Embed Size (px)
Citation preview

Prof P. Vijayaraghavan’s Unitby Dr J. Stalin Roy

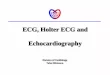
• Munirathinam 70 yr old male, a known Hypertensive came for routine check up.
• His pulse was regularly irregular, an ECG was ordered.



• Two foci of origin of atrial depolarisation as evidenced by two different p wave morphologies (the sinus p wave is + followed by – ie right atrial followed by left atrial; the ectopic p is – followed by + ie left atrial followed by right atrial)
• The sinus impulse is followed by an Atrial Premature Depolarisation (APD) which is coupled to the sinus impulse by a constant interval (0.48sec)
• The APD is followed by a normal ventricular depolarisation as evidenced by normal QRS
• This rhythm is known as Atrio-Ventricular Bigeminy or simply Atrial Bigeminy

Sinus impulse
• PR 0.12 sec
• QRS 0.10 sec
• QRS axis +30
• ST isoelectric
• T occasionally dented by the p wave of APD
APD
• PR 0.16 sec
• QRS 0.10 sec
• QRS axis +15
• ST isoelectric
• T normal


A P-wave algorithm constructed on the basis of findings from 130 atrial tachycardias correctly localized the focus in 93%

Right atrial
• A negative or biphasic (positive, then negative) P-wave in lead V1 was
associated with a 100% specificity and PPV for a tachycardia arising from the RA.
Left atrial
• A positive or biphasic (negative, then positive) P-wave in ECG lead V1 was associated with a 100% sensitivity and NPV for tachycardia originating in the LA.

• Lead V1 is oriented towards the right atrium, aVL towards the left atrium, so localization is mainly based on morphologies of p waves in these leads.
• Lead V1 is always positive when the impulse originates near the pulmonary veins (left atrial); and negative when the origin is near the tricuspid annulus (right atrial).
• In general, the polarity of leads II, III, aVF is deeply negative for an inferoanterior location, and low amplitude, positive, or biphasic for a superior location.
• Perinodal (near the AV node) and right septal foci are associated with an isoelectric V1.

• Rare rhythm disorder characterized by an APD occurring after each sinus impulse followed by a non-compensatory pause (characteristic of APD)
• The APD usually arises from a single irritable focus within the atria.
• An atrial or junctional focus becomes irritable due to:• Excess adrenaline due to increased sympathetic stimuli• Caffeine amphetamines, cocaine and other β1 receptor stimulants• Excess digitalis, certain toxins, occasionally ethanol• Hyperthyroidism • Stretch • Hypoxia

• Usually benign condition
• But it may rarely precipitate supraventricular and ventricular arrhythmias most commonly Atrial Fibrillation
• Management includes correction of predisposing conditions