Embed Size (px)
Citation preview

Treating MS beyond monotherapy
MS treatment history, current unmet needs
Prof. Gavin GiovannoniBarts and The London School of Medicine and Dentistry

Disclosures
Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design, trial steering committees and data and safety monitoring committees from: Abbvie, Actelion, Atara Bio, Almirall, Bayer-Schering Healthcare, Biogen, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma, Ironwood, Merck, Merck-Serono, Novartis, Pfizer, Roche, Sanofi-Aventis, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals.
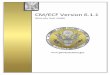
The therapeutic landscape
1994 1996 20001998 2002 2004 2006 2008 2010 2012 2014
SC IFN beta-1b1995 (RMS)
IM IFN beta-1a1997 (RMS)
SC IFN beta-1a 1998 (RMS)
Natalizumab2006 (RRMS)
Glatiramer acetate20 mg/mL
2003 (RMS)Fingolimod
2011 (RRMS)
Alemtuzumab2013 (RRMS)Teriflunomide 2013 (RRMS)
2016
Dimethyl fumarate2014 (RRMS)Peginterferon beta-1a2014 (RRMS)
Daclizumab2016 (RMS)
Glatiramer acetate40 mg/mL2015 (RMS)
Ocrelizumab2017 (RMS/PPMS)
Oral Cladribine2017 (RMS)
2018

Neuroaxonal loss & failure of recovery
Dis
abili
ty
Time
Acute relapse-associated
axonal damageDelayed
relapse-associated neurodegeneration
Post-inflammatoryneurodegeneration
Ageing
days-weeks months-years years-decades decades
reserve threshold
1
2
4
3

*
Therapeutic hierarchy
1. Smoking2. Exercise3. Diet4. Sleep5. Co-morbidities6. Infections7. Concomitant medications8. Menopause - HRT

Residual deficits:• Walking distance >500m• Unable to run • Exercise induces intermittent sensory
symptoms in L arm• Mild urinary frequency
17-yr girl, myelitisJun-2000
1st-yr University L-optic neuritis
Feb-2001
clumsy left hand
Jan -2002
pins & needles in legs
Oct-2003
R optic neuritisMar-2004
Brainstem syndrome; diplopia and ataxia
Dec 2007
Cervical cord relapseweak L arm with pain
Jan 2008
Bladder dysfunction
depression, anxiety and
fatigue
Reduced mobility
Mild urinary frequency
No depression ,anxiety or fatigue
Fully mobile
NEDA (no evident disease activity)Feb-2008 to May-2014
IFN-betaFeb-2001
Natalizumab
Jan-2008
ED
SS
IFN-beta NatalizumabJun-2000 Nov 2017
6.0
3.5 3.5
JCV positive - index 2.9
2014-Bridging fingolimod
pins & needles in legs
2015 - Alemtuzumab
2017 - Baby

Is this patient in long-term remission?

Residual deficits:• Walking distance >500m• Unable to run • Exercise induces intermittent sensory
symptoms in L arm• Mild urinary frequency
17-yr girl, myelitisJun-2000
1st-yr University L-optic neuritis
Feb-2001
clumsy left hand
Jan -2002
Oct-2003
R optic neuritisMar-2004
Brainstem syndrome; diplopia and ataxia
Dec 2007
Cervical cord relapseweak L arm with pain
Jan 2008
Bladder dysfunction
depression, anxiety and
fatigue
Reduced mobility
Mild urinary frequency
No depression ,anxiety or fatigue
Fully mobile
NEDA (no evident disease activity)
Feb-2008 to May-2014
IFN-beta
Feb-2001
Natalizumab
Jan-2008
ED
SS
IFN-beta NatalizumabJun-2000 Nov 2017
6.0
3.5 3.5
JCV positive - index 2.9
2014-Bridging fingolimod
pins & needles in legs
2015 - Alemtuzumab
2017 - Baby
✳ higher-efficacy
✳ neuroprotection
✳ safer
✳ anti-JCV
✳ remyelination
✳ neurorestoration
✳ unmet need
✳ comorbidities

Higher efficacy
Comparison of Switch to Fingolimod or Interferon Beta/Glatiramer Acetate in Active Multiple Sclerosis
He et al. JAMA Neurol. 2015;72(4):405-413.
Proportions of Patients Without Relapses in the Matched CohortsHR indicates hazard ratio.
Figure Legend:
Would interferon-beta, GA and fingolimod be more effective in combination than when used as a monotherapy?
✳ higher-efficacy

Reasoning by analogy
Crohn's Disease Rheumatoid Arthritis
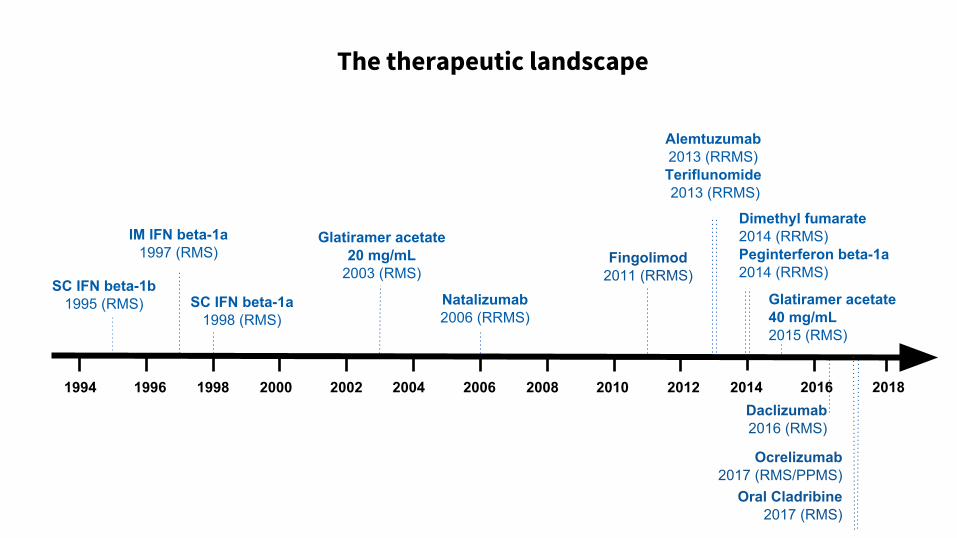
Phenytoin neuroprotection acute optic neuritis
Phenytoin
Participants with AON N=86
Phenytoin (4 mg/kg OD)
Placebo
Randomised within 2 wks of symptom
onset
Treatment period
3 months
Monitoring period
3 months
Primary outcome measures
Primary outcome measure: RNFL thickness
RNFL thickness Macular volume
1. Kapoor R et al. Presented at AAN; Washington, USA; 2015; 2. https://clinicaltrials.gov/ct2/show/NCT01451593;
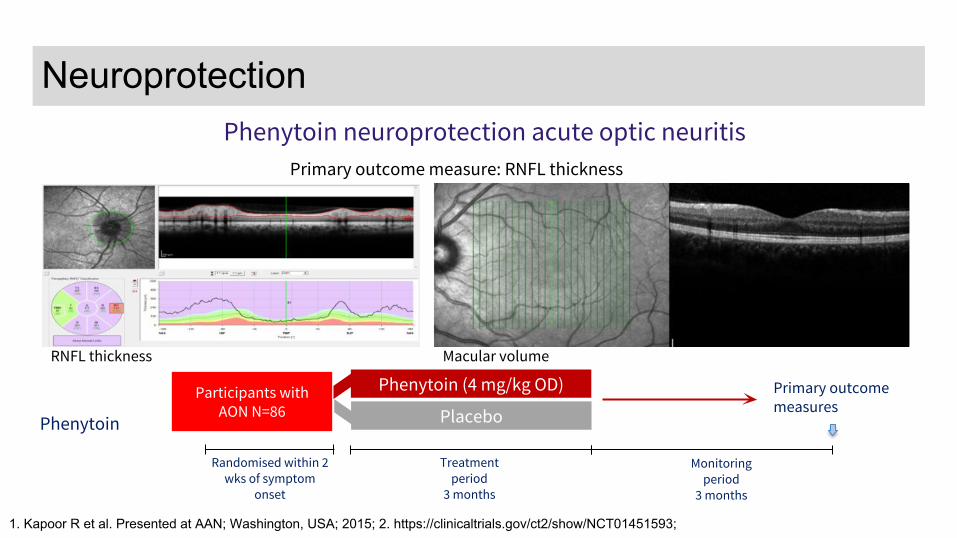
Neuroprotection
1. Kapoor R et al. Presented at AAN; Washington, USA; 2015; 2. https://clinicaltrials.gov/ct2/show/NCT01451593;
Neuroprotection
Should add-on protection become a standard of care in the management of MS?
✳ neuroprotection

*Adjusted for baseline characteristics.
13
Neuroprotection

Anti-JCV
I predict a future in which all patients who are JCV+ve are treated with an antiviral to clear them of the virus.
✳ anti-JCV

Alemtuzumab innate immunodeficiency
VZV TB Listeria Nocardia
Molluscum HPVCMV EBV
PCP Etc...
Thomas et al. Neurol Neuroimmunol Neuroinflamm 2016;3:e228;
AVN
AAN 2017, Boston
InnateImmunity
AdaptiveImmunity
AVN = avsacular necrosis, HPV = human papiloma virus, PCP = Pneumocystis carinii pneumonia, VZV = varicalle zoster virus
Safer
Combination of antiviral and antibacterial prophylaxis
✳ safer

Nogo, MAG, OMgP
Lingo-1-NgR-p75NTR
GAP-43
NCAM
Neuregulin
Agents in development or completed PoC trials:
1. Benztropine: anticholinergic
2. Opicinumab: anti-LINGO-1
3. Clemastine: anti-histamine/anti-cholinergi (M3)
4. GSK239512: histamine H3 receptor antagonist
5. IRX4204 & bexarotene: RXR agonist
6. rHIgM22: oligodendrocyte target
7. VX15: anti-SEMA4D
8. MD1003 (High-dose biotin): myelin biosynthesis
9. Elezanumab (ABT-555): anti-RGMa
Figure courtesy of Sharmilee Gnanapavan
Remyelination
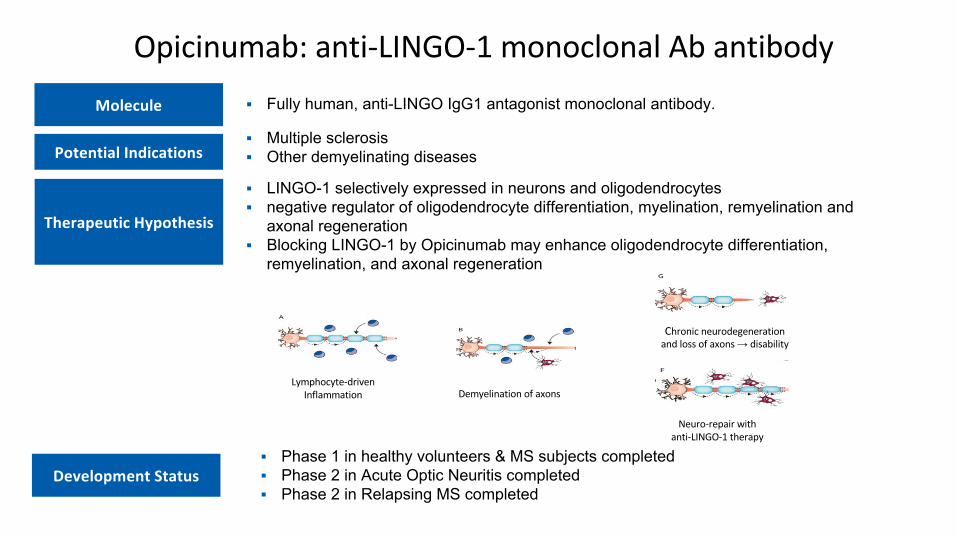
▪ Fully human, anti-LINGO IgG1 antagonist monoclonal antibody.
▪ Phase 1 in healthy volunteers & MS subjects completed ▪ Phase 2 in Acute Optic Neuritis completed ▪ Phase 2 in Relapsing MS completed
▪ Multiple sclerosis▪ Other demyelinating diseases
▪ LINGO-1 selectively expressed in neurons and oligodendrocytes▪ negative regulator of oligodendrocyte differentiation, myelination, remyelination and
axonal regeneration▪ Blocking LINGO-1 by Opicinumab may enhance oligodendrocyte differentiation,
remyelination, and axonal regeneration
→

Safety and efficacy of opicinumab in acute optic neuritis (RENEW): a randomised, placebo-controlled, phase 2 trial.
Cadavid et al. Lancet Neurol. 2017 Mar;16(3):189-199.
RENEW1,2
Anti-LINGO-1(multi-centre)
Anti-LINGO-1 (100 mg/kg IV Q4W x 6)
Placebo (IV Q4W x 6)Participants with first episode of
unilateral AON (n=82)
Randomised within 4 weeks of symptom onset
Dosing period20 weeks
Assessments at24 and 32 weeks
3–5 days’ IV steroids
EoS follow-up 32 weeksPrimary outcome: VEP

Opicinumab - Estimated Overall Response Scores (± SE)
Larger and more durable treatment effect over 72 weeks demonstrated in a post hoc subpopulation defined by disease duration and baseline brain MTR & DTI-RD
SYNERGY efficacy population Post hoc subpopulationPlacebo (n = 91)10 mg/kg opicinumab (n = 94)
Placebo (n = 25) 10 mg/kg opicinumab (n = 21)
Ove
rall
resp
onse
sco
re (±
SE
)
Weeks Weeks
Sheikh S, et al., Poster Session 1, P718, MSParis2017

All MD1003Placebo-controlled
p=0.014*
n=42
n=91
n=82
n=41
*Mann-Whitney U test months
24-month-treatment with-MD1003 (high doses of biotin) in progressive multiple sclerosis: results of the MS-SPI trial extension phase
Tourbah, et al. AAN 2016
24-mth treatment with MD1003 (high-dose biotin) in progressive MS: MS-SPI trial ext. phase
Mean change in EDSS from baseline
Which patients will benefit from add-on remyelination therapies?
✳ remyelination

*
Axonal sproutingAxonal modelling Synaptogenesis Cortical Plasticity
Kerschensteiner et al. J Exp Med. 2004;200(8):1027-38.
Waxman. Nat Rev Neurosci. 2006;7(12):932-41.
Stampanoni et al. Mult Scler. 2017 Jul doi: 10.1177/1352458517721358.
Neurorestoration

Co-morbidities
Combination therapy with a cocktail of drugs targeting MS-related comorbidities.
✳ comorbidities
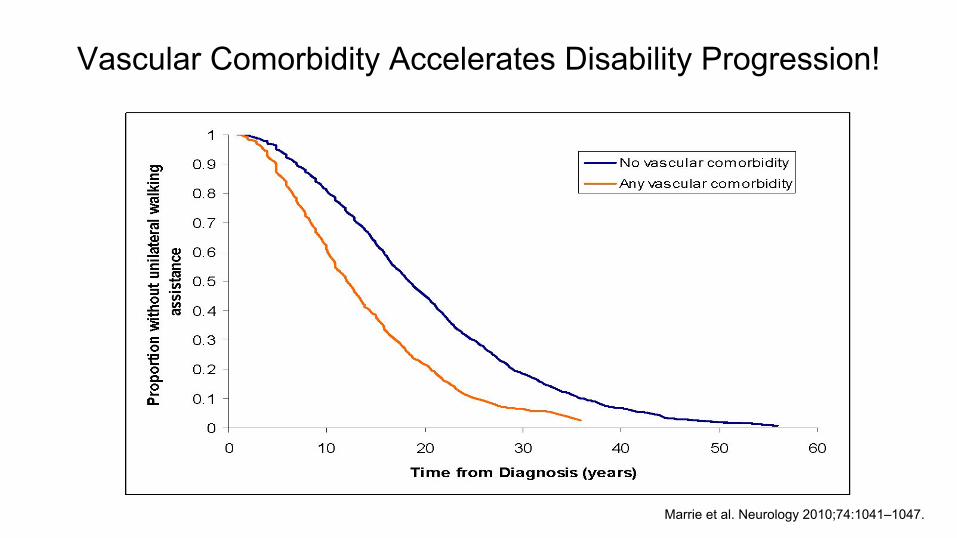
Vascular Comorbidity Accelerates Disability Progression!
Marrie et al. Neurology 2010;74:1041–1047.
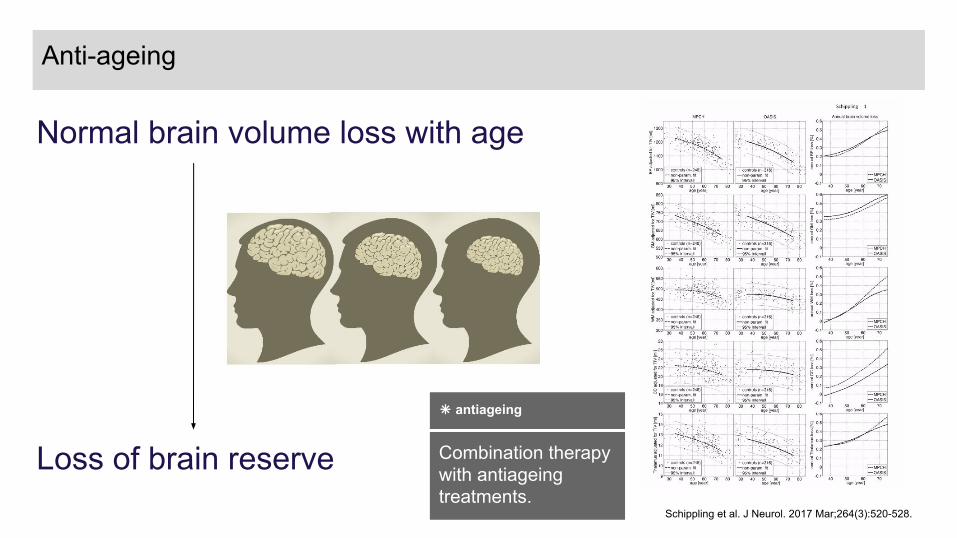
Normal brain volume loss with age
Loss of brain reserve Schippling et al. J Neurol. 2017 Mar;264(3):520-528.
Anti-ageing
Combination therapy with antiageing treatments.
✳ antiageing

Optimising MS managementD
isab
ility
Time
Acute relapse-associated
axonal damageDelayed
relapse-associated neurodegeneration
Post-inflammatoryneurodegeneration
Ageing
days-weeks months-years years-decades decades
reserve threshold
1
2
Acute neuroprotection Remyelination
Chronic neuroprotectionAnti-ageingAnti-inflammatory
4
3
✳ combination therapy

Residual deficits:• Walking distance >500m• Unable to run • Exercise induces intermittent sensory
symptoms in L arm• Mild urinary frequency
17-yr girl, myelitisJun-2000
1st-yr University L-optic neuritis
Feb-2001
clumsy left hand
Jan -2002
Oct-2003
R optic neuritisMar-2004
Brainstem syndrome; diplopia and ataxia
Dec 2007
Cervical cord relapseweak L arm with pain
Jan 2008
Bladder dysfunction
depression, anxiety and
fatigue
Reduced mobility
Mild urinary frequency
No depression ,anxiety or fatigue
Fully mobile
NEDA (no evident disease activity)
Feb-2008 to May-2014
IFN-beta
Feb-2001
Natalizumab
Jan-2008
ED
SS
IFN-beta NatalizumabJun-2000 Nov 2017
6.0
3.5 3.5
JCV positive - index 2.9
2014-Bridging fingolimod
pins & needles in legs
2015 - Alemtuzumab
2017 - Baby
✳ higher-efficacy
✳ neuroprotection
✳ safer
✳ anti-JCV
✳ remyelination
✳ neurorestoration
✳ unmet need
✳ comorbidities

*
1. Smoking2. Exercise3. Diet4. Sleep5. Co-morbidities6. Infections7. Concomitant medications8. Menopause - HRT
Therapeutic hierarchy
n...,2 ,1

Conclusions
∙ MS is a complex disease
– Multiple immunological and cellular targets
– Combination therapies makes sense (complementary modes of action)
– Adopt strategies from other disease areas, e.g. rheumatology, gastroenterology, transplantation and oncology
∙ Biology underlying the recovery of function is complex and involve many biological processes
– Synaptic
– Axonal
– Cortical
– Interacts with systems biology (ageing, comorbidities, concomitant medications, exercise and lifestyle factors)
∙ Can we afford not develop combination therapies?
✳ higher-efficacy ✳ neuroprotection
✳ safer
✳ anti-JCV
✳ remyelination
✳ neurorestoration
✳ unmet need
Addressed by combination therapies
✳ comorbidities
✳ ageing