Embed Size (px)
Citation preview

OLD MAN’S CLAW HAND
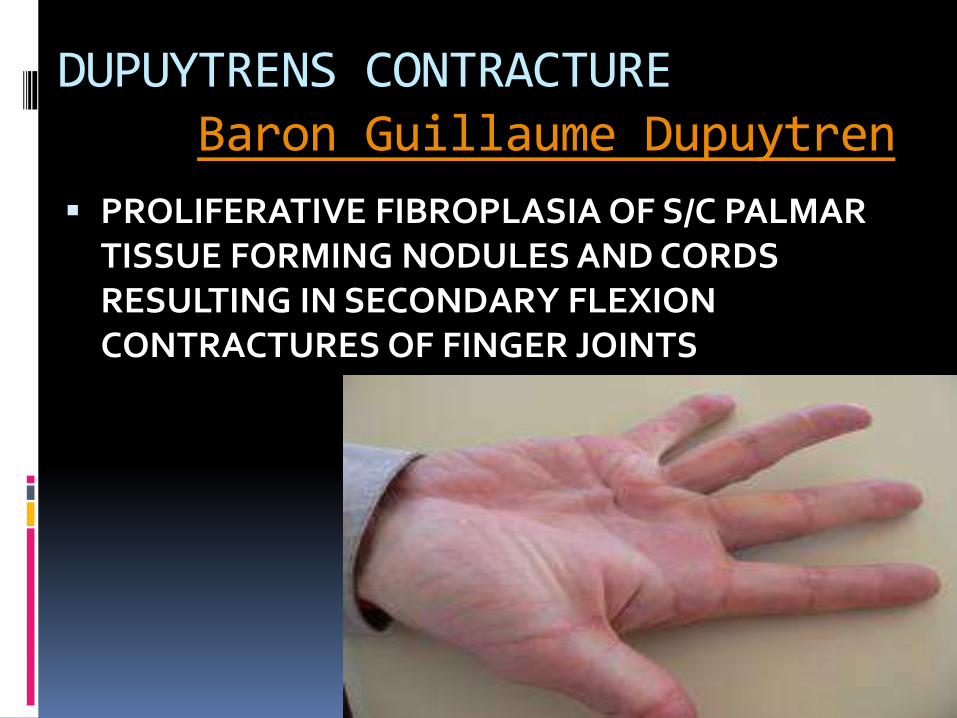
DUPUYTRENS CONTRACTUREBaron Guillaume Dupuytren
PROLIFERATIVE FIBROPLASIA OF S/C PALMAR TISSUE FORMING NODULES AND CORDS RESULTING IN SECONDARY FLEXION CONTRACTURES OF FINGER JOINTS

OTHER SECONDARY CHANGES
THINNING OF OVELYING S/C FAT
ADHESION OF SKIN TO LESION
PITTING OR DIMPLING OF SKIN
KNUCKLE PADS ON DORSUM OF PIP JOINTS

ETIOLOGY
AGE GROUP- B/W 50 AND 70
MALES ARE COMMONLY AFFECTED
HEREDITY-AUTOSOMAL DOMINANT PATTERN
TRAUMA AND MANUAL LABOUR?
VASCULAR INSUFFICIENCY AND CIGRATTE SMOKING

Associated conditions
Epilepsy (42%)
Alcohol-induced liver disease
Smoking
Diabetes mellitus
Hypertension
IHD

PATHOANATOMY
FASCIAL COMPONENTS INVOLVED
PRETENDINOUS BANDS
SUPERFICIAL TRANSVERSE LIGAMENT
SPIRAL BANDS
NATATORY LIGAMENTS
GRAYSONS LIGAMENTS
LATERAL DIGITAL SHEATH

Bands – Normal tissue Cords – Abnormal tissue

The basis of Dupuytren disease lies in
the nodule and the cord, the pathologic
counterparts to the tendon and
pretendinous bands. Most often, a
nodule forms on either side of the distal
crease of the palm. Later, nodules may
form near the MCP joint or next to the
PIP joint of the thumb and fourth and
fifth digits..

In the palm, contractures occur in the pretendinous bands and natatoryligaments, which are subsequently called the pretendinous cord and natatory cord, respectively.
In addition, a contracture maybe formed by the attachment of the transverse fibers of the palmar aponeurosis, which is found at the crease between the index finger and the thumb.
In the digits, normal fascial
structures, including the volar
superficial fascia and lateral digital
sheets, effectively become the central cord and lateral cords, respectively

PATHOGENESIS
Investigators have proposed several hypotheses for the pathogenesis of Dupuytrendisease. Most of them agree the cords and nodules are formed by fibroplasia and hypertrophy of already existing palmar fascia and subcutaneous fat.
Research has shown that growth factors such as basic fibroblast growth factor (FGF), platelet-derived growth factor (PDGF), and transforming growth factor-beta (TGF-â) may signal the overproduction of the myofibroblastsand/or myofibroblastic activity of the fibroblasts

History A patient typically presents with a history
of progressive loss of range of motion (ROM) of the affected finger(s)
The fourth digit most commonly is involved. The fifth, third, and second fingers are involved in decreasing order of frequency. Specifically, there is a decreased ability to fully extend the MCP joint(s); sometimes a decreased ability to fully extend the PIP joint(s) is noted.

The history may refer to an isolated nodule in this area, initially somewhat tender, which may have hardened and then disappeared. Asking about functional disabilities may elicit a history of certain tasks that the individual can no longer perform, such as grasping objects and typing.
No sensory deficits are reported unless there is a concomitant pathology. The condition is painless in its later stages.


CLINICAL FINDING
PAINFUL NODULES
DIMPLING OF OVERLYING SKIN
DEFORMITY AND INTERFRERENCE
OF NORMAL FUCTIONING OF
HAND

Examination reveals a palmar skin nodule, generally within the distal aspect of the palm.
The nodularity generally is not tender to palpation.
Puckering of the skin above the nodularitymay be noted. Overlying skin may be adherent to the fascia, and a fibrous cord can extend into the finger.
Flexion of the digit is normal for passive and active ROM.
Conversely, extension is limited at the MCP and sometimes the PIP joints of the affected digits. This limitation in finger extension occurs when testing passive and active ROM.
The ring finger (digit 4) is the most commonly involved site, followed by the small finger (digit 5). Other digits may be involved, although less commonly.
Loss of progressive flexion of the fingers in the resting position from the radial to ulnar side may be noted.
Although the patient may, because of the contractures, have difficulty grasping objects, strength is normal within the available ROM.
Sensation is typically normal.

PROGNOSIS
POOR PROGNOSTIC FACTORS
HEREDITY—FAMILY HISTORY
IN WOMEN IT BEGINS LATE AND PROGRESSES SLOW
ALCOHOLICS AND EPILEPTICS
BILTERAL

TREATMENT

OBSERVATION
WHEN CONTACTURE IS PROGRESSING SLOW
NOT DISABLING
REVIEW EVERY 3 MONTHS

RADIOTHERAPY
EFFECTIVE ONLY DURING EARLY FIBROPLASTIC PHASE

SURGERY- BEST KNOWN TREATMENT
1. SUBCUTANEOUS FASCIOTOMY
2.PARTIAL(SELECTIVE) FASCIECTOMY
3.COMPLETE FASCIECTOMY
4. FASCIECTOMY WITH SKIN GRAFTING
5.AMPUTATION

1.SUBCUTANEOUS FASCIOTOMY
PREFFERED IN ELDERLY,ARTHRITIS PATIENTS AND IF GENERAL CONDITION IS POOR
RESULTS ARE GOOD WHEN LESION IS MATURE
MAY BE DONE AS PRELIMINARY STEP TO FASCIECTOMY
72% RECURENCE RATE

CONTD…SUBCUTANEOUS FASCIOTOMY
TECHNIQUE- LUCK
DISEASED FASCIAL BANDS IS CUT WITH A SHARP INSTUMENT PASSED S/C THROUGH A PUNCTURE WOUND

AFTER TREATMENT- PRESSURE DRESSING IS USED FOR 24 HOURS,THEN SMALLER DRESSING
ACTIVE MOTION OF HAND AND FINGERS ENCOURAGED

2.PARTIAL(SELECTIVE) FASCIECTOMY
COMMONLY DONE PROCEDURE
LESS MORBIDITY
LESS COMPILCATIONS
50% CHANCE OF RECURRENCE
ONLY MATURE DEFORMING TISSUE IS EXCISED

ZIGZAG INCISION IS MADE OVER THE PATHOLOGIC STRUCTURE.INCISION EXTENDED PROXIMALLY AVOIDING CROSSING PALMAR CREASES AT RIGHT ANGLES.SKIN IS ELEVATED AND S/C TISSUE IS SEPERATED FROM PATHOLOGIC TISSUE
PATHOLOGIC TISSUE EXCISED.
Z-PLASTY WILL BE DONE


3.COMPLETE FASCIECTOMY
RARELY DONE BECOZ IT IS ASSOCIATED WITH HAEMATOMA,JOINT STIFFNESS,DELAYED HEALING AND RECURRENCE.

4. FASCIECTOMY WITH SKIN GRAFTING
INDICATED FOR YOUNGER PEOPLE WITH EPILEPSY,ALCOHOLISM.
SKIN AND UNDERLYING ABNORMAL FASCIA ARE EXCISED AND FULL THICKNESS OR THICK SPLIT SKIN GRAFT IS APPLIED.

AMPUTATION
IF FLEXION CONTRACTURES OF PIP JOINTS ARE SEVERE

POST-OP
STATIC DORSAL FOREARM SPLINT
WITH A DISTAL COMPONENT OVER DORSUM OF FINGERS TO WHICH THEY ARE STRAPPED IN EXTENSION
MIN 3 MONTH SPLINT
FINGER EXERCISES

Notable sufferers

Plantar fibromatosis-MorbusLedderhose benign nodules grow at the arch of the foot
cords can develop but not as frequently as with Dupuytren's contracture
Initially these nodules are usually painless but as they grow they can cause considerable pain when walking


same therapies apply
But feet have to carry a lot of weight and while a patient might be able to avoid the use of an operated hand, this is usually much more inconvenient with an operated foot
Ledderhose nodules seem to grow to bigger sizes than Dupuytren nodules

While contraction is usually observed at the hand (Dupuytren's contraction), it is not typical for Morbus Ledderhose though it might happen
. Development of cords seems to be less dominant for Ledderhose.
Possibly weight and continuous exercise keep feet and toes straight or the Ledderhosenodules reside in a more static area and are thus subject to less pulling forces than the nodule's in the hand.

Thus therapies to straighten toes again are less important for Morbus Ledderhose
the focus is more on reducing the size of the nodules, reducing pain and inflammation, and maintaining the ability to walk.
Therefore therapies for Ledderhose and Dupuytren's are probably as similar as foot and hand: similar, but not the same.
Thank you
&
Happy Teacher’s day