits the stress response to surgery and can also influence postoperative outcome by beneficial effects on organ function.
(Medline, October, 2005)