Embed Size (px)
Citation preview
Slide 1
Medicare, private health insurance and three elephants in the room
Paul Gross PhD
Invited address, 15th Annual Health Insurance Summit, 28 July 2016
Slide 2
This presentation
n Ten great truths (or at least bold conjectures) n Three elephants in the room n Refining PHI to bend the cost curve: 8 ways
Slide 3
Budget cuts +
PHI irrelevance +
Increasing privatisation of care =
Higher copayments AND
Larger elephant in room: financial protection
GREAT TRUTH 1 post 2 July 2016

Slide 4
GREAT TRUTH 2: Medicare reform 2016
Simplistic solutions ≠ Medicare reform
n Raise the Medicare levy1 n Medicare Select single payer + HSA2 n Unravel the MBS freeze3
n Medical Home pilot n Listing surgical Px prices alone4
None of these avoid the iceberg of RISING COPAYMENTS
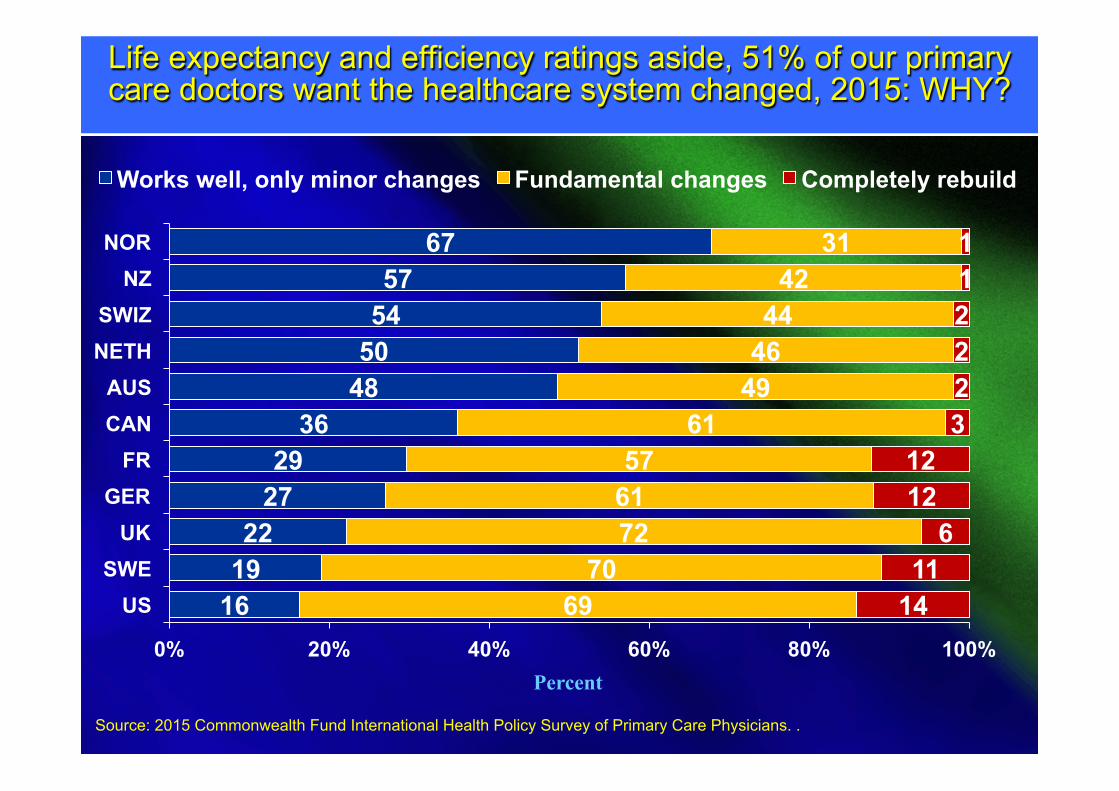
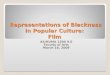
Slide 5 5 Life expectancy and efficiency ratings aside, 51% of our primary care doctors want the healthcare system changed, 2015: WHY?
16 19 22
27 29
36 48 50 54 57
67
69 70
72 61 57
61 49 46 44
42 31
14 11
6 12 12
3 2 2 2 1 1
0% 20% 40% 60% 80% 100%
US SWE
UK GER
FR CAN AUS
NETH SWIZ
NZ NOR
Works well, only minor changes Fundamental changes Completely rebuild
Percent
Source: 2015 Commonwealth Fund International Health Policy Survey of Primary Care Physicians. .
Slide 6
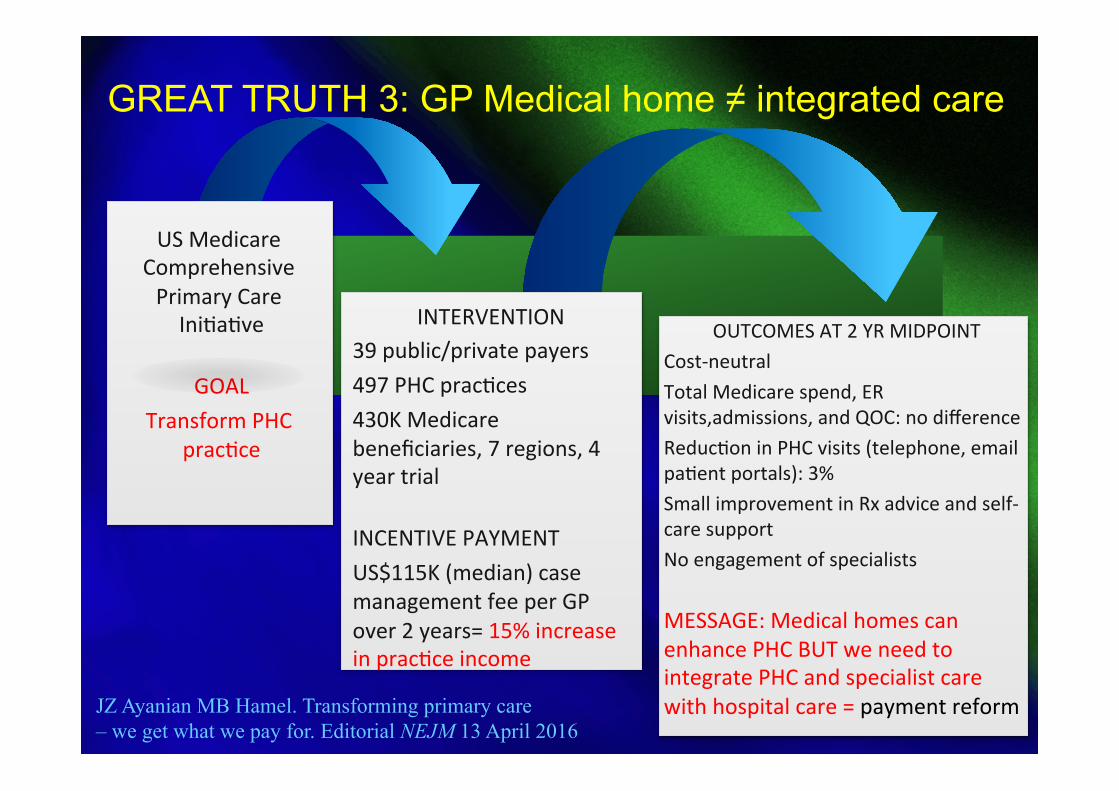
OUTCOMES AT 2 YR MIDPOINT Cost-‐neutral Total Medicare spend, ER visits,admissions, and QOC: no difference ReducEon in PHC visits (telephone, email paEent portals): 3% Small improvement in Rx advice and self-‐care support No engagement of specialists
MESSAGE: Medical homes can enhance PHC BUT we need to integrate PHC and specialist care with hospital care = payment reform
US Medicare Comprehensive Primary Care IniEaEve
GOAL Transform PHC
pracEce
INTERVENTION 39 public/private payers 497 PHC pracEces 430K Medicare beneficiaries, 7 regions, 4 year trial
INCENTIVE PAYMENT US$115K (median) case management fee per GP over 2 years= 15% increase in pracEce income
GREAT TRUTH 3: GP Medical home ≠ integrated care
JZ Ayanian MB Hamel. Transforming primary care – we get what we pay for. Editorial NEJM 13 April 2016

Slide 7
Great truth 4: Transitional care matters n Four of eleven programs in Medicare Coordinated Care
Demonstration reduced hospitalizations by 8–33 percent among enrollees who had a high risk of near-term hospitalization.
n Care coordinators in at least three of the four programs :
– supplement telephone calls to patients with frequent in-person meetings;
– occasionally meet in person with providers; – act as a communications hub for providers; – deliver evidence-based education to patients; – provide strong medication management; and – provide timely & comprehensive TC post-discharge
“The approaches would save money only if care coordination fees were modest and organizations found cost-effective ways to deliver the interventions”
Slide 8
GREAT TRUTH 5: NEP ≠ efficient prices
Pricing systems that do not measure adverse events, patient complexity and post-acute care following discharge do not generate “efficient” payments to hospitals.
Bundled payments for some surgery (joints, obstetrics, cataracts, some cardiac interventions) and post-acute care do so
Slide 9
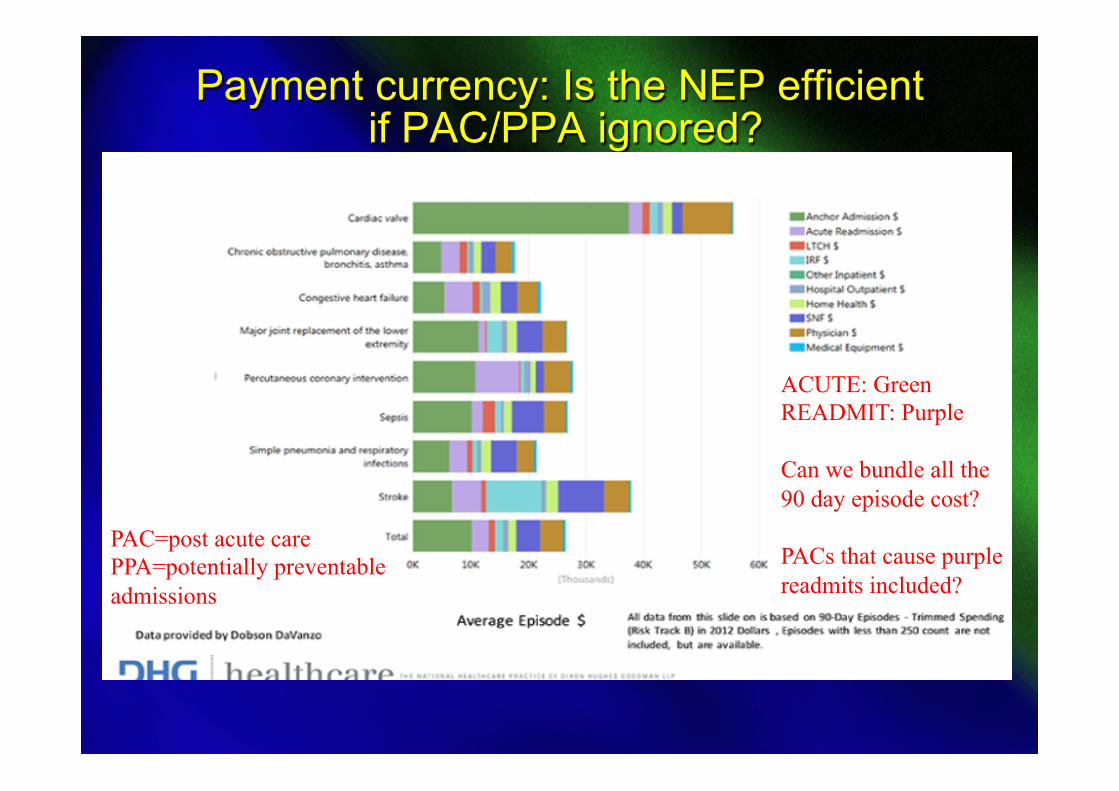
Payment currency: Is the NEP efficient if PAC/PPA ignored?
ACUTE: Green READMIT: Purple Can we bundle all the 90 day episode cost? PACs that cause purple readmits included?
PAC=post acute care PPA=potentially preventable admissions
Slide 10
GREAT TRUTH 6: Reform w/o doctors ≠ reform
It's a lot easier to get doctors and perhaps hospitals engaged in transformation when it's done at the locus of their control.
After De Brantes, 2015
Confirmed by Healthe initiative with DVA
Slide 11
Technological
Your Logo
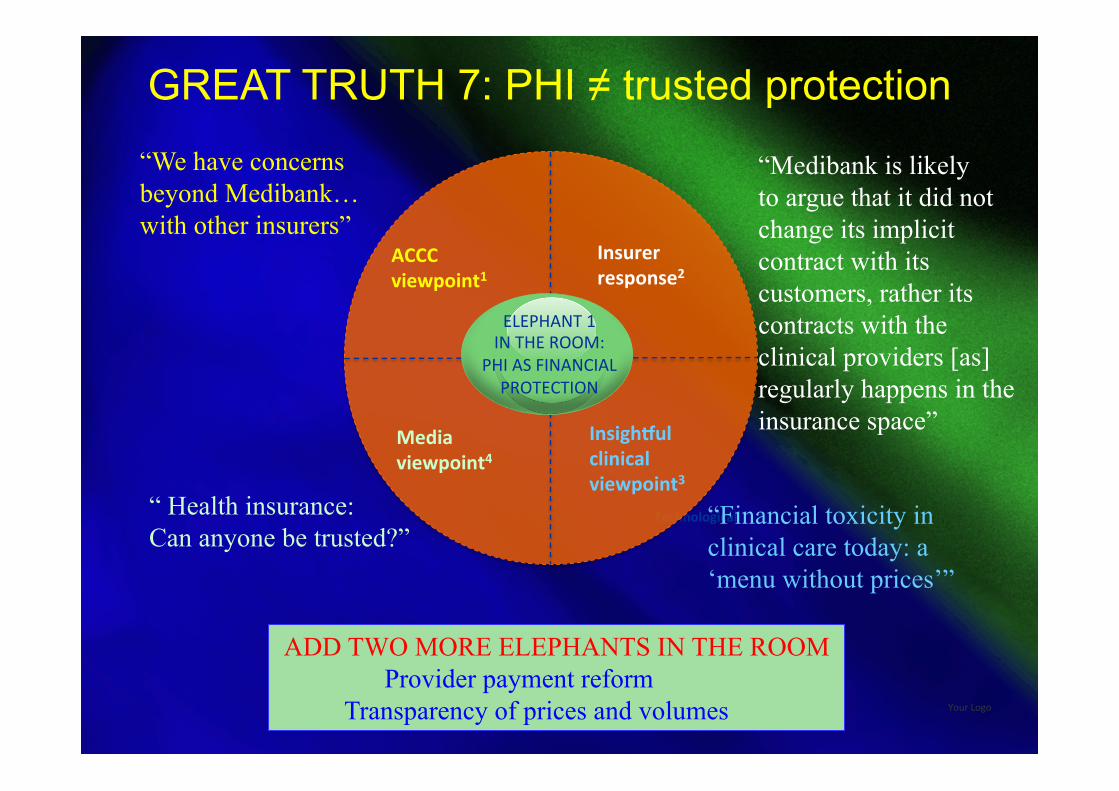
ELEPHANT 1 IN THE ROOM:
PHI AS FINANCIAL PROTECTION
ACCC viewpoint1
Media viewpoint4
Insurer response2
Insigh;ul clinical viewpoint3
“We have concerns beyond Medibank… with other insurers”
“ Health insurance: Can anyone be trusted?”
“Medibank is likely to argue that it did not change its implicit contract with its customers, rather its contracts with the clinical providers [as] regularly happens in the insurance space”
“Financial toxicity in clinical care today: a ‘menu without prices’”
ADD TWO MORE ELEPHANTS IN THE ROOM Provider payment reform Transparency of prices and volumes
GREAT TRUTH 7: PHI ≠ trusted protection
Slide 12
GREAT TRUTH 8: Payment reform starts with an undeniable fact
Expenditure = [(price) x (quantity)] + waste Medicare and PHI require policies for prices, volumes, inefficiencies and quality of care All big-bang reforms (Medicare Select, HSAs, managed care, competitive markets) sink without payment reform
Slide 13
GREAT TRUTH 9: PHI value case=f(D,P,PPC)
DATA Predict patient risk and cost Enhance chronic care management Compare quality, safety and prices
POLICIES Interoperability and use of EHRs Incentives for behavioral change Enhanced financial protection of individuals across the life cycle
PROVIDER PAYMENT CURRENCIES Reduce waste Reward better outcomes Reward hospitals for innovation in care
Slide 14
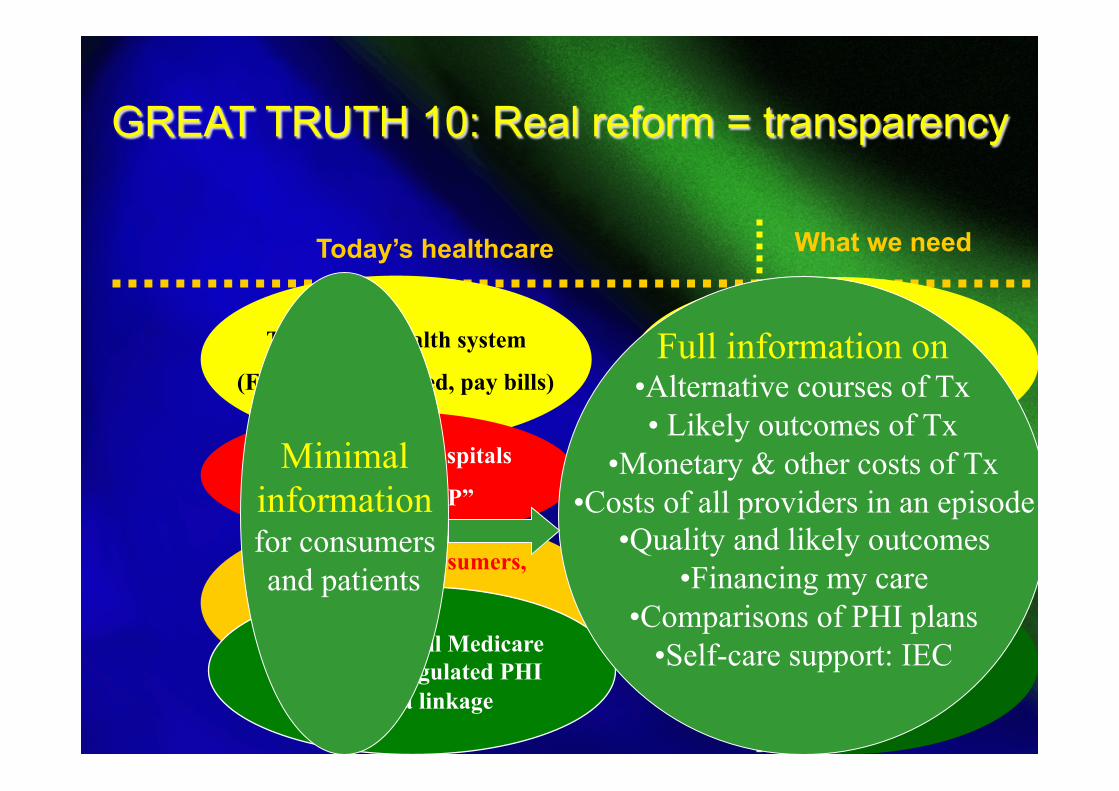
GREAT TRUTH 10: Real reform = transparency
Today’s healthcare What we need
Disease management (change behavior)
Traditional health system
(FFS, uncoordinated, pay bills)
Ill-informed consumers,
minimal self-care,
no economic incentives
Informed buyers,
Consumer-directed healthcare
Behavioral incentives
Multispecialist hospitals
Casemix, “NEP”
More single-specialty hospitals
Pay-for-value
Medicare
PHI + MSA’s, LTCI
Data linkage
One-size-fits-all Medicare Irrelevant, regulated PHI
No data linkage
Minimal information for consumers and patients
Full information on • Alternative courses of Tx • Likely outcomes of Tx
• Monetary & other costs of Tx • Costs of all providers in an episode
• Quality and likely outcomes • Financing my care
• Comparisons of PHI plans • Self-care support: IEC
Slide 15
Not all bad: Australian payers are moving
n Three PHI funds report doctor performance n One PHI fund reports adverse event rates in hospitals n One PHI fund develops m-health tools for members MEANWHILE n DVA shares data with doctors and hospitals, measuring adverse events and readmissions, feedback to hospitals on patient-reported events from every admission
Slide 16
But the PHI value case is zilch without
n Policies that enhance behavioral change n Tools that predict patient risk and cost n Tools that enhance chronic care management n Risk equalisation that encourages CCM n Tools that compare quality, safety and prices n Policies for interoperability and use of EHR n Payment currencies that reduce waste n Payment incentives to hospitals to innovate n Policies that enhance financial protection
Slide 17
Three elephants in the room n Provider payment reform n Transparency of prices, volumes, episode
costs, patient safety, clinical quality, health and functional outcomes, patient satisfaction
n Future financial protection in an era with
- government budget cuts - growing privatisation of care - rising copayments by households
Slide 18
PHI reform 1: payment currency beyond an NEP set at the average
“We propose that in a true pay-for-value system, a national payment rate should be established and rooted in reality (e.g., based on the costs of the top performing health care delivery organizations) and adjusted for three factors: a) risk of the patient population, b) geographic variation in the cost of doing
business, c) patient outcomes."
D Cortese et al HA Blog May 2016
Slide 19
PHI reform 2A: target sickest with MBS fee
n Target: four costliest 3-disease combinations - stroke, chronic kidney disease, and either - asthma, COPD, depression, or HF n New MBS incentives to doctors (+ new PHI) - engage patients in prevention - connect data and make MU of data - care transition services to reduce readmissions - extra payment for face-to-face management of
patients with 2+ CCs1 - targeted home visits + telemed incentives
Fontenot et al 2016; US Senate Committee on Finance , Bipartisan Chronic Care Working Group 2015
Slide 20
PHI reform 2B: PHI for chronically ilI n Personalised PHI for individuals with special care
needs because of CI n Rewards/incentives for participation in health-related
activities, starting with weight loss, diabetes management, diet
n Risk adjusted reinsurance pool having regard to physical and mental disability and # CCs
n Payment currency: care plans, quality, outcomes, higher payment for taking on higher risks (patient CC, patient engagement, care coordination tasks, IT use, Rx management)
n Mandatory patient satisfaction surveys of care coordination/transitions reimbursed by PHI
Fontenot et al 2016; US Senate Committee on Finance , Bipartisan Chronic Care Working Group 2015
Slide 21
PHI reform 3: reduce post-acute readmissions by payment currency + VBI
Source: MEDPAC June 2016
PAYMENT CURRENCY - common payment per stay, adjusted by patient characteristics1 - - longer term: bundled payment per episode VALUE-BASED HEALTH INSURANCE - measure outcomes (prevent under-treatment) - Report resource use (reduce unnecessary use, serial post-acute stays)
Patient characteristics are: age, diagnoses and comorbidities, patient severity and treatments, impairments, functional status and cognitive status
Slide 22
PHI reform 4: cover transition care of high-risk cases and pharmacy
n Insurer-initiated care transition program based on medication reconciliation by pharmacists via home visits and telephone for high-risk patients
- 50 percent reduced relative risk of readmission within thirty days of discharge and absolute risk reduction of 11.1 percent.
- Savings: $2 for every $1 spent. n “Such programs, focused on but not limited to medication reconciliation, improve clinical outcomes and reduce total costs of care”.
HA July 2016
Slide 23
PHI reform 5: provide incentives for hospital innovation
UKNHS payment reform announced 24 June 2016 n help technology companies that produce
innovative devices to win fast-track approval that gets their products into patients’ hands when they visit their GP or hospital consultant
n a new hospital “tariff” (case payment) providing a financial incentive to make greater use of innovation and technology
Today’s NEP/ Prostheses List determinations create no incentives
Slide 24
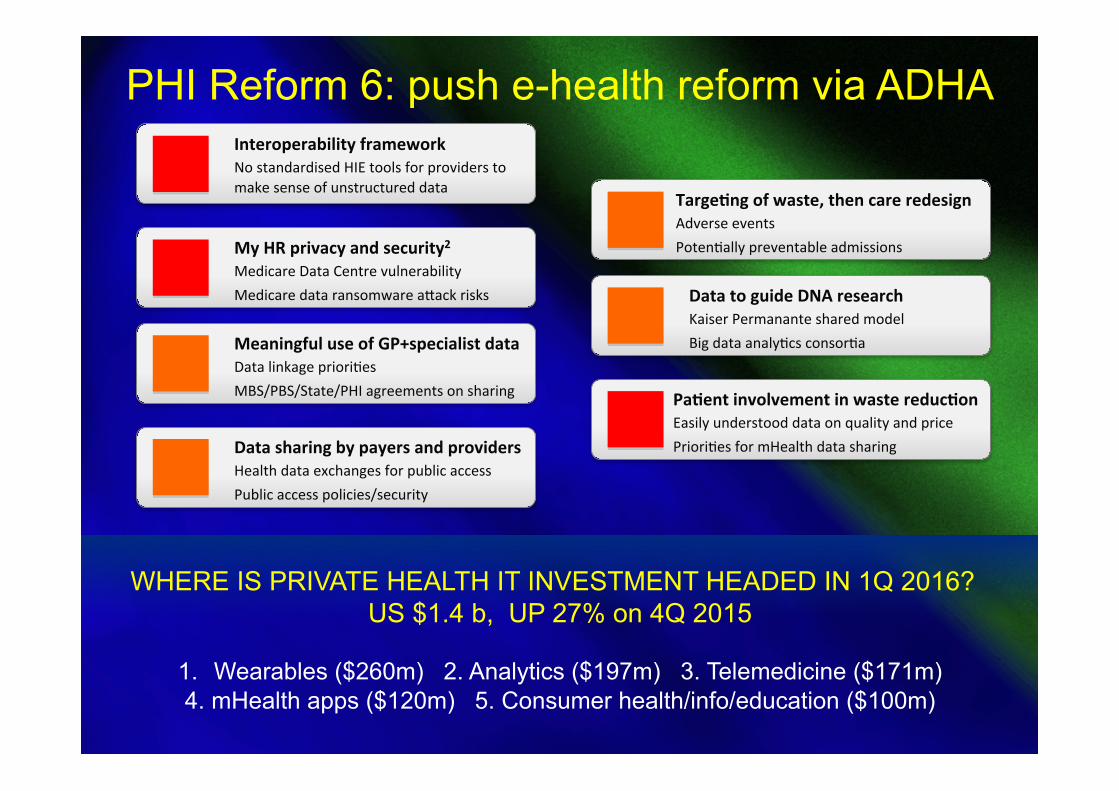
WHERE IS PRIVATE HEALTH IT INVESTMENT HEADED IN 1Q 2016? US $1.4 b, UP 27% on 4Q 2015
1. Wearables ($260m) 2. Analytics ($197m) 3. Telemedicine ($171m) 4. mHealth apps ($120m) 5. Consumer health/info/education ($100m)
Interoperability framework No standardised HIE tools for providers to make sense of unstructured data
My HR privacy and security2 Medicare Data Centre vulnerability Medicare data ransomware acack risks
Meaningful use of GP+specialist data Data linkage prioriEes MBS/PBS/State/PHI agreements on sharing
Data sharing by payers and providers Health data exchanges for public access Public access policies/security
TargeHng of waste, then care redesign Adverse events PotenEally preventable admissions
Data to guide DNA research Kaiser Permanante shared model Big data analyEcs consorEa
PaHent involvement in waste reducHon Easily understood data on quality and price PrioriEes for mHealth data sharing
PHI Reform 6: push e-health reform via ADHA
Slide 25
PHI reform 7: initiate transparency of P,V,Q,O
Draft a national healthcare transparency law 1. Specify framework for collecting patient data on tests, Txs, outcomes 2. Rich data source on all provider prices - Compel providers, payers to report prices charged to patients OR - Mandate a single all-payer claims database
3. Publish meaningful prices - All prices in a typical episode, not just a hospital stay or a doctor fee - Specify scope of prices (IP and OP) for full list of Px’s 4. Mandate standards for all websites: data currency, consumer tools NAYSAYERS: read CPR/HCI3 Report card on state price transparency laws, July 2016
Slide 26
PHI reform 8: take a visible role on financial protection in an ageing society
n Converging paths of insurance for workers
compensation, disability insurance sold as life insurance add-ons
n Gaps in data sets affecting insurance claims n Gaps in financial protection when individuals
fall through WC, life insurance, NDIS cracks n Growing privatisation of healthcare and aged
care as public budgets are trimmed n New high-cost interventions will stretch
private and public budgets -> new funding
Slide 27
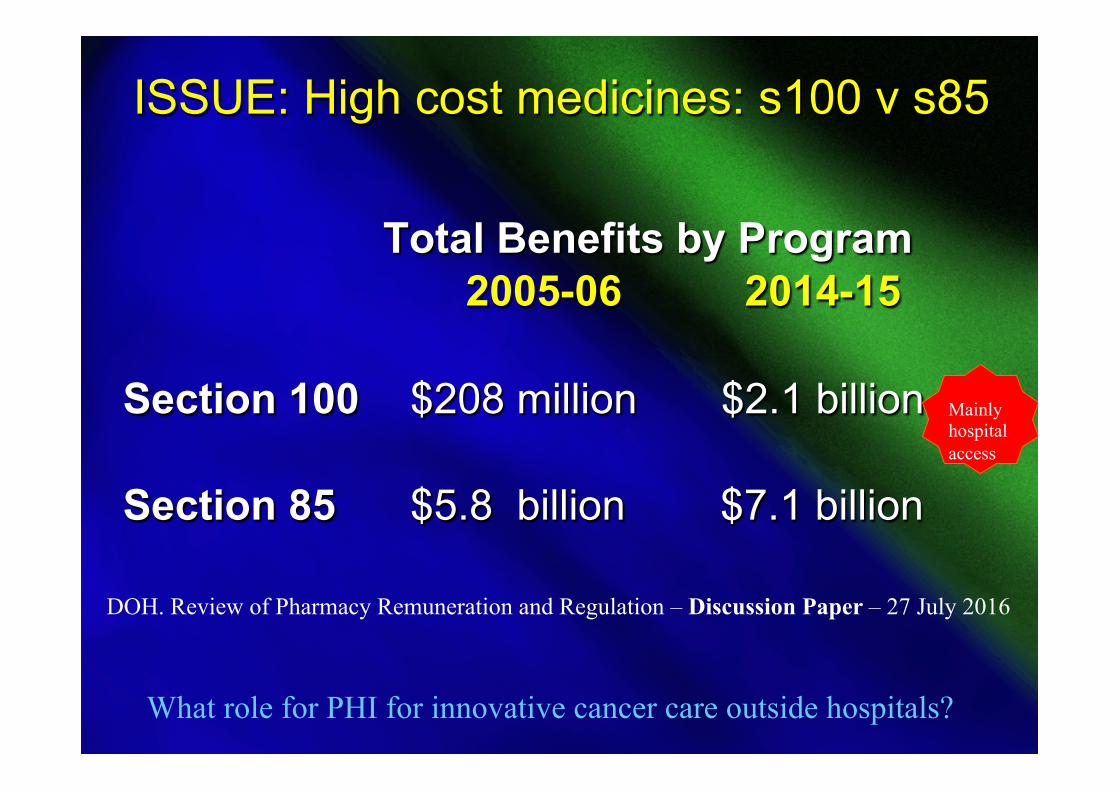
ISSUE: High cost medicines: s100 v s85
Total Benefits by Program 2005-06 2014-15 Section 100 $208 million $2.1 billion Section 85 $5.8 billion $7.1 billion
DOH. Review of Pharmacy Remuneration and Regulation – Discussion Paper – 27 July 2016
Mainly hospital access
What role for PHI for innovative cancer care outside hospitals?
Slide 28
Community-based cancer care: PHI role? Cancer care is privatising rapidly -> cost WILL rise More PGx drugs and biomarkers are coming: costs WILL rise Prostheses List gaps: breast biopsy markers ($100) not on Prostheses List, thus no patient charge, hospitals wear cost S100 Highly Specialised Drugs Program and the Efficient Funding of Chemotherapy (EFC) Program available mainly in private and public hospitals under treating specialist, at hospital supply cost Community based pharmacists: minimal role No incentives for community-based oncology care: PHI role?
Slide 29
ISSUE: Chronic care management & disability
n NDIS costs are surging: n PHI currently lies in a parallel domain n General insurance, WC and super-funded
insurance are in a separate domain n All cover disability, none have common
datasets n Disability prevention is minimal in all n Dutch study 2015: prevention of disability
should be on the PHI CCM reform agenda
Slide 30
Disability prevention in PHI? Dutch study
* “[W]e cannot expect a decrease in the prevalence of chronic diseases among the older population in the short run. * Investing in lifestyle changes at younger ages can pay off in the long run through a decrease in chronic diseases among the future old. * Life expectancy gains due to health improvements at younger ages lead to less expenditure growth than when these same gains are solely due to health improvements after 65.
(Wouterse et al, 2015)
Slide 31
Disability prevention in PHI? Dutch study
* [The modeling shows] the potential for cost containment through preventing disability. * Given that prevention of chronic diseases among older adults can be difficult in the short term, policies focusing on the improvement of independence of older adults with chronic disease could contain LTC costs. * In all scenarios, population aging leads to a rise in health services use. Health improvement policies thus have an important but also slightly limited role in containing health care costs”.
Slide 32
“It’s clear that somebody has to do something, and it’s just pathetic that it has to be us.”
Jerry Garcia (of the Grateful Dead)
We cannot let politicians stuff up healthcare by protracted inaction and endless reviews
The “us” are in this room