Embed Size (px)
DESCRIPTION
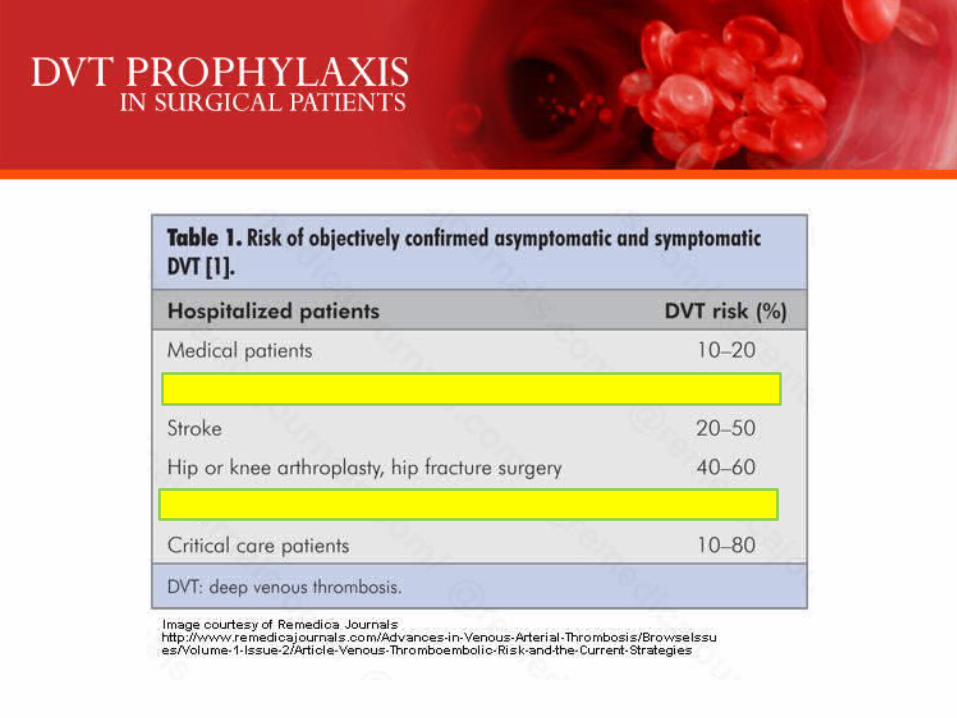
Key Points : Venous thromboembolic “is the most common cause of potentially preventable death in the surgical patient .” Clinical diagnosis is challenging, and providers should utilize risk assessment tools to aid in determining which patients should undergo additional imaging studies. The vast majority of patients with venous thromboembolism can be treated with standard therapy. Operative intervention should be considered in all patients with ileofemoral thrombosis who have symptoms lasting less than 14 days, low bleeding risk, and adequate life expectancy. DVT Prophylaxis : Although as many as 64% of surgical patients are at risk for developing venous thromboembolism only 59% of these patients receive thromboprophylaxis. 25 Individual risk assessment for the development of venous thromboembolism for both surgical and nonsurgical patients can be achieved by utilizing the Caprini Risk Assessment Model (RAM), which has been validated in a large retrospective trial of general, vascular, and urological surgery patients . Based on this score, risk of VTE can be estimated, and appropriate prophylaxis can be initiated.
Citation preview
By: Dr. Anas Ahmed Bettamer
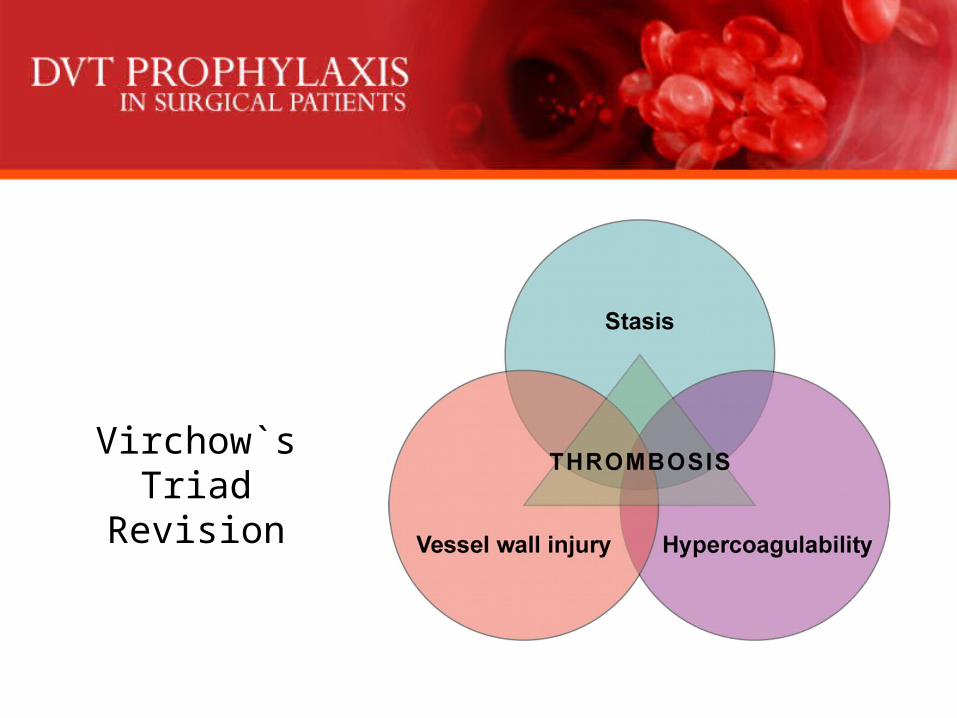
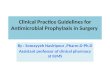
Virchow`s TriadRevision
Key Points :• Venous thromboembolic “is the most common cause of potentially preventable
death in the surgical patient .”
• Clinical diagnosis is challenging, and providers should utilize risk assessment tools to aid in determining which patients should undergo additional imaging studies.
• The vast majority of patients with venous thromboembolism can be treated with standard therapy.
• Operative intervention should be considered in all patients with ileofemoral thrombosis who have symptoms lasting less than 14 days, low bleeding risk, and adequate life expectancy.
• DVT Prophylaxis :– Although as many as 64% of surgical patients are at risk for developing
venous thromboembolism only 59% of these patients receive thromboprophylaxis.
– 25 Individual risk assessment for the development of venous thromboembolism for both surgical and nonsurgical patients can be achieved by utilizing the Caprini Risk Assessment Model (RAM), which has been validated in a large retrospective trial of general, vascular, and urological surgery patients . Based on this score, risk of VTE can be estimated, and appropriate prophylaxis can be initiated.
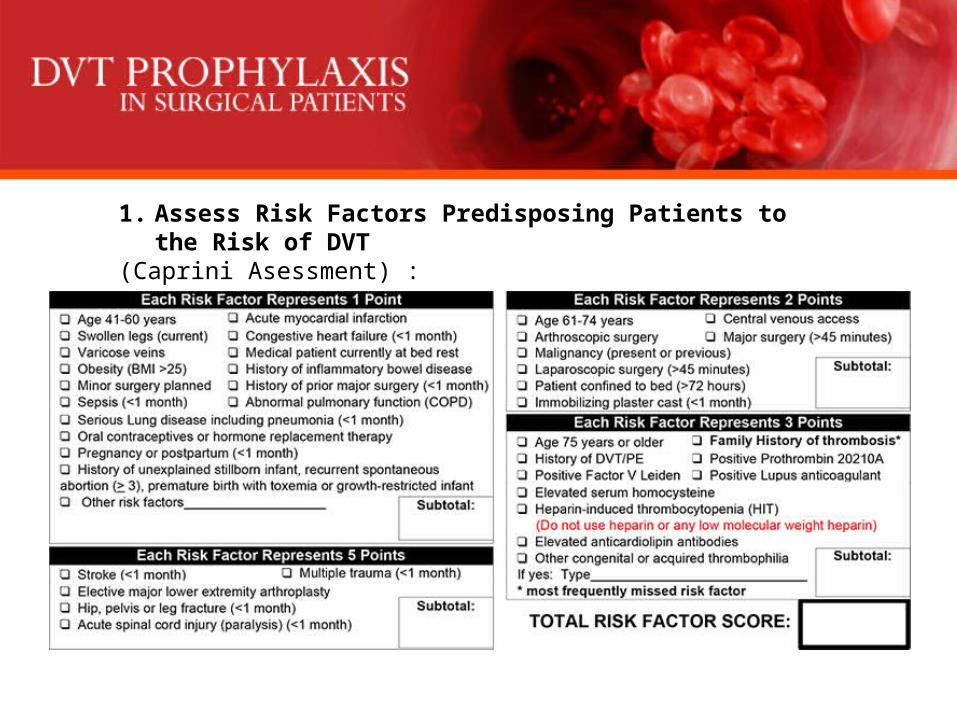
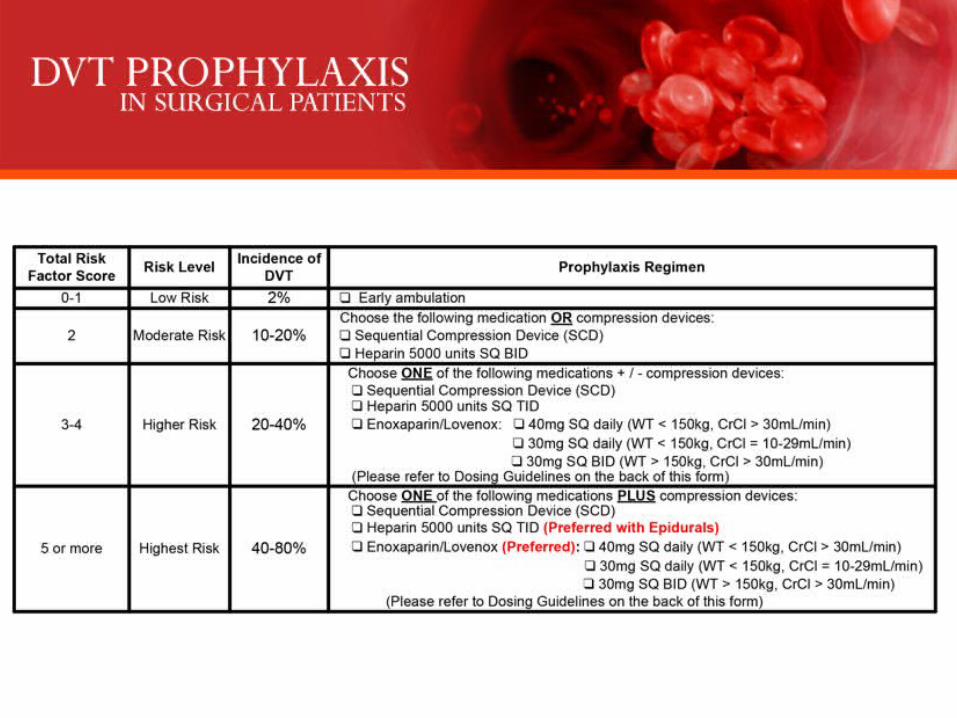
1. Assess Risk Factors Predisposing Patients to the Risk of DVT(Caprini Asessment) :
• Total Risk Factor score (0-1)– Low Risk (Incidence 2%)
• Uncomplicated minor surgery (general anesthesia < 30 minutes) in patients < 40 years old with no clinical risk factors.
– PROPHYLAXIS REGIMEN:• No specific prophylaxis other than early ambulation• May consider TED hose and/or Sequential Compression Devices
(SCD’s); from immediately before surgery until fully ambulatory.
• Total Risk Factor score (2)– Moderate Risk (Incidence 10-20%)
• ANY surgery (major or minor) in patients 40-60 years old with no additional risk factors
• Major surgery in patients < 40 years old with no additional risk factors• Minor surgery in patients with risk factors
– PROPHYLAXIS REGIMEN: • TED hose and/or SCD’s; start immediately before surgery and continue until
fully ambulatory AND/ OR• Heparin 5000 units s.c. q 12h (may start 1-2h before surgery) for 7 days or
until fully ambulatory OR• Dalteparin 2500 units q day for 5-10 days (may start 1-2h before surgery) OR• Enoxaparin 40mg q day or 30 mg q 12h for 7-10 days (may start 1-2h before
surgery)
• Total Risk Factor score (3-4)– High Risk (Incidence of DVT 20-40%)
• Major surgery in patients >60 years old with no additional risk factors• Major surgery in patients 40-60 years old with additional risk factors• Patients with MI
– PROPHYLAXIS REGIMEN -- Combination therapy: • TED hose and/or SCD’s – especially in patients prone to wound complications such as
hematomas or infections; start immediately before surgery and continue until fully ambulatory PLUS
• Heparin 5000 units s.c. q 8h or q 12h (may start 1-2h before surgery) for 7 days or until fully ambulatory OR
• Dalteparin 5000 units q day for 5-10 days (may start 10-12h before surgery) OR• Enoxaparin 40mg q day (or 30mg q 12h) for 7-10 days (may start 10-12h before surgery)
OR• Dextran 40 (in D5 or NS) 500 – 1000ml (5-7ml/kg) IV at 20-25ml/hr on the day of surgery
and 500ml (4-7ml/kg) daily at 20-25ml/hr for 2-3 days. then every 2 or 3 days for 2 weeks according to risk.
• Total Risk Factor score (5 or more)– Highest Risk (Incidence of DVT 40-80%)
• Major surgery in patients >40 years old with prior history of DVT, PE, cancer, or hypercoagulable state
– PROPHYLAXIS REGIMEN -- Combination therapy: • TED hose and/or SCD’s; start immediately before surgery and continue until fully
ambulatory PLUS• Heparin 5000 units s.c. q 8h (may start 1-2h before surgery) for 7 days or until
fully ambulatory OR• Dalteparin 5000 units q day for 5-10 days (may start the evening before surgery)
OR• Enoxaparin 40mg q day or 30mg q 12h for 7-10 days (may start 2h before
surgery) OR• Dextran 40 (in D5 or NS) 500 – 1000ml (5-7ml/kg) IV on the day of surgery and
500ml (4-7ml/kg) daily for 2-3 days. Then every 2 or 3 days for 2 wks according to risk OR)
• Consider IVC filter insertion in patients with high thromboembolic risk and sub-optimal prophylaxis, especially if proximal DVT is demonstrated and if anticoagulants are contraindicated OR
• Warfarin 5mg qd starting the day of or the day after surgery (adjust dose to keep INR between 2-3); consider referral to anticoagulation clinic.
--------------------------------Current CHEST guidelines recommend IVCF placement only in those who have contraindications to anticoagulation, and that anticoagulation should be initiated once bleeding resolves
• MULTIPLE TRAUMA SURGERY : in patients of all ages with an identifiable risk factor for thromboembolism
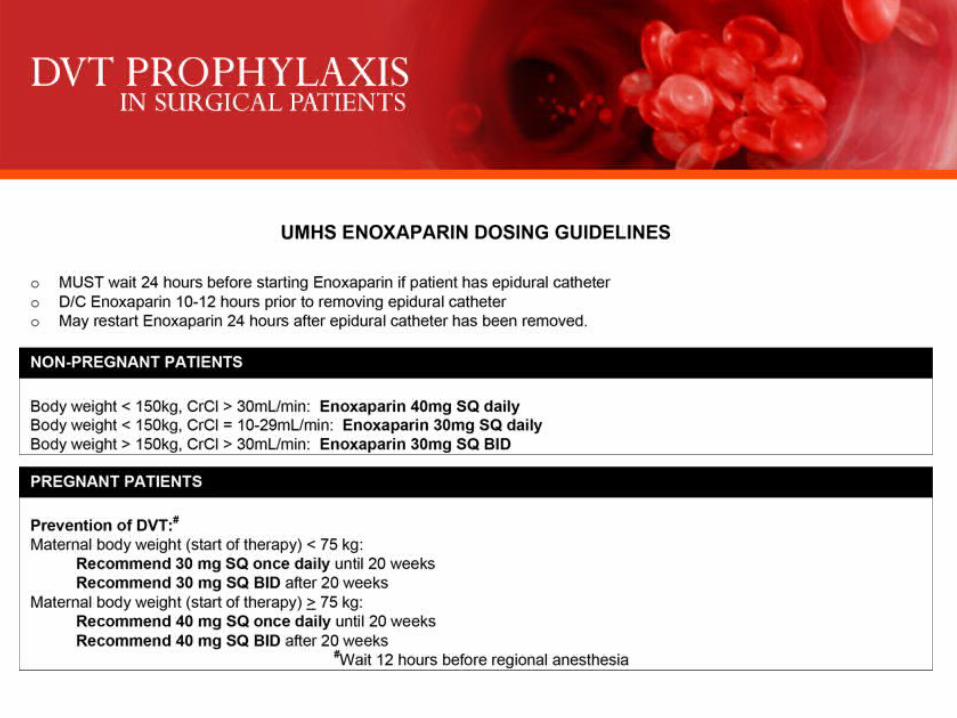
• PROPHYLAXIS REGIMEN– Unless contraindicated, start enoxaparin 30mg q12h as soon as it is considered safe to
do so (usually 12-36h after injury)– If enoxaparin is contraindicated or delayed, consider use of TED hose and/or SCD’s,
and/or foot pumps– Consider IVC filter insertion in patients with high thromboembolic risk and sub-optimal
prophylaxis, especially if proximal DVT is demonstrated and if anticoagulants are contraindicated
– Consider warfarin in patients with ongoing thromboembolic risks, if no major bleeding risk exists & no more surgery is required
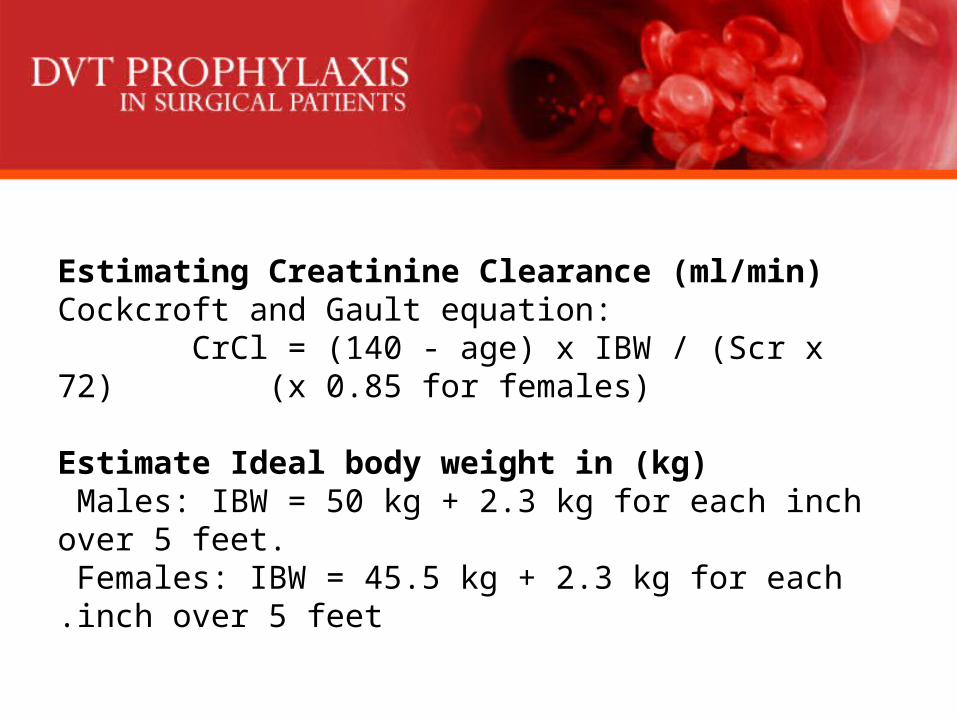
Estimating Creatinine Clearance (ml/min)Cockcroft and Gault equation: CrCl = (140 - age) x IBW / (Scr x 72) (x 0.85 for females)
Estimate Ideal body weight in (kg) Males: IBW = 50 kg + 2.3 kg for each inch over 5 feet. Females: IBW = 45.5 kg + 2.3 kg for each inch over 5 feet.
Thank You.