Embed Size (px)
Citation preview
ECG Emergencies
October 1, 2014Melanie S. Sulistio, M.D., F.A.C.C.
UT SouthwesternInternal Medicine Core Lecture Series
Get yourselves down to the front of the lecture hall. You’ll want to, I promise. And I’ll call on anyone who
stays in the back….
Rules of Engagement
1. This is a competition
2. VA- sorry guys. But you won’t be blamed for the downfall of your compadres either…
3. Divide the room into 3 (left, center and right)
4. Raise hand w/ answer
5. Chiefs will determine who raises hand 1st
6. + Point for each correct answer, - point for any incorrect answer.
7. I am the FINAL judge for correct/incorrect answers. No arguing allowed (= deduction ).
Intern Level
• 57 y/o woman w/ breast cancer s/p chemo, DM2, HTN, HLP
• Presents to ED short of breath and feeling like her heart is racing
• Vitals: 95/50, HR 150, RR 30-35, O2 sat 88%
• Exam: elevated JVP, bibasilar crackles & intern cardiac exam (difficult heart sounds)
Answer the following questions…
1. What are your top 2 diagnoses?
A. Heart failure
B. Pericardial effusion/Tamponade
2. What else can you check on physical exam?
A. Kussmauls sign
B. Pulsus paradoxus
More Questions….
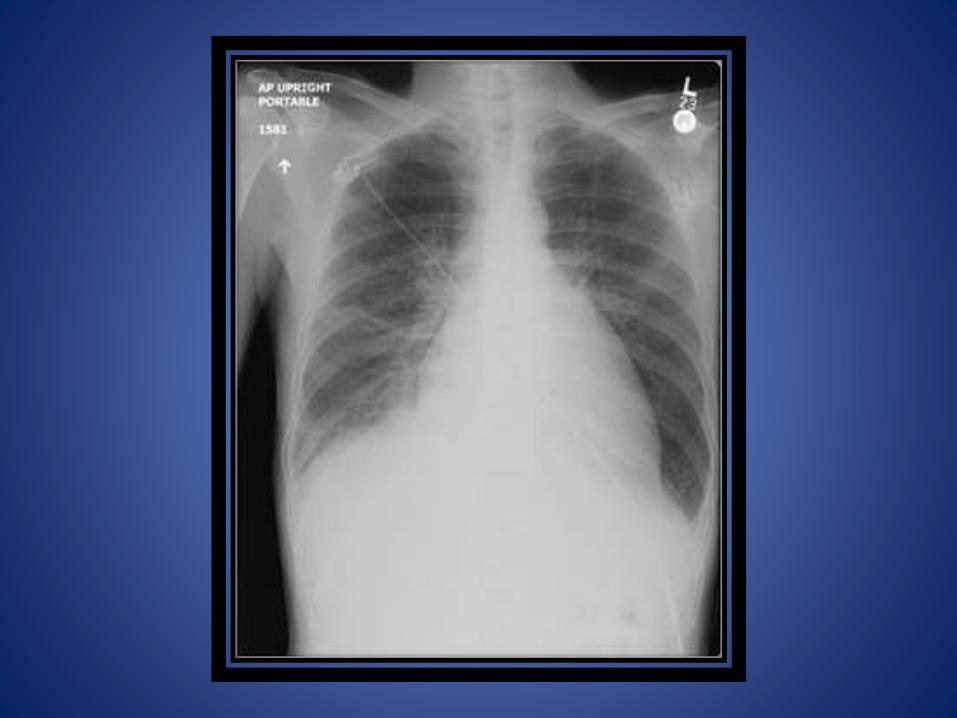
1. What other studies do you want?
A. Chest X-ray
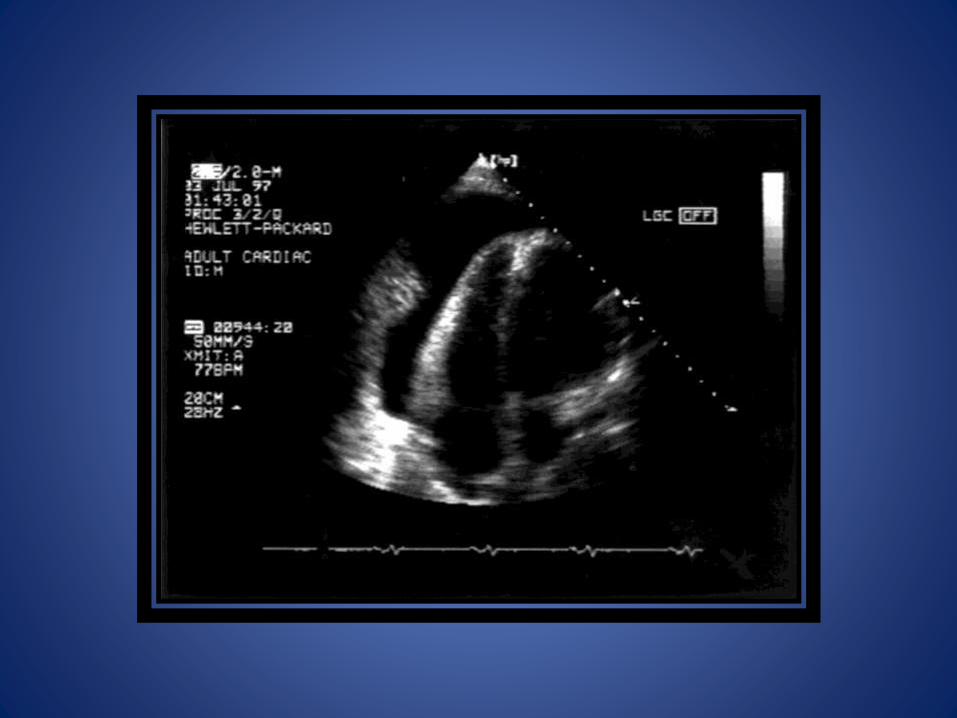
B. Echocardiogram
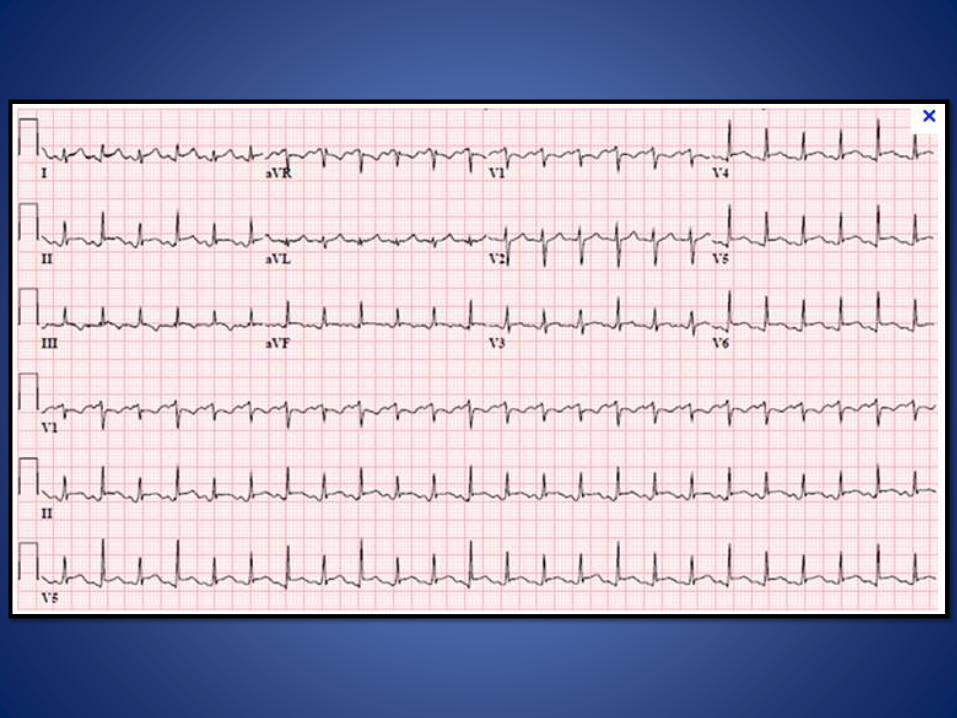
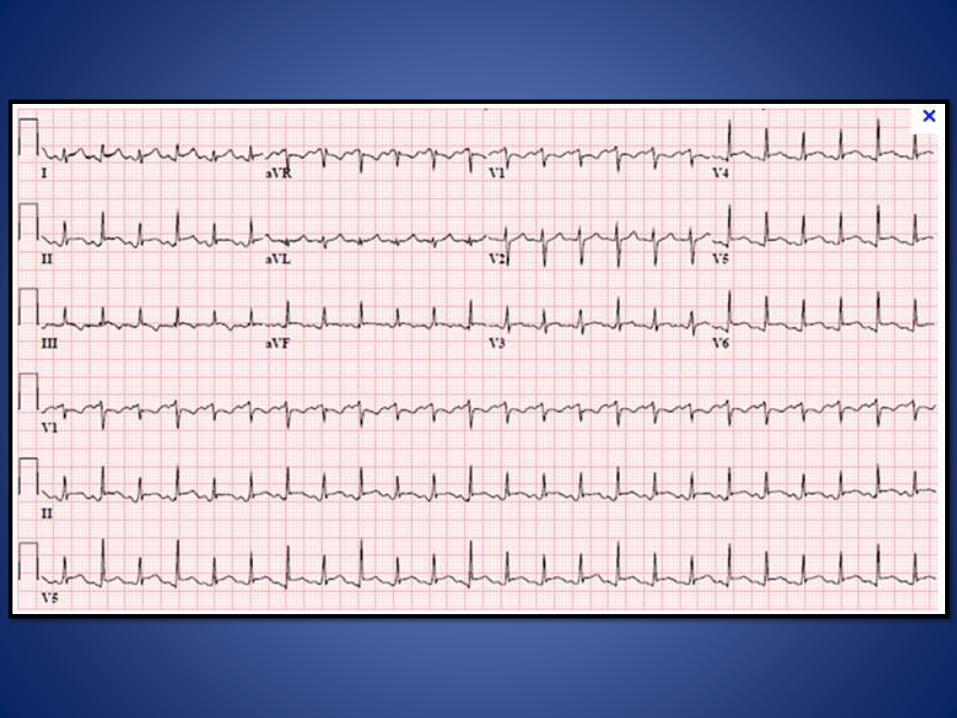
2. What findings on ECG are significant in this patient to help you?
More Questions….
1. What findings on ECG are significant in this patient to help you?
A. Electrical alternans
B. Sinus tachycardia
2. What is the final diagnosis?
A. Tamponade
Treatment questions…
1. How do you treat this patient’s hypotension?A. Volume, but can exacerbate her SOB
2. How do you treat this patient’s shortness of breath?A. Drain the effusion!
3. What steps would you take in the ED?A. Place patient on O2
B. Have fluid ready in case pt becomes symptomatically hypotensive
C. Call the CARDIOLOGY FELLOW!!!


• 27 y/o M with a history of an “SVT” comes in with severe dizziness and palpitations
• He has been seen by an outside cardiologist and started on a medicine, can’t remember the name
• Has felt ill with this med x 1 wk w/ associated poor appetite
• Vitals: HR 40-45 bpm, BP 100/70, RR normal
• PE: pale, appears unwell, conversant
2nd year Residents
Questions to answer
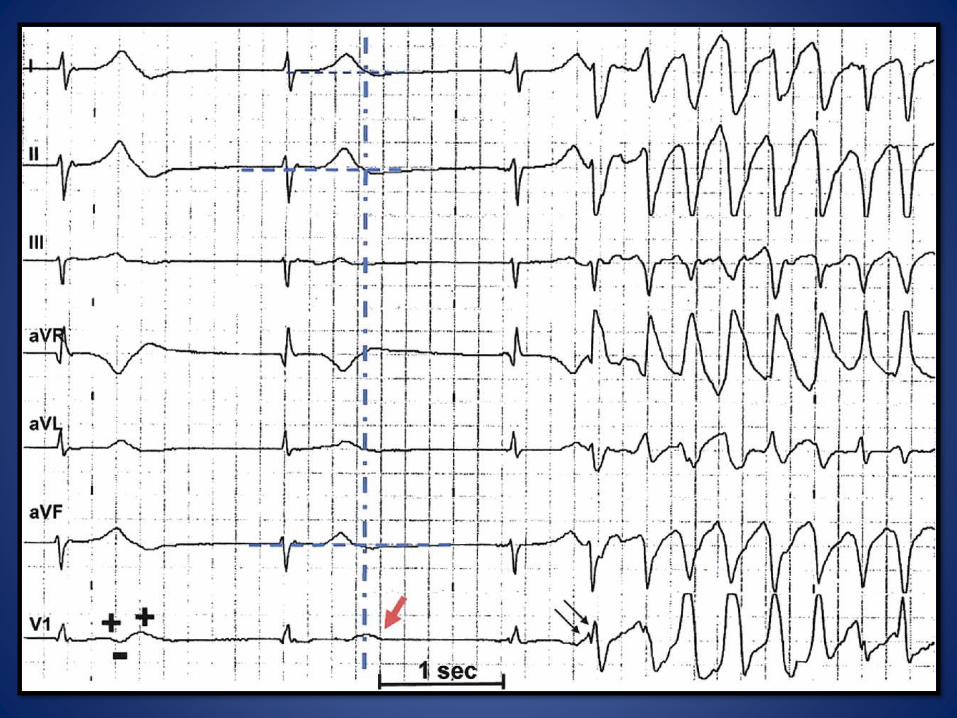
1. You (wisely) immediately request the defibrillator to be brought into the room.
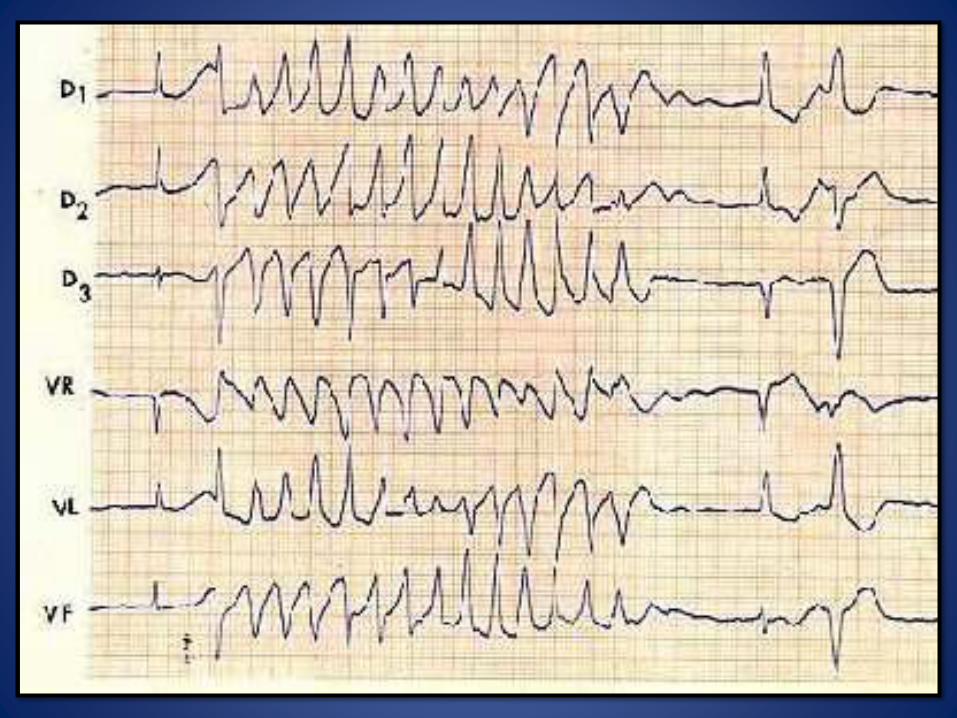
2. What is the rhythm?A. Torsades de pointes
3. True or False: Given how ill he is on presentation, I would immediately defibrillate.A. False, he’s having salvos- not persistent
4. What is the first med you ask the nurse for?A. Magnesium sulfate
5. How do you tell her to give it (dose/administration?) A. 2 grams iv push (if stable, can be given over 15 mins to
avoid hypotension)
Despite the MgSO4, he’s still having salvos.
1. What other med (continuous infusion) should you ask for? A. Isoproterenol (2 mcg/min, titrate for HR >110 bpm)
2. What other non-medicine option do you have?A. Transcutaneous pacing
3. What class of anti-arrhythmics predispose patients to TdP?A. Class III
4. BONUS! What channel do these affect?A. Potassium channel, IKr
Questions to answer
1. List 3 things that predispose you to develop TdP
A. Congenital Long QT
B. Bradycardia
C. QT prolonging drugs
D. Hypokalemia, hypomagnesemia & hypocalcemia
E. Underlying heart disease
F. Female sex
G. Advanced age
H. Recent conversion from AF
Questions to answer
Why did this patient have TdP?
• Underlying SVT
• Started on sotalol w/o inpt obs to chk QTc
• Became brady, felt sluggish & unwell ->
• Poor appetite -> hypovolemia & renal failure
• Increased sotalol levels, worsening QTc
• Also -> electrolyte disturbances, worsening QTc
• Combination of med, brady, e-lytes, renal failure = TdP
3rd year Residents
• 75 y/o WM pxs w/ feeling “like my head is drunk” w/ occasional falls
• PMH: HTN, HLP, tobacco use
• Vitals: 85/50, HR 30-40s, irregular, RR 13
• During eval in ED they hand you the ECG.
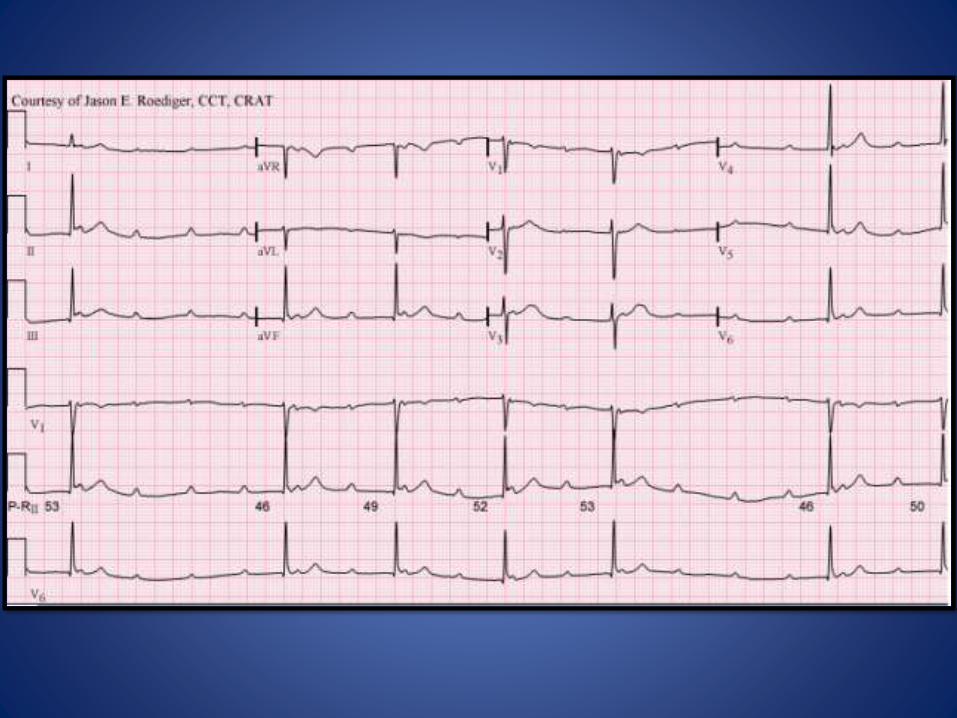
Questions to answer
1. What is the rhythm? (2 parts)A. Sinus tachycardiaB. High degree AV block
2. While looking at the ECG in the ED – you ask for what medications (2)?A. AtropineB. dopamine
3. What do you ask the nurse to do aside from getting the meds? A. Put pads on the patientB. Get the crash cart/defibrillator
BP drops to 70s/30s and pt says he feels he’s going to pass out
1. What dose of atropine to you give?A. 0.5 to 1 mg iv push
2. How do you hang the dopamine? A. 10-15 mcg/kg/min
3. Oh no, you can’t get IV access. What do you do next? A. Transcutaneous pace
Questions to answer
Questions to answer
1. What 2 things must you program on the defib/pacer?A. RateB. voltage
2. What heart rate do you set?A. 100 bpm or greater
3. What mV do you set? A. Whatever it takes to capture
4. How do you know when it captures (2 answers)?A. AuscultateB. Check the pulse/blood pressure response
5. True or false, you can NOT do chest compressions while someone is being paced transcutaneously. A. False
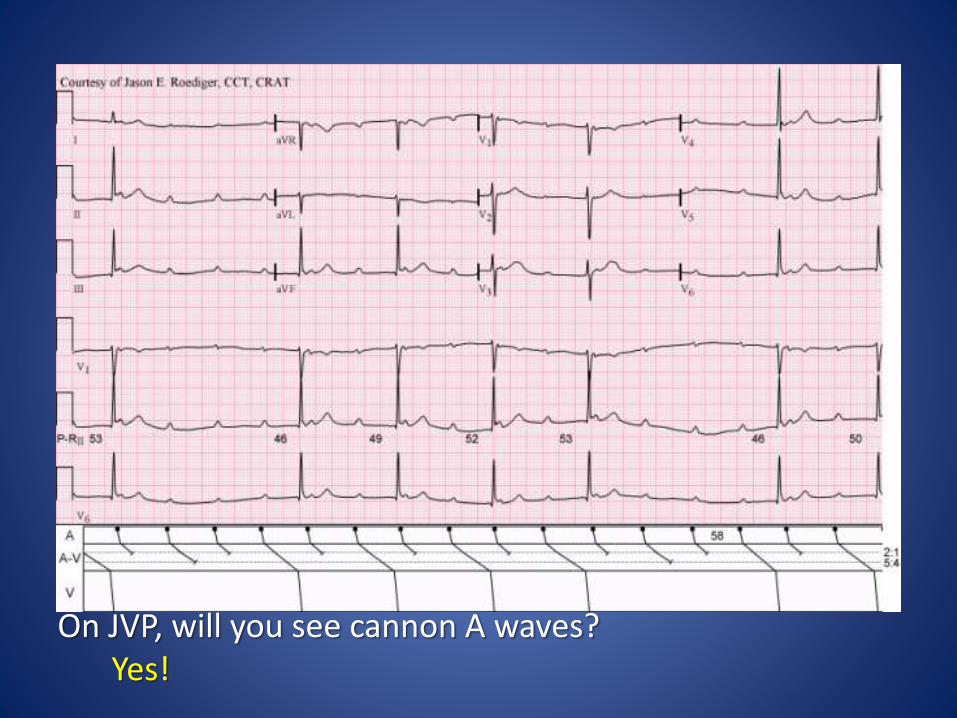
On JVP, will you see cannon A waves? Yes!
BONUS ROUND
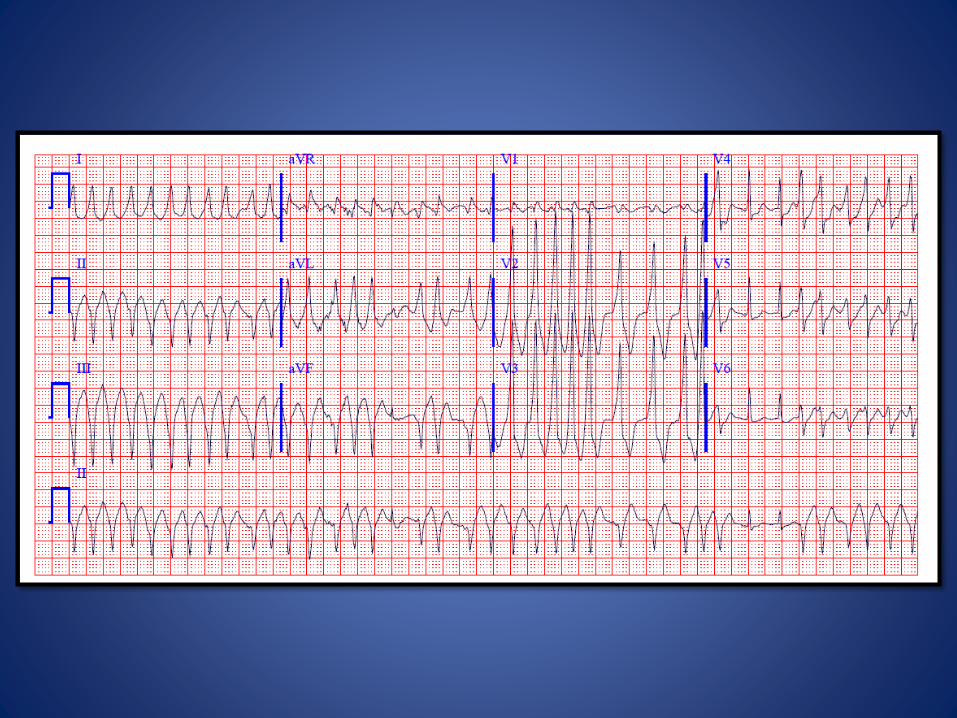
1. 67 y/o W presents w/ palpitations, feeling like her heart is racing
Questions
You have no prior ECGs and she has never been to our hospitals before (of course!).
1. What is the underlying rhythm? A. Atrial fibrillation
2. What medicine would you give and how?A. Procainamide, 50 mg/min OR 100 mg q5 mins
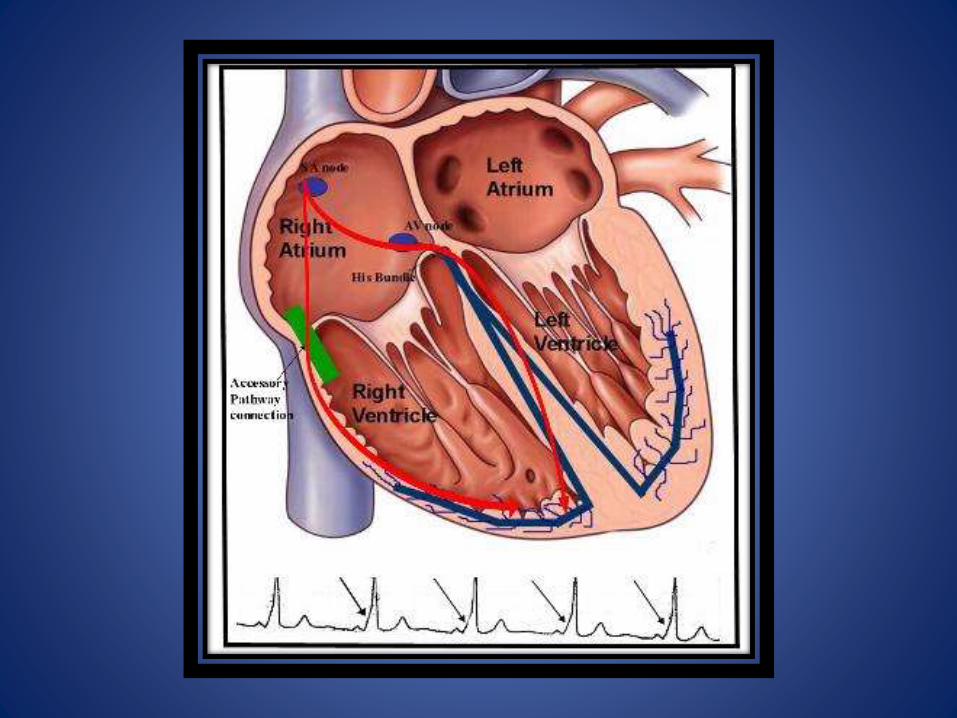
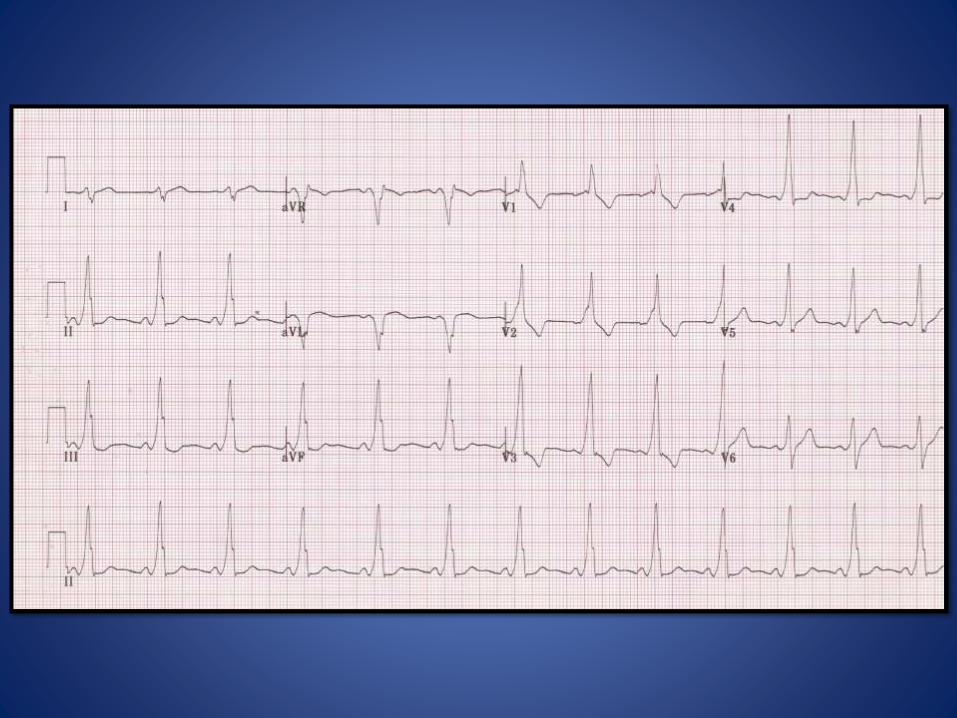
3. What would you suspect you would see on a an old ECG and why?A. Delta wave
B. Pt has WPW or AVRT
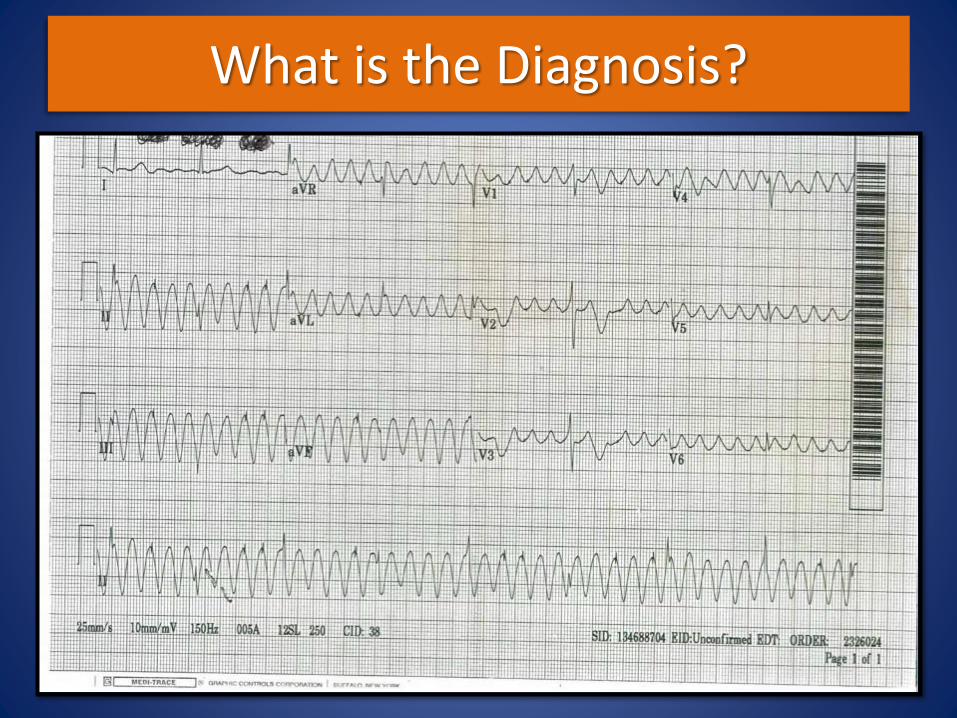
What is the Diagnosis?
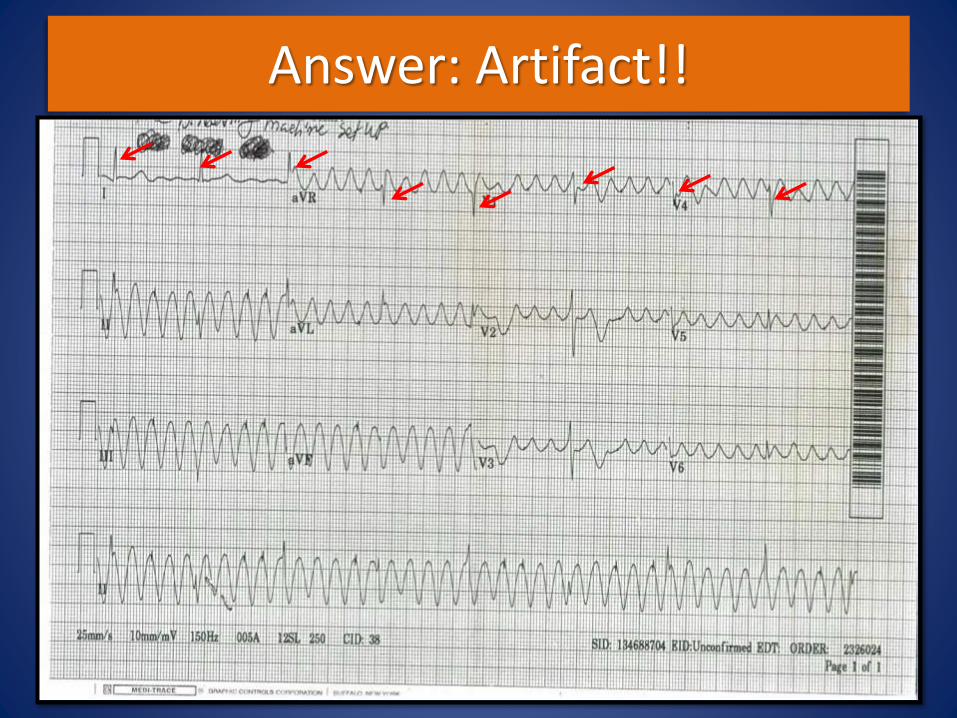
Answer: Artifact!!

We are UT Southwestern Medicine!
Interview datesOctober 24*November 7
November 14November 21December 5
December 12December 19
January 9January 16
January 23*
Happy Birthday Dr. Kazi!!!