Embed Size (px)
DESCRIPTION
Dr Melody Caramins delivered the presentation at 2014 National Pathology Forum. The National Pathology Forum 2014 featured case studies on innovative testing methods in the fields of genetics, biobanking and PoCT. The highly interactive nature of the National Pathology Forum allowed delegates to network with each other and converse with the speakers asking questions as part of debates, industry roundtables, short workshops and panel discussions. For more information about the event, please visit: http://bit.ly/pathology14
Citation preview

Genetic testing: where are we now?
Dr Melody Caramins
National Head, Genetics, Specialist Diagnostic Services
Chair, RCPA Genetics Advisory Committee

Outline
• Definitions: Genetic testing, genomic testing,
mutations and variants
• Massively parallel sequencing (MPS)
• Current implementations of MPS
– Targeted approach
– Whole Genome approach
• Challenges
• Key points for policy

Genetics vs. genomics
Genetic tests – examining on a gene by gene level –e.g. CF
Genomic tests – examining the entirety of the genetic material
Very low resolution genomics
Karyotype
Low resolution genomics
Molecular karyotype
High resolution genomics
Whole genome sequencing
Whole exome = all
known/disease
implicated genes
Gene panels =
All known genes for a
disease

Your genome: what’s included?
• 2.9 billion bases
• 3.3 million variants
• 1.5 million variants in
genes
• ~100 genuine LoF
variants
• 5-20 genuine
pathogenic findings

What is a “mutation”?
• The classical definition of a “mutation” was
once:
– A permanent change in DNA sequence or structure
that is associated with a phenotype (generally
deleterious)
– Change is recognised by comparison of sample and
reference genomes, and is described in relation to
the reference
• Usage has changed
– Can include epigenetic modifications of DNA
– “mutation” is now mostly considered a colloquialism,
with “variant” being preferred.

Why look for variants?
• Can enable specific diagnosis confirmation,
classification, or exclusion
• Can determine appropriate management based
on molecular biological classification of a disease
• Can determine risk of disease
• Can reduce risk of developing disease
• Can lead to recognition of new diseases

Why now? A history of sequencing
• Cost of HGP= 600 000 genomes today at $5000 each

MPS is disruptive innovation
• Disruptive Innovation = Allows popular or
more general access to a product or service
that was historically only accessible to
consumers with a lot of money or a lot of skill.
• Often, the value of a such technologies is
initially dismissed (e.g. the PC)
• Institutions are often blindsided as the
technology matures and suddenly gains a
larger audience, e.g. email, mobile computing/devices,
Wikipedia.


Current implementation models
• Targeted
– Panels (handful hundreds of genes)
– Exome
• Whole genome sequencing

Targeted sequencing – gene panels
• Pros
– Tractable - testing using targeted panels is
currently available both in Australia and overseas
– Clinical utility is well established for many
disorders
– Minimises risk of “incidental findings”
– Genes previously considered untestable can now
be included
– Variants identified in other related genes which
modify phenotype and prognosis
– Avoid “diagnostic odyssey”

Targeted sequencing – gene panels
Cons:
• As gene panel sizes
increase, clinical
sensitivity and diagnostic
yield increases
• However, this
improvement is tempered
by an emerging
interpretive challenge,
with inconclusive results
increasing up to 10 fold
• Unknown causative genes
not included

• ~40Mb (coding) or 60Mb (coding + UTRs)
• Greatest application in gene identification in research,
or diagnosis of unknown rare genetic disorders
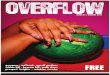
Targeted sequencing - exomes

Inherited Mendelian Diseases Identified
by Exome Sequencing
Rabbani, B., et al. (2012) J. Hum. Genet. 57:621-632.
By mid-2012, ~100 genes identified.
By mid-2013, >150 genes identified.

Evaluated 500 patients
8% not genetic
92% Traditional testing model
42% diagnosed, majority at 1st
clinical consultation
50% undiagnosed. Conservative cost $25 000/ diagnosis
25-50% of this cohort could be diagnosed by
WES/WGS
(fraction of the cost)
clinically and economically viable
alternative


Whole genome sequencing
• Challenge of appropriate interpretation
• Enormous amount of genetic variation – both
inter-population and inter-individual, with
many international collaborative efforts to
catalogue variation – HapMap, DGV, HVP,
1000 genomes, ClinVar, etc...
• Spectrum of variation effect from:
no change in
discernible
phenotype
alternative
phenotypes
with no medical
consequence
medical consequences of varying
severity and penetrance
disease susceptibility→ pathogenic
Variants of unknown significance (VUS)

Clinical interpretation & pathogenicity
Recent publication evaluating coverage and concordance of clinically relevant genetic variation provided by WGS in 12 patients:
• 10-19% of inherited disease genes were not covered to acceptable standards
• Good platform concordance for SNV but poor for indel variants
• 90-127 variants/individual requiring ~55 min curation each, 2-6 disease causing variants/individual
• Variant classification agreement = kappa 0.52
• 1-3 follow-up diagnostic tests or referrals
Image by D.Shrigley

Summary of approaches
Targeted Panel
(few-hundreds
genes)
Whole Exome
(~90% coverage
of 20 000 genes)
Whole genome
Size 500kb – 3 Mb 45-62 Mb 3.1 Gb
Advantages Greater sensitivity,
Greater specificity
High clinical utility
Easier analysis
Quick and cost
effective
Higher chance of
finding a mutation
in all the protein-
coding regions
Covers everything
Disadvantages Pathogenic mutations
could be in genes not
covered
High drop out rate
of some exons and
incomplete
coverage (~80-
90%)
Very challenging
and expensive
analytics
Success rate High Good but complex
and challenging to
implement
In nascent phase
of utility evaluation
for diagnostics

Wright C BMJ 2013
Which approach?

The new genomics will save money?
• Paradigm: a less expensive test/procedure, utilisedin a larger swath of indications.
• A previous example: laparascopic cholecystectomy.– Hypothesised savings due to shorter hospital stays,
decreased complications
– Increased costs due to 20% increase in surgery uptake.
• Genomics will lower costs?– Pharma companies may increase prices due to reduced
target market
– Physicians may continue to treat inappropriately (although not borne by MBS if clear indications for rebate)
– Cost of follow up confirmatory testing in inherited disease, and testing of relatives?

Things change….

Things change…

• The use of genomic technologies (genome-
wide arrays or WGS) requires a justification
in terms of necessity (the need to solve a
clinical problem) and proportionality (the
balance of benefits and drawbacks for the
patient).

Challenges (not a comprehensive list)
Technical
How much to sequence
How complete is coverage
Scalability of interpretive practices
Ethical
Who to sequence
Incidental findings –report, or
not?
Biological
Which sequence
variant findings are relevant and contribute to
current diagnosis?
Which sequence
variant findings are relevant to clinical care
but not necessarily
to presenting diagnosis?
(clinically actionable
incidental data)
Informatics
What sequence
information should be
stored
Where can it be stored,
who should have access
to it?
• How do we most responsibly communicate
results to patients and their doctors?
• How do we best balance individuals’ right to
privacy/security of health information vs.
community benefit of sharing information?

• Many of the issues are not entirely new, but the
scale of the challenges is
• Our frameworks and guidelines for good clinical
services are based on experiences to date;
these are surpassed by the amount of
information available
– Should current frameworks dictate developments?
– Should existing frameworks be reconsidered?

Differing international opinionsACMG ESHG
Diagnostic laboratories should
routinely screen all clinical
exomes/genomes for a list of
known variants in genes
associated with medically
important conditions
Preferable to use a targeted
approach to avoid unsolicited or
uninterpretable findings.
Genomic screening is not
specifically advocated. Variants
with limited/no clinical utility
should be filtered out (neither
analyzed nor reported
Patients cannot opt out of
genetic screening, it is the
responsibility of the clinical team
to provide appropriate pre and
post test counseling
Guidelines for informed consent
need to be developed, but the
individual’s right not to know
does not automatically over-ride
professional responsibilities
The genomes of minors should
be screened for variants offering
clinical utility to their parents
Guidelines for minors need to be
developed regarding what
unsolicited information should
be disclosed

Key points of awareness for policy
• Individuals vary in their tolerance for uncertainty
• Individuals vary in their understanding of predictive
value (or lack thereof) of genomics
• Autonomy of patients should be balanced with
autonomy of relatives
• Resolve whether healthcare providers have a duty
to search for and act on clinically actionable
variants that are not directly pertinent to the clinical
question
• Resolve whether healthcare providers have a duty
to interpret data with uncertain predictive value

THANK YOU!

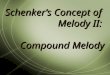
Overview of the MPS process
• Aim to provide improved constitutional and
somatic mutation detection in diagnosis and
research
1 2 3 4 5 6
Assay
development
DNA
extraction
Library
preparation
Sequence
generation
Primary
data
analysis
data
analysis
Secondary
Primer design
Primer validationTarget enrichment
Sample indexing
-SOLiD 5500 XL
-Ion PGM
-OtherImage or signal
processing
Mapping
SNP calling
SV

MDT meetings

Altman A, Weber P et al
Human Genetics 2012

• Next Generation Sequencing Data
• Primary Sequence Alignment• BWA
• Refined Sequence Alignment• GATK/Picard
• Variant Calling• SAMTools/GATK
Variant Annotation
• Annovar
Candidate genes/potential causative variants

Ashley et al. Lancet 2010, 375:1525
An approach to comprehensive analysis of
a human genome in a defined clinical
context

Kaiser J. Science (2012) 338:1016-1017.