Embed Size (px)
Citation preview

Welcome to Fight Colorectal Cancer’s
Webinar:Stomach Stuffers: How to eat well and avoid
a bowel obstruction this holiday seasonMake Sure You Know the Latest News
About CRC Research and Treatment visit fightcrc.org
Our webinar will begin shortly.

Today’s Webinar:1. Today’s Speakers: Margaret Martin, RD, MS, LDN, CDE &
James D. Waller, Jr., MD
2. Archived Webinars: FightColorectalCancer.org/Webinars
3. AFTER THE WEBINAR: expect an email with links to the
material. Also a survey on how we did, receive a Blue Star pin
when completed
4. Ask a question in the panel on the RIGHT SIDE of your screen
5. Follow along via Twitter – use the hashtag #CRCWebinar

Introducing our much acclaimed:
Patient Resource Guide

Funding Science
Established in 2006, our Lisa Fund has
raised hundreds of thousands of dollars
to directly support the innovative research
in treating late-stage colorectal cancer.
100% of the funds donated go
directly to Late-stage colorectal
cancer research.
Learn more or donate:
FightColorectalCancer.org/LisaFund

DisclaimerThe information and services provided by Fight Colorectal
Cancer are for general informational purposes only. The
information and services are not intended to be
substitutes for professional medical advice, diagnoses, or
treatment.
If you are ill, or suspect that you are ill, see a doctor
immediately. In an emergency, call 911 or go to the
nearest emergency room.
Fight Colorectal Cancer never recommends or endorses
any specific physicians, products or treatments for any
condition.
SpeakerMargaret Martin, RD, MS, LDN, CDE is a Licensed Dietitian and Nutritionist in the
State of Tennessee as well as a Certified
Diabetes Educator. Margaret graduated from
the University of Alabama with a Bachelor of
Science in Dietetics and received her
Master’s Degree in Nutrition Science & Public Health from the
University of Tennessee. With more than 10 years of experience in
Clinical Nutrition, Margaret has also worked in the insurance
industry with WellPoint Inc. and Blue Cross Blue Shield providing
telephonic nutrition consultations, service assistance, and web-
based nutrition education. In her free time Margaret volunteers
with the American Lung Association’s annual “Lung Force Walk" in
Middle Tennessee.

PearlPoint Cancer Support• Our Mission: To create a more
confident cancer journey for adults
anytime, anywhere
• Provide personalized guidance,
education, and support through My
PearlPoint (mypearlpoint.org)
• Focus on patients and family
members dealing a cancer
diagnosis and subsequent
treatment
• Personalized services from the
moment of diagnosis, free of
charge
12/9/2014 7

Nutrition Tips for Colorectal Surgery
Objectives
• The Colon’s Job
• Nutrition Steps to Know
• Holiday Tips to Avoid obstruction
8

Nutrition & The Healthy Colon
The colon is your body’s food & nutrition workhorse. What does the colon do?
• Finishes the final step of digestion
• Absorbs nutrients and fluids
• Balances nutrition for life and immunity
• Prepares waste for elimination
9

Nutrition and Colorectal Cancer
• Colorectal cancer & surgery may trigger digestive issues.
• Digestive issues such as diarrhea, constipation, gas, & bowel obstruction can trigger malnutrition.
• Digestive issues are treatable! – Start the conversation with your healthcare
team– Share your “Side Effects Log”
10

Fortify Before Surgery
• Grab nutrient-rich foods
• Stir in extra protein sources
• Sip on supplemental liquids
• Follow your surgeon’s pre-op instructions
11

Fortify Before Surgery
• Choose nutrient-richfoods with iron, protein, vitamins, etc.
• Look on Nutrition Facts labels for % Daily Values
5% or less=LOW20% or more=HIGH
12

Fortify Before Surgery
• Stir extra nutrition into hot
cereals, gelatins, beverages,
soups, creamy items,
or casseroles.
• For example:
– egg whites powder
– dry milk powder
– commercial protein powders
– liquid daily multivitamin
13

Nutrition after Surgery
• Give your colon time to heal
• There is not just ONE post-op meal plan
• Surgeon or registered dietitian will prescribe your nutrition plan
• Nutrition plan progresses over time from ice chips to solid foods
14

Nutrition After Surgery
Tips to Avoid Obstruction:
• Ask for printed meal plan
• Meet with registered dietitian
• Drink fluids as prescribed– Ice chips
– Clear liquids such as apple, cranberry, or cherry juices
– Gelatins, decaf tea, soft drinks, coffee
– Full liquids such as milk, soup, ice cream, or yogurt
15
Nutrition After Surgery
Eat small, frequent mini-meals
• Go small
– Small meals give your colon an easier job
• Choose fuel
– Frequent nutrition fights fatigue & mood swings
• Drink up
– Aim for 10-12 ounces every 3-4hrs
16

Nutrition After Surgery
Types of Fiber• Soluble Fiber thickens the stool
• Insoluble Fiber gives bulk
• Spread fiber intake throughout the day
17

Nutrition After Surgery
Watch Fiber Intake • Know which foods and drinks contain fiber
• Low-fiber means less than 0.5 to 2 grams per serving and less than 13 grams daily
• Low fiber = low-stress digestion which helps speed healing
• High-fiber sources include nuts, seeds, pulp, peels. Avoid these.
18

Nutrition After Surgery
Good Low-fiber foods • Juices with no pulp or seeds• Cooked veggies with no strings, peels, seeds• White bread, plain bagels, crackers with < 2 grams fiber• Cooked and cold cereals <3grams fiber• Plain noodles, pasta, white rice• Skinless potatoes • Bananas• Canned fruits, seedless in light syrup• Cooked meat, fish, and eggs• Broths and soups made with OK items• Angel food cake, frozen yogurt, pudding, ices
19

Holiday Tips To Avoid Obstruction
• Choose low fiber
• Hydrate thru the day with 64 ounces +
• Eat every 3-4 hours
• Enjoy what you eat
• Review your food intake log for any issues
• Seek help for meal plan, cooking & shopping
20
Holiday Tips to Avoid Obstruction
• Take good posture
• Off the high risk foods—nuts, strings,
peels, seeds, stalks, whole grains, etc.
• Avoid spicy foods, gassy foods, gum, & straws
• Set goals to get active-start 5 minute walk
• Trim alcoholic and caffeinated beverages
21

For more resources to help you navigate your cancer journey, sign up for a free dashboard on My PearlPoint at mypearlpoint.org.
22

For more tips managing nutrition side effects, download our free Cancer Side Effects Helper mobile app from Google Play or iTunes.
23
Additional Resources
• www.MyPearlPoint.org
• www.FightColorectalCancer.org
• www.cancer.gov
• www.cancer.org/Low-FiberFoods
• www.OncologyNutrition.org
• www.AICR.org
24

SpeakerJames D. Waller, Jr., MD is a
native of Evansville, Indiana. He
attended medical school at Indiana
University and completed his internship
at Methodist Hospital in Indianapolis.
His residencies in general surgery and
colorectal surgery were in Michigan at Butterworth Hospital
and Ferguson Hospital respectively. Dr. Waller is board-
certified by the American Board of Surgery and the American
Board of Colon and Rectal Surgery. In 1986, Dr. Waller
joined Dr. Krystosek in practice at Ohio Valley Colon and
Rectal Surgeons. Outside the office, he enjoys playing ice
hockey and softball.

12/9/2014 26
James D. Waller, M.D.
Ohio ValleyColon &Rectal Surgeons
801 St. Mary’s Drive, 200 WestEvansville, IN 47714(812) 477-6103 ● (800) 371-1169www.colonsurgeons.com


DIGESTIVE CARE CENTER
12/9/2014 28
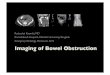
Bowel Obstruction
Small bowel
Colon

Obstruction
Small bowel obstruction more common
Colon cancer most common cause of colonoic
obstruction
Colon cancer obstructing in only 2-3% of cases

Small Bowel Obstruction
Complete or partial occlusion of the intestinal
lumen
Adhesions in 60%
Cancer in 20%
Hernia in 10%
Inflammation 5%, Crohn’s, diverticulitis, abcess

Adhesions
Can occur after any surgery
More common with extensive or multiple
surgeries
Worse with pelvic or colon surgeries
Obstruction occurs with torsion/twisting of
bowel (garden hose)
This reults in kinking of the bowel and possible
compromise of the blood supply

Tumors
Metastatic cancers are most common
Small bowel cancers are rare
Intra-abdominal:
ovaries/pancreatic/stomach/colon
Extra abdominal: lung/breast/melanoma
Obstruction caused by direct
compression/invasion or twisting

Hernia
Entrapment of bowel within the hernia
Compression/twisting and possible restriction
of blood flow
Inflammation
Crohn’s disease
Ulcerative colitis
Diverticulitis

Majority of Obstructions
Adhesions with twisting or entrapment of the
bowel
Involving the small bowel
Even in patients with a history of colon cancer!!

Clinical presentation
Crampy abdominal pain
Abdominal distension
Nausea and vomitting
Obstipation (no stool or gas )
Loose frequent stool/diarrhea with partial
obstruction!

Evaluation
Exam
-abdominal distension
-pain
-hyperactive bowel sounds
-scars
-herniae

Evaluation
Plain abdominal Xray- Upright KUB
CT scan
Barium study when intermittent or partial
CBC, CMP, EKG, UA

Treatment
IV fluid support
Tube ( NG ) decompression
Surgery when indicated

Medical Tx
Monitor closely… vitals, urine output, exam
Over 50% will resolve with medical treatment

Surgery
If no improvement in 24-48 hours
Deterioration
Any sign of acute abdomen
Negative exploration is sometimes better than
waiting!
Surgery
Laparoscopic approach sometimes possible
Simple lysis of adhesion in most cases
Reduction repair of herniae
Bowel resection if not viable
Bypass or resection if cancer or radiation
Resection or stricturoplasty in Crohn’s
Resection of sigmoid if diverticular

Special cases
Early post op
History of multiple surgeries for obstruction
Metastatic disease
Radiation
Colon Cancer Patients
15% or greater lifetime risk of obstruction
? Less risk with laparoscopic resection
Partial obstruction can occur with anastomotic
strictures
Radiation induced strictures
Ostomy can represent an area of partial
obstruction

Prevention
No proven method of prevention
Minimize ‘injury’ of surgery
Not caused by diet or activities

Summary
Most obstructions caused by adhesions
At least a 15% risk after colon resection
Most respond to conservative treatment
Surgery for those who do not improve or
present with incarcerated hernia or acute
abdomen

Question & Answer Time . . .
DONATE $10 NOW on your mobile.
Text “FCRC” to 501501
(A $10 donation to Fight Colorectal Cancer will be deducted from your cell phone bill. Message rates apply.)
BECOME AN ADVOCATE.Learn more at FightColorectalCancer.org/Advocacy
How can YOU help? Join us.

Contact UsFight Colorectal Cancer
1414 Prince Street, Suite 204
Alexandria, VA 22314
(703) 548-1225
Resource Line: 1-877-427-2111
www.FightColorectalCancer.org
facebook.com/FightCRC
twitter.com/FightCRC
youtube.com/FightCRC
pinterest.com/FightCRC