Embed Size (px)
Citation preview
PEPTIC ULCER DISEASEPresenting by:
Dr. Aiydarus Ali AhmedGeneral Medine and Surgery
Banadir University - Faculty of Medicine
Mogadishu-Somalia
Background
• Peptic ulcer disease (PUD) is a
common disorder that affects
millions of individuals in the world
each year, with a major impact on
health care costs.
• In the last two decades, major
advances have been made in the
understanding of the
pathophysiology of PUD,
particularly regarding the role of
Helicobacter pylori infection and
nonsteroidal anti-inflammatory
drugs (NSAIDs).
• This has led to important changes
in diagnostic and treatment
strategies, with the potential for
improving the clinical outcome and
decreasing health care costs.
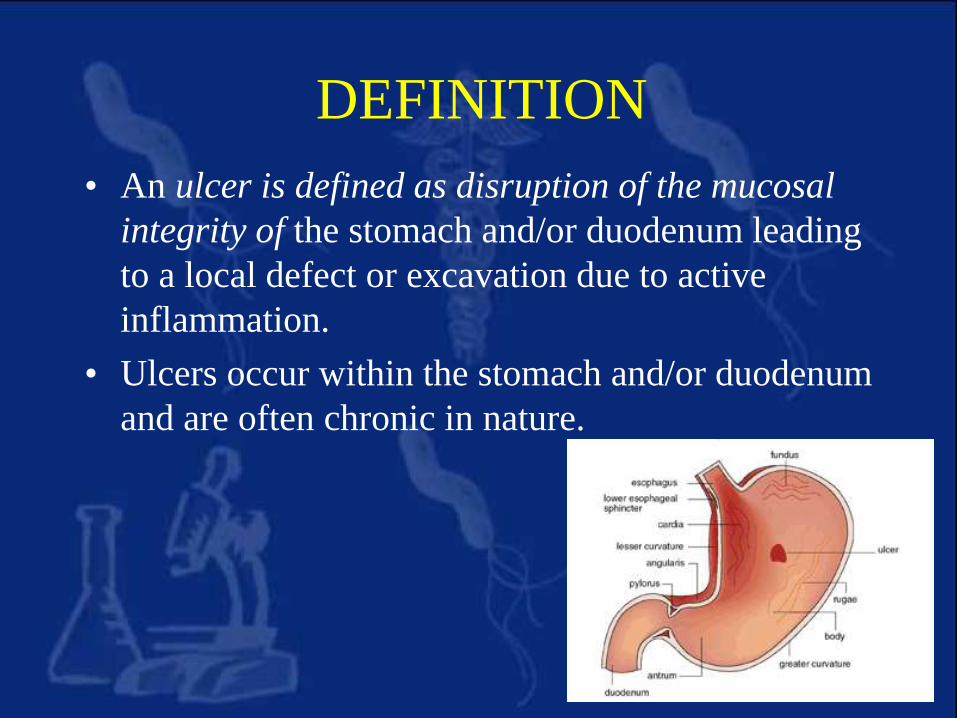
DEFINITION
• An ulcer is defined as disruption of the mucosal
integrity of the stomach and/or duodenum leading
to a local defect or excavation due to active
inflammation.
• Ulcers occur within the stomach and/or duodenum
and are often chronic in nature.
Epidemiology• Peptic ulcer is very common among the population.
• Ulcers can develop at any age
• They most often occur from early middle age onwards (
30 - 50), with gastric ulcers being more common in
elderly people ( > 60).
• Affect both men and women.
• May be acute or chronic
• Acute ulcers are often multiple, produce no symptoms
and usually heal without scarring.
• Chronic ulcers are deeper, usually occur individually and
usually produce symptoms. They leave a scar when they
heal.
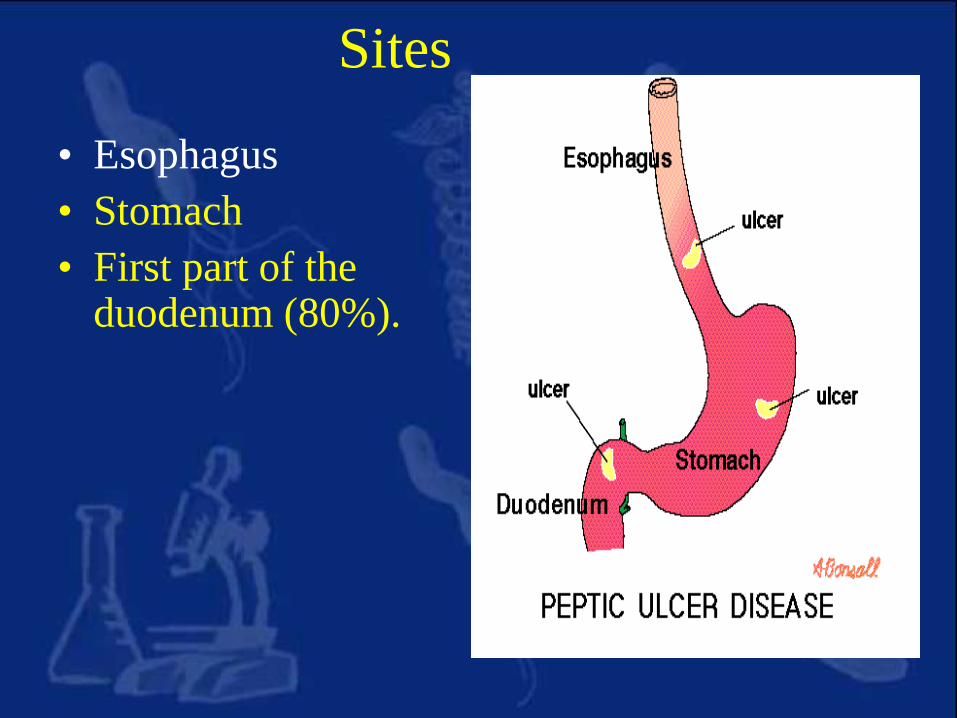
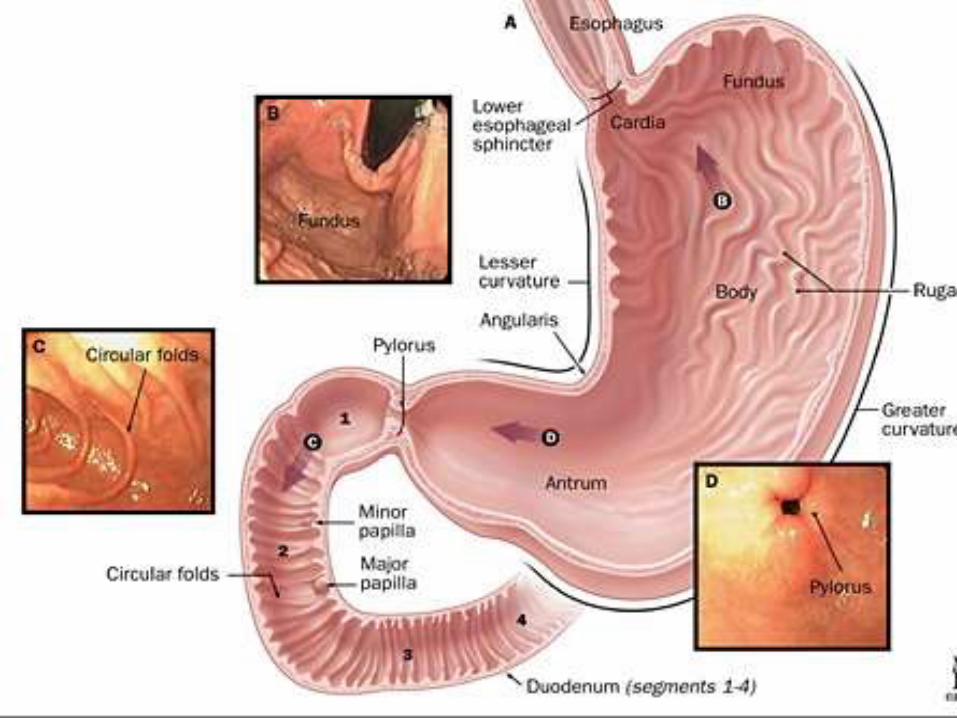
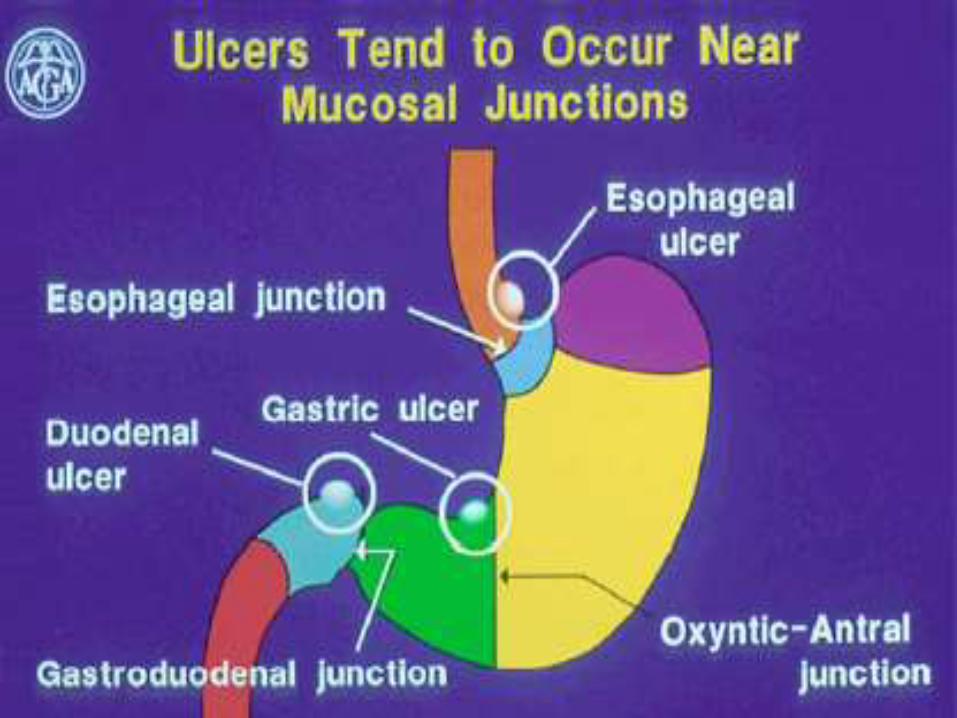
Sites
• Esophagus
• Stomach
• First part of the duodenum (80%).
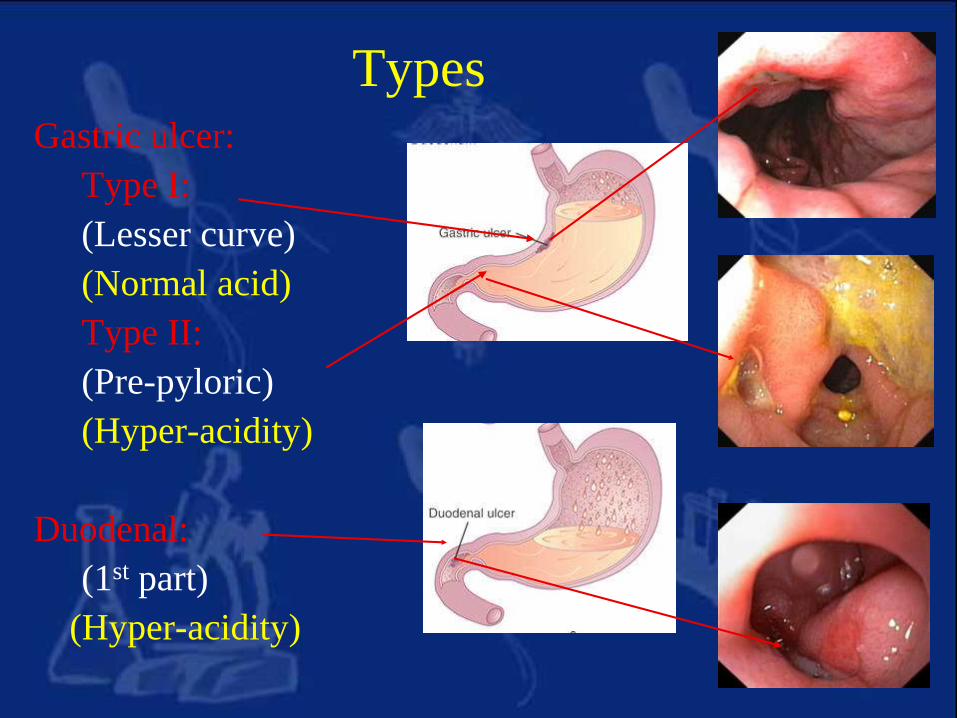
TypesGastric ulcer:
Type I:
(Lesser curve)
(Normal acid)
Type II:
(Pre-pyloric)
(Hyper-acidity)
Duodenal:
(1st part)
(Hyper-acidity)
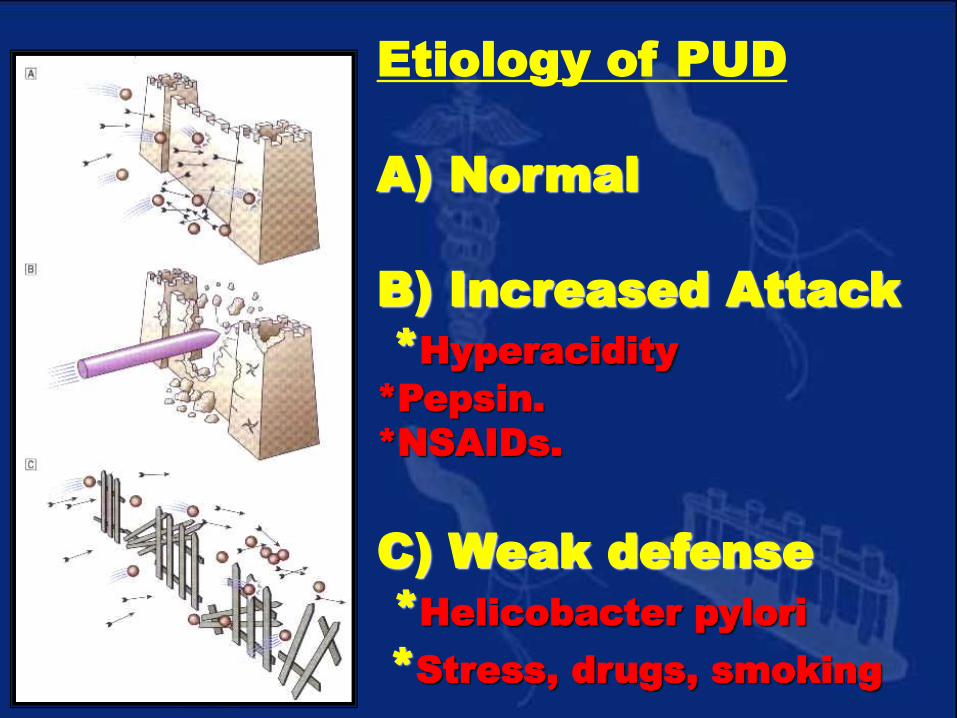
Etiology of PUD
A) Normal
B) Increased Attack
*Hyperacidity
*Pepsin.
*NSAIDs.
C) Weak defense
*Helicobacter pylori
*Stress, drugs, smoking
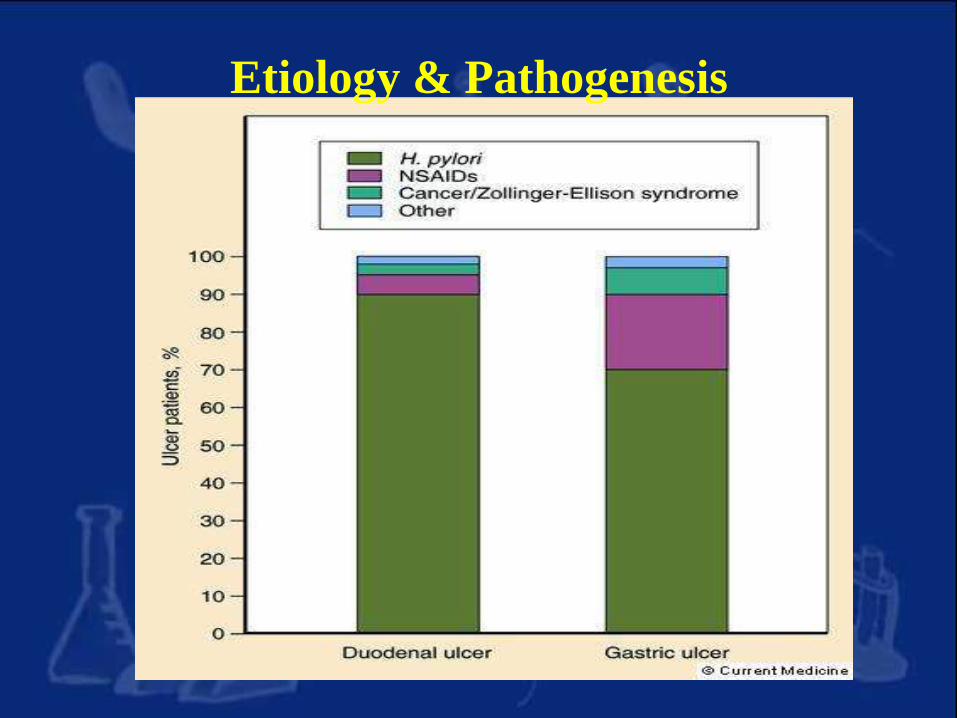
Etiology & Pathogenesis
1. Helicobacter pylori infection
2. NSAIDs & Aspirin
3. Acid/Pepsin
4. Smoking
5. Genetics
6. Psychological factors
Nonsteroidal anti-inflammatory drugs, NSAIDs
Etiology & Pathogenesis
Cont…
• The most important contributing factors are H pylori,NSAIDs, acid, and pepsin.
• Additional aggressive factors include smoking, ethanol, bile acids, aspirin, steroids, and stress.
• Important protective factors are mucus, bicarbonate, mucosal blood flow, prostaglandins, hydrophobic layer, and epithelial renewal.
– Increased risk when older than 50 d/t decrease protection
• When an imbalance occurs, PUD might develop.
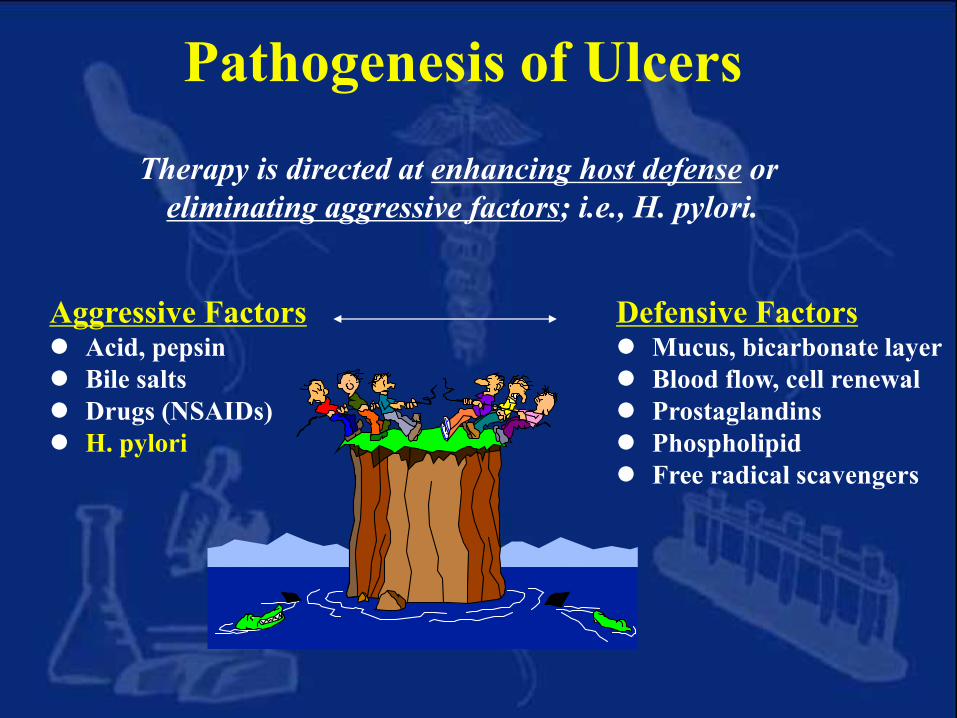
Pathogenesis of Ulcers
Aggressive Factors Acid, pepsin
Bile salts
Drugs (NSAIDs)
H. pylori
Defensive Factors Mucus, bicarbonate layer
Blood flow, cell renewal
Prostaglandins
Phospholipid
Free radical scavengers
Therapy is directed at enhancing host defense or
eliminating aggressive factors; i.e., H. pylori.
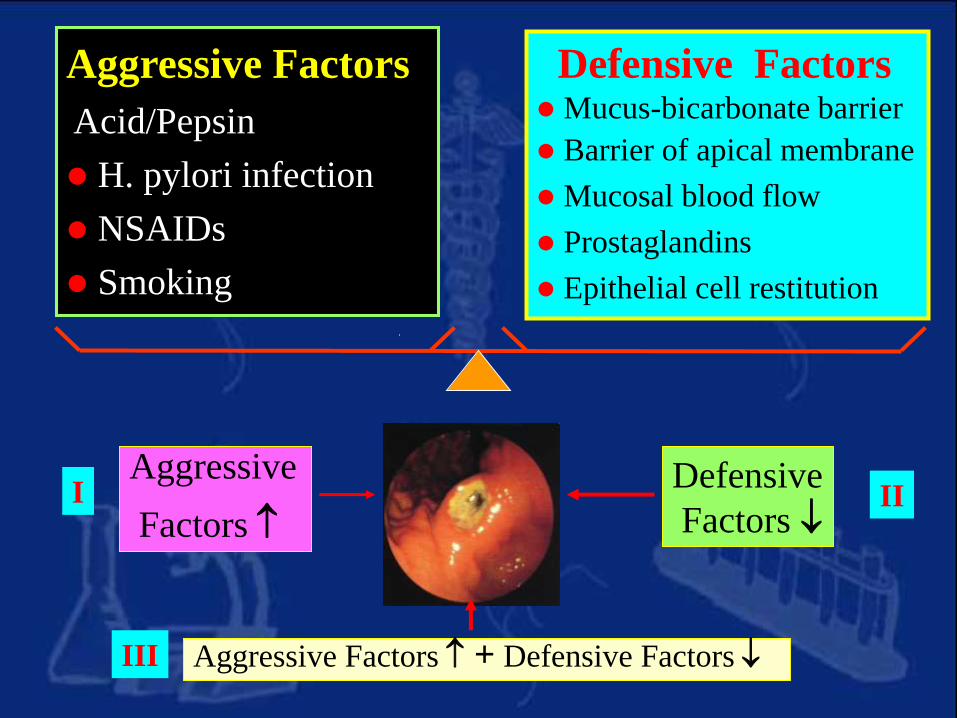
Aggressive Factors
Acid/Pepsin
H. pylori infection
NSAIDs
Smoking
Defensive Factors Mucus-bicarbonate barrier
Barrier of apical membrane
Mucosal blood flow
Prostaglandins
Epithelial cell restitution
Defensive
Factors
Aggressive
Factors
Aggressive Factors + Defensive Factors
I II
III
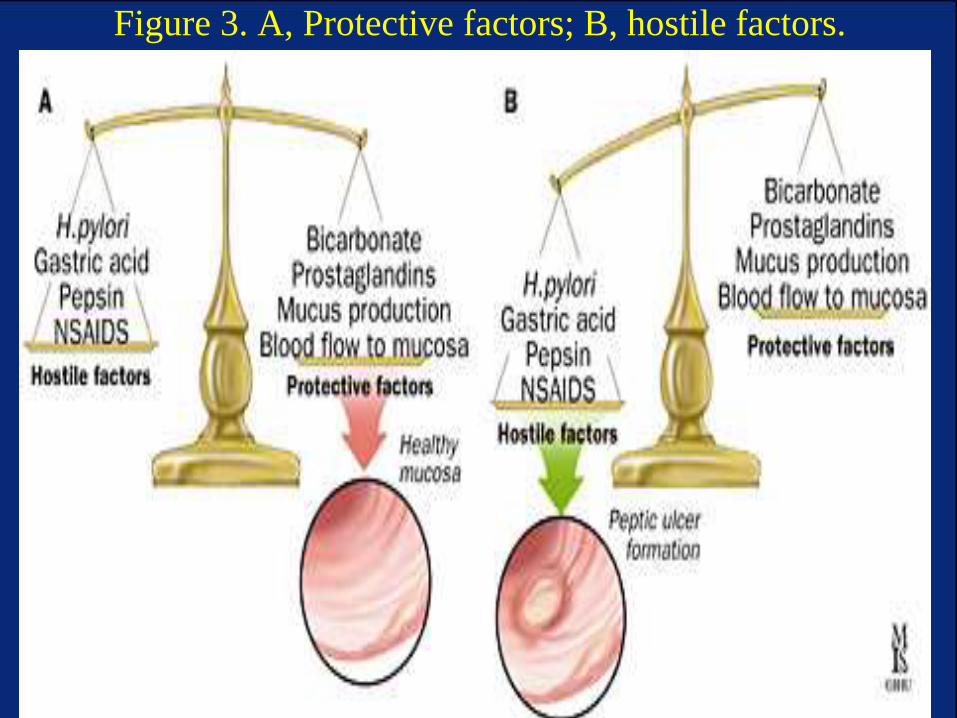
Figure 3. A, Protective factors; B, hostile factors.
Dictum No acid, no ulcer
No acid, no Hp, no ulcer
No Hp, No NSAIDs, no ulcer
Evolving Knowledge
Two Common Forms of Peptic Ulcer
H.pylori – associated: 70-85%
NSAIDs – associated: 10-25%
Non-Hp, Non-NSAID Ulcer: 5-30%
1. Helicobacter pylori in Peptic
Ulcer
•It is found in the gastric antrum of the stomach
•95%of duodenal ulcers & 85% of gastric ulcers
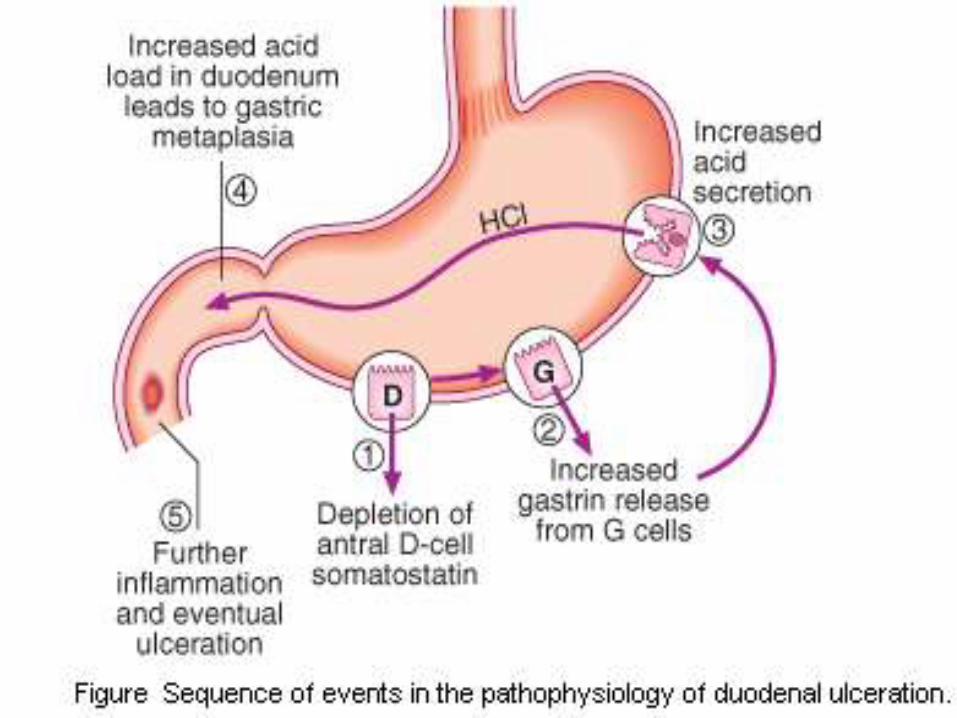
• In most people H. pylori causes antral
gastritis associated with depletion of
somatostatin (from D cells) and gastrin
release from G cells.
• The subsequent hypergastrinaemia
stimulates acid production by parietal cells,
but in the majority of cases this has no
clinical consequences.
• In a minority of patients (perhaps smokers)
this effect is exaggerated, leading to
duodenal ulceration . The role of H. pylori
in the pathogenesis of gastric ulcer is less
clear but H. pylori probably acts by
reducing gastric mucosal resistance to
attack from acid and pepsin.
• In approximately 1% of infected people, H.
pylori causes a pangastritis leading to
gastric atrophy and hypochlorhydria. This
allows bacteria to proliferate within the
stomach; these may produce mutagenic
nitrites from dietary nitrates, predisposing
to the development of gastric cancer
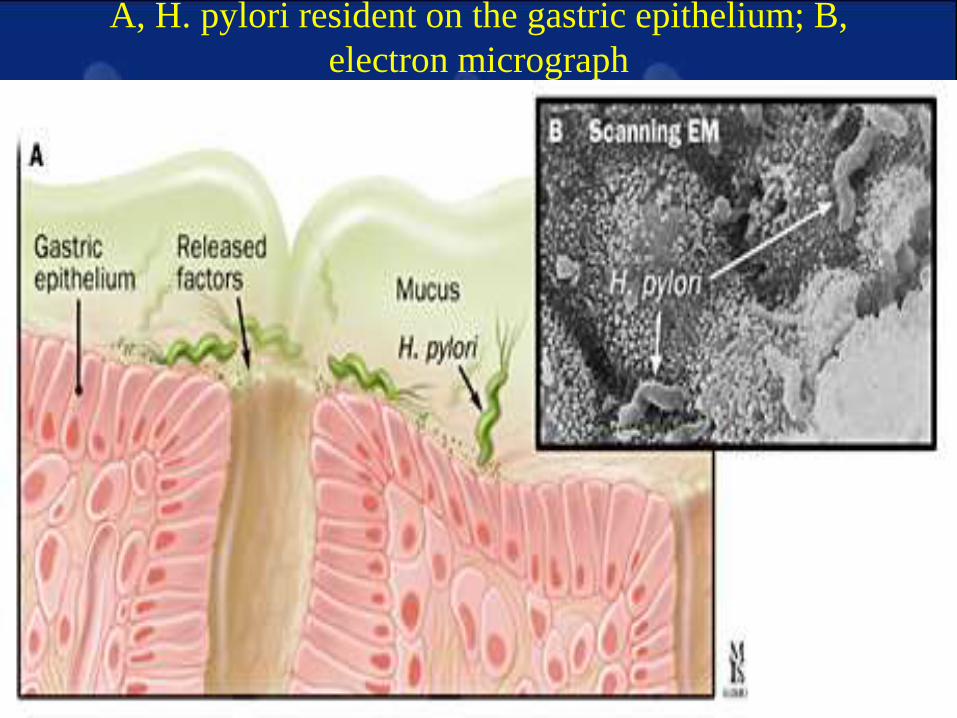
A, H. pylori resident on the gastric epithelium; B,
electron micrograph
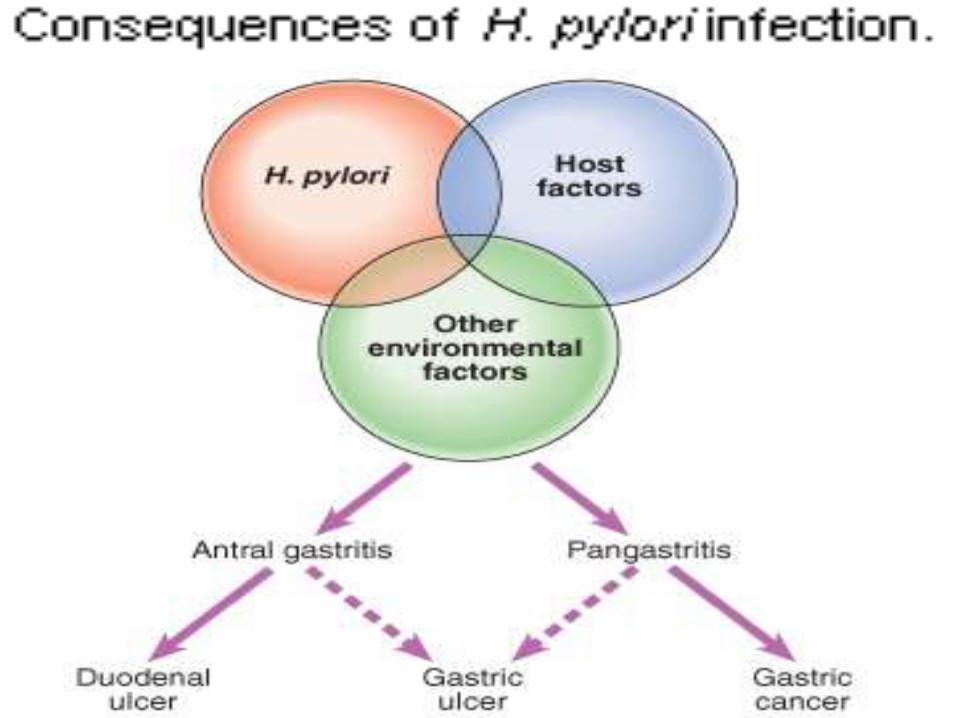
• Specifically, the presence of antral-
predominant gastritis is associated with
DU formation; gastritis involving
primarily the corpus predisposes to the
development of GUs, gastric atrophy,
and ultimately gastric carcinoma .
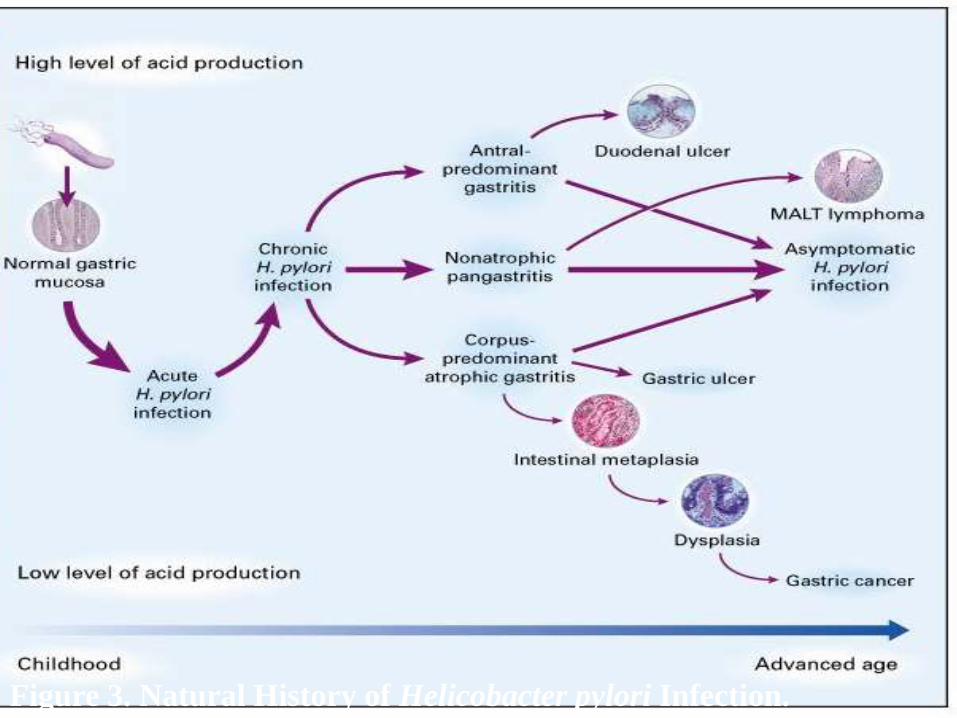
Figure 3. Natural History of Helicobacter pylori Infection.
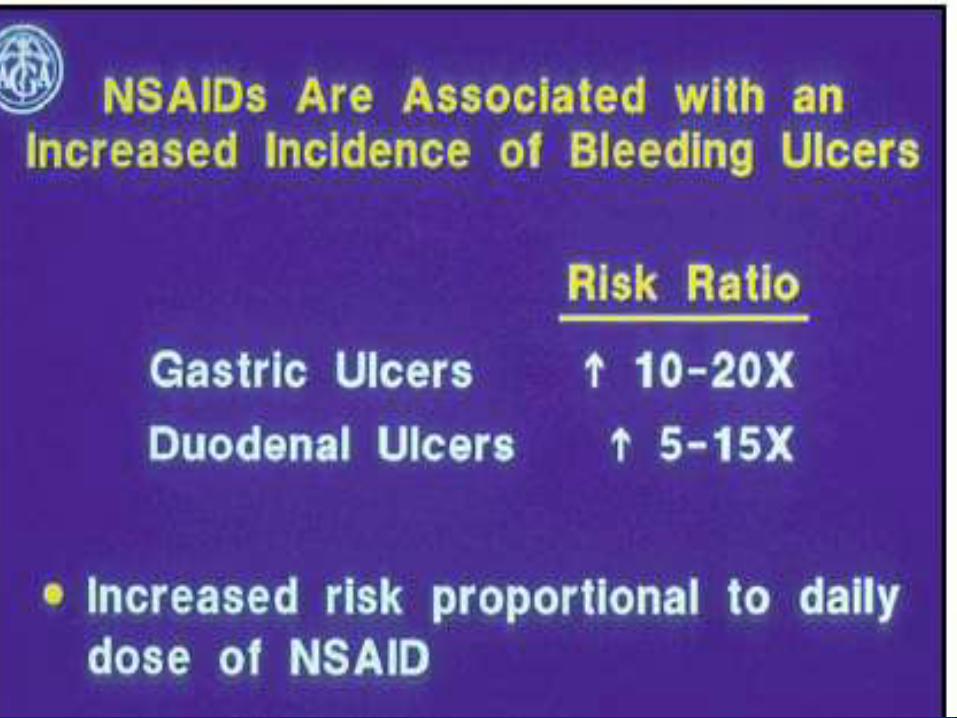
2. NSAIDs & Peptic Ulcer
• Apart from H pylori infection,
NSAID (or aspirin) use is the
other major identifiable risk
factor for PUD. Accounts for the
majority of H pylori–negative
ulcers.
• Second most common cause of
PUD.
NSAIDs
• Prostaglandins have important
several mechanisms to protect gastric
mucosa. They stimulate bicarbonate &
mucus secretion from the gastric
mucosa. Also they increase the
microvasculature of the mucosa. All
these mechanisms are called the
mucosal barrier.
• NSAIDs act by inhibiting cyclo-
oxygenase enzyme (COX) leading to
decrease prostaglandins at the site of
inflammation.
• NSAIDs decrease gastric and duodenal
prostaglandins, so mucosal erosions &
ulcerations will occur.
• The cyclo-oxygenase enzyme (COX)
has 2 types, COX-2, which is present
at sites of inflammation and COX-1,
which is present in the stomach. So
COX-2 inhibitors will not affect the
gastrointestinal mucosa.
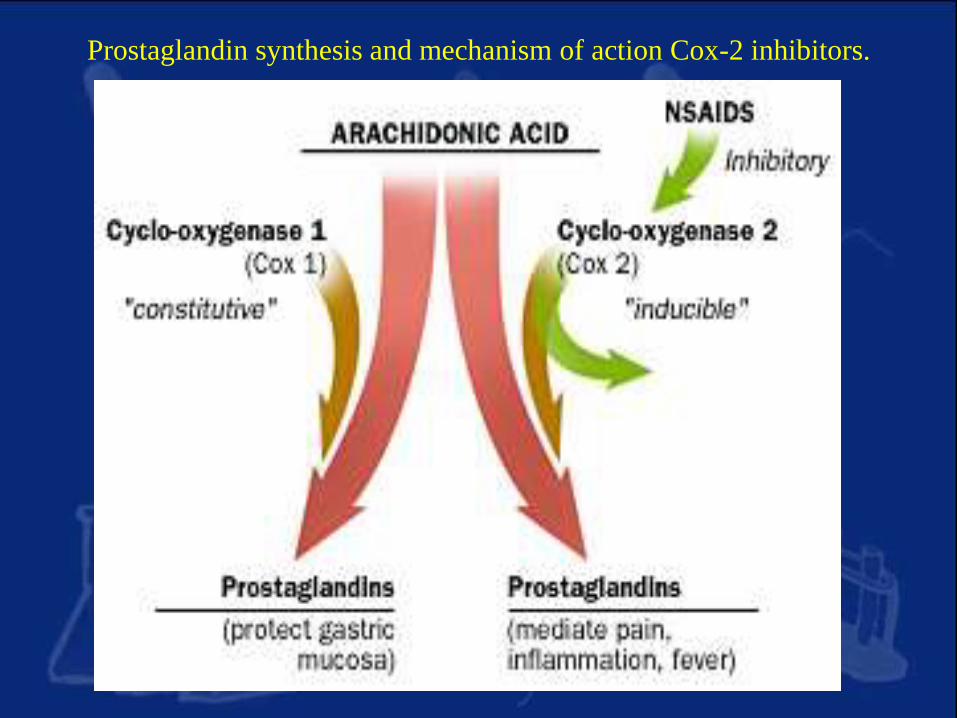
Prostaglandin synthesis and mechanism of action Cox-2 inhibitors.
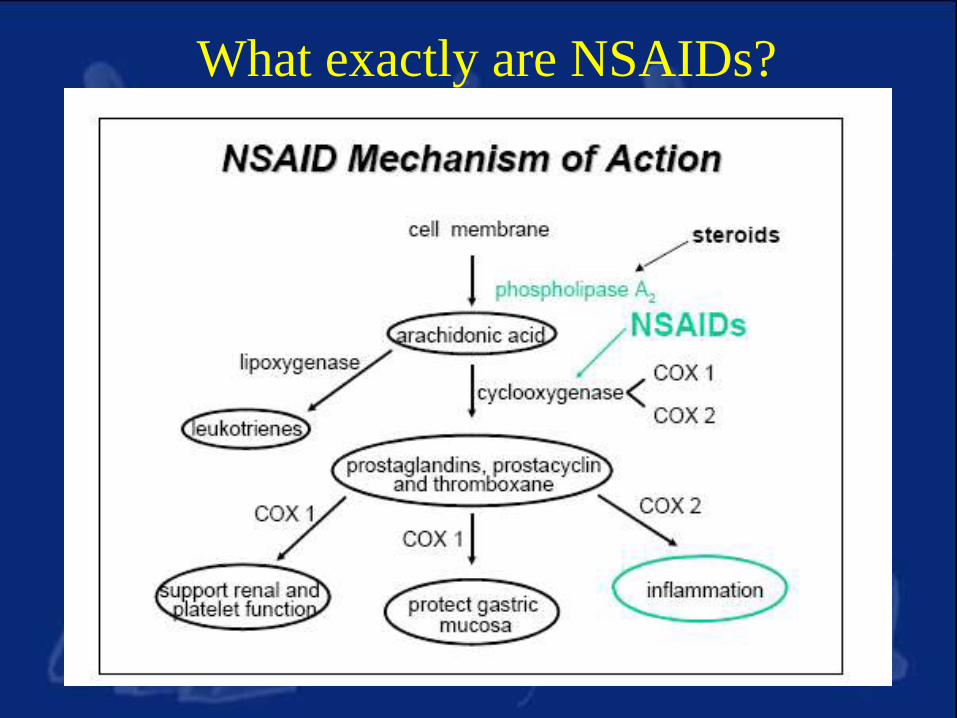
What exactly are NSAIDs?
3. Acid /Pepsin
By definition, peptic ulcer is caused by
autodigestion of acid and pepsin
Activity of pepsin is pH-depedent
Pepsinogen pepsin pH< 4
Maintaining activity pH< 4
Usual therapy toward suppression of acid
4. Smoking & Peptic UlcerIncreasing incidence of peptic ulcer
Delaying healing of ulcer
Increasing relapse and complication
Mechanisms:
Facilitating bile
reflux
Decreasing mucosal
blood supply
Inhibiting synthesis
of PGs
5. Genetics & Peptic Ulcer
Familial Clustering Genetic factors
Environment factor : H. pylori infection
Concordance of peptic ulcer is more
common in monozygotic that dizygotic
twins.
Peptic ulcer occurs in a few rare inherited
syndromes.
Gastrinoma
Mastocytosis
Genetics & Peptic Ulcer
6. Psychological Factor in Peptic Ulcer
Controversial
Possible mechanisms
through vagal mechanisms,
Stimulating acid secretion
Decreasing mucosal blood supply
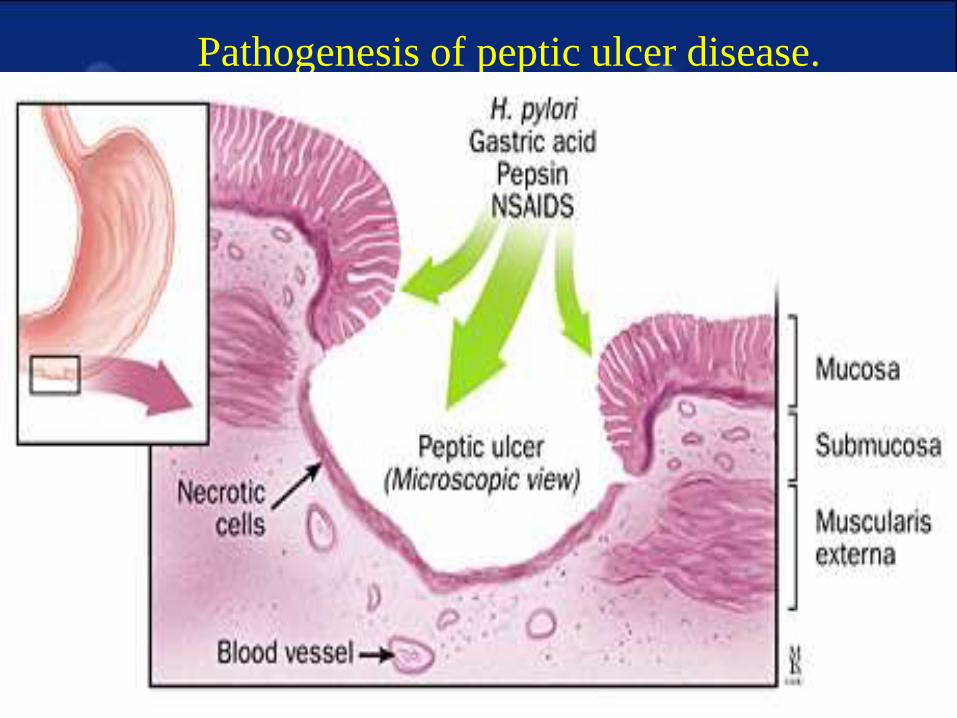
Pathogenesis of peptic ulcer disease.
Signs and symptoms
• Gastric ulcer: Usually sufferers are above age 40
1. Periodical pain occurs immediately after food and finally pain persists
2. Pain is felt over the umbilicus and left to midline and no radiation of pain is felt
3. Pain is relieved by vomiting or alkali foods
4. Fear of eating due to pain
5. Weight loss due to reduced intake
6. Hametemesis (blood vomiting) may be present
7. Sensation of feeling fullness, indigestion and heartburn noticed immediately after eating.
• Duodenal ulcer: Usually sufferers are between age group of 20-50.
1. Periodicity of pain is very marked
2. Pain is felt above umbilicus and right to the midline and it may radiate to back
3. Pain appears 1-2 hours after food i.e. Pain is felt when the stomach gets empty, so the pain is often felt during middle of the night or sleep which disturbs sleep
1. Pain is usually better after taking food
2. No weight loss will be there since patient feels better with eating and goes on eating
3. Black or bloody stools (melena) may be present
Differentials
• Biliary Colic
• Cholecystitis
• Cholelithiasis
• Gastritis, Acute
• Gastritis, Chronic
• Gastroesophageal Reflux Disease
• Mesenteric Artery Ischemia
• Myocardial Ischemia
• Pancreatic Cancer
• Pancreatitis, Acute
• Pancreatitis, Chronic
WORKUP
• Lab Studies:
–In most patients with
uncomplicated PUD, routine
laboratory tests are usually
unhelpful.
–Documentation of PUD depends on
radiographic and endoscopic
confirmation.
– If the diagnosis of PUD is unclear or
complicated and PUD is suspected,
obtaining CBC, liver function tests
(LFTs), amylase, and lipase might be
useful
Imaging Studies
• Upper gastrointestinal series
–Double-contrast radiography performed by an experienced radiologist might approach the diagnostic accuracy of upper GI endoscopy.
–However, it has been replaced largely by diagnostic endoscopy, when available.
–It is not as sensitive as endoscopy
for the diagnosis of small ulcers
(<0.5 cm).
–It does not allow for obtaining a
biopsy to rule out malignancy in
the setting of a gastric ulcer or to
assess for H pylori infection in the
setting of a gastroduodenal ulcer.
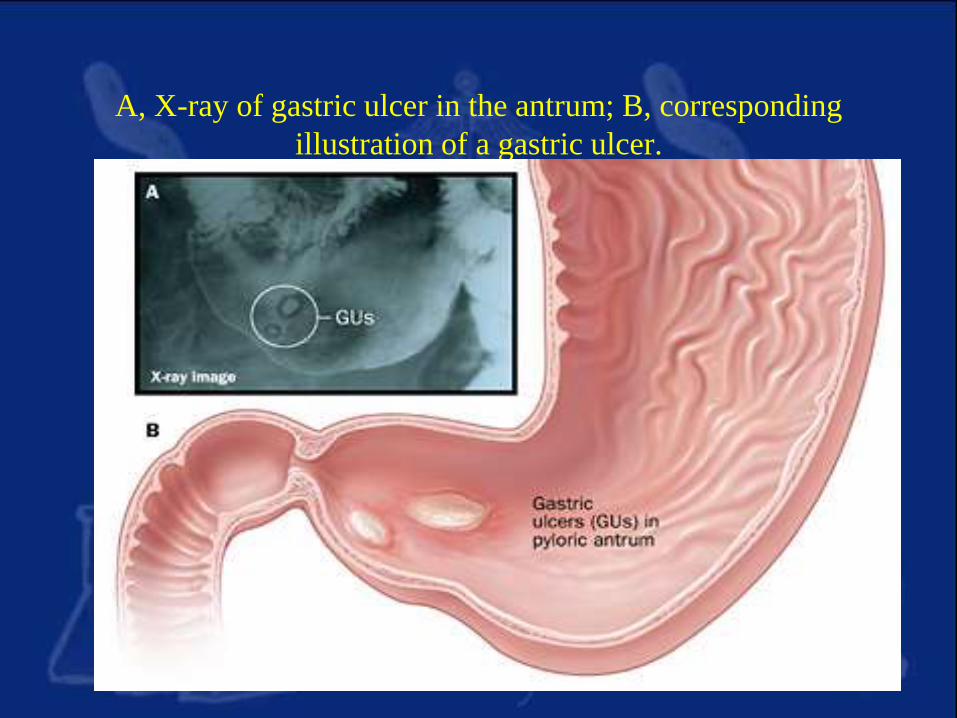
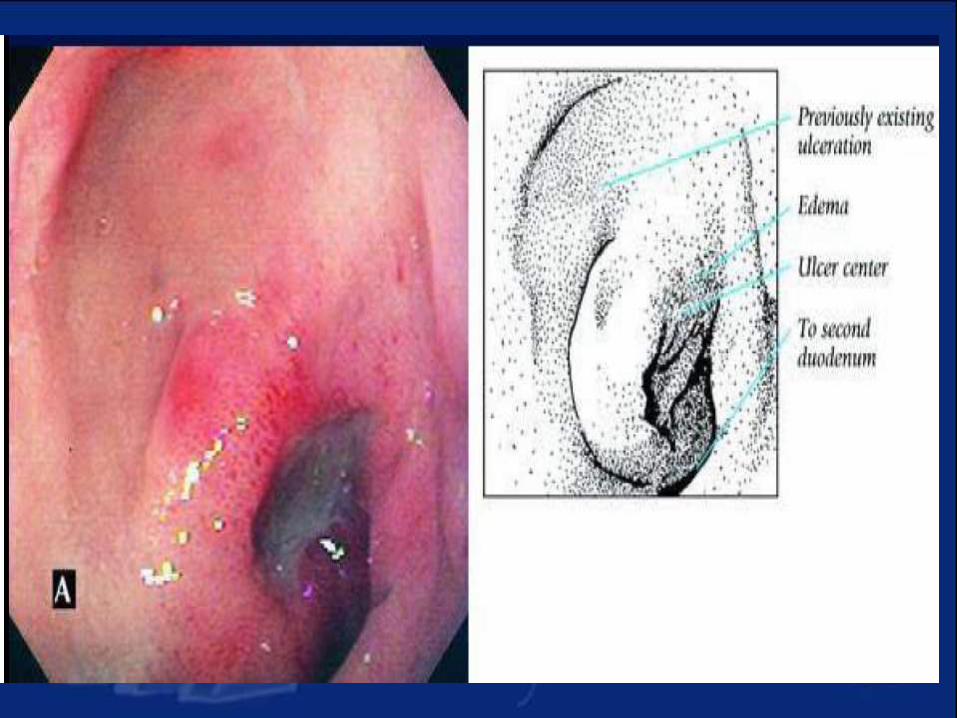
A, X-ray of gastric ulcer in the antrum; B, corresponding
illustration of a gastric ulcer.
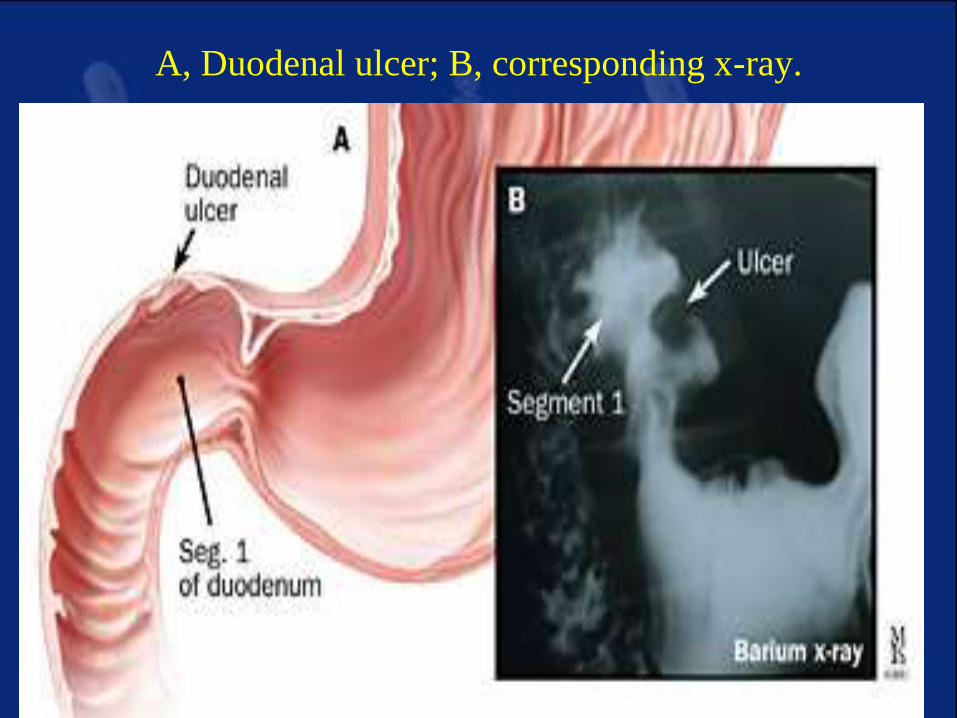
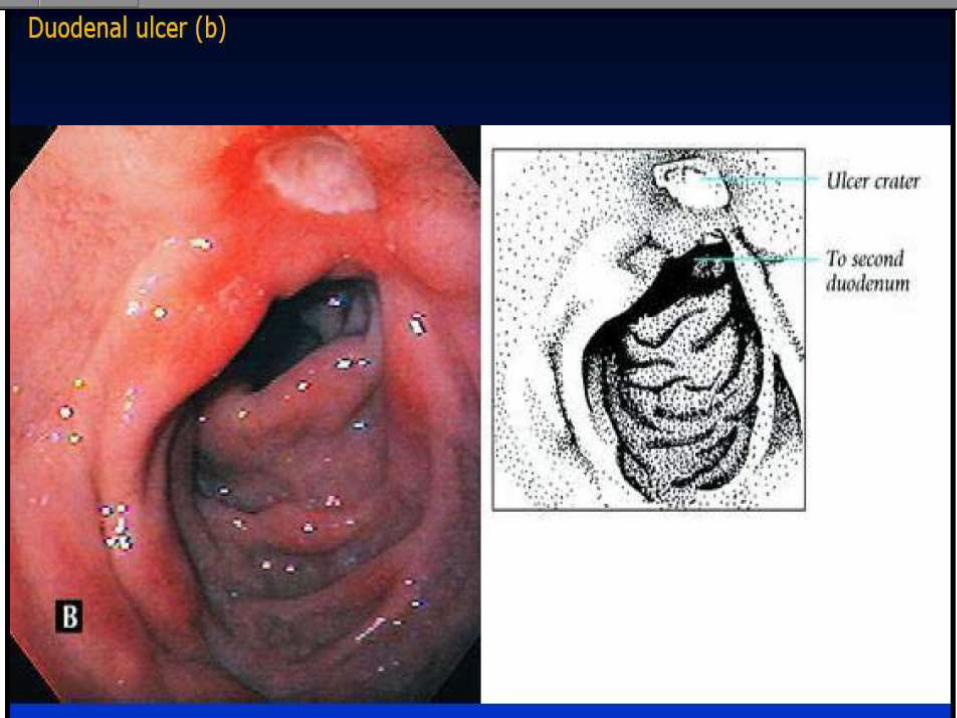
A, Duodenal ulcer; B, corresponding x-ray.
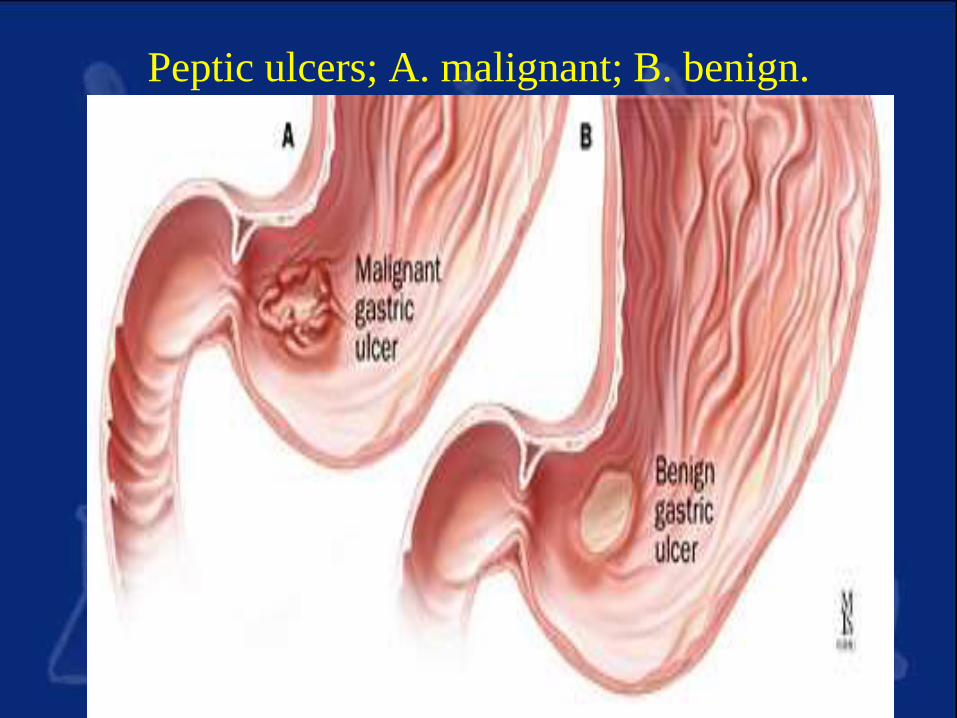
Peptic ulcers; A. malignant; B. benign.
Other Tests
• Detection of H pylori infection is
essential in all patients with peptic
ulcers.
• Endoscopic or invasive tests
include a rapid urease test,
histopathology, and culture.
–Rapid urease tests are considered
the endoscopic diagnostic test of
choice.
–The presence of H pylori in
gastric mucosal biopsy
specimens is detected by testing
for the bacterial product urease.
–One or more gastric biopsy
specimens are placed in the rapid
urease test kit.
–If H pylori are present, bacterial
urease converts urea to ammonia,
which changes pH and produces
a color change.
–Obtain histopathology, often
considered the criterion standard
for the diagnosis of H pylori, if
the rapid urease test result is
negative and a high suspicion for
H pylori persists (presence of a
duodenal ulcer).
–Culture primarily is used in
research studies and is not
available routinely for clinical
use.
• Nonendoscopic or noninvasive
tests include serum H pylori
antibody detection, fecal antigen
tests, and urea breath tests.
–Antibodies (immunoglobulin G
[IgG]) to H pylori can be
measured in serum, plasma, or
whole blood.
–Urea breath tests detect active H
pylori infection by testing for the
enzymatic activity of bacterial
urease.
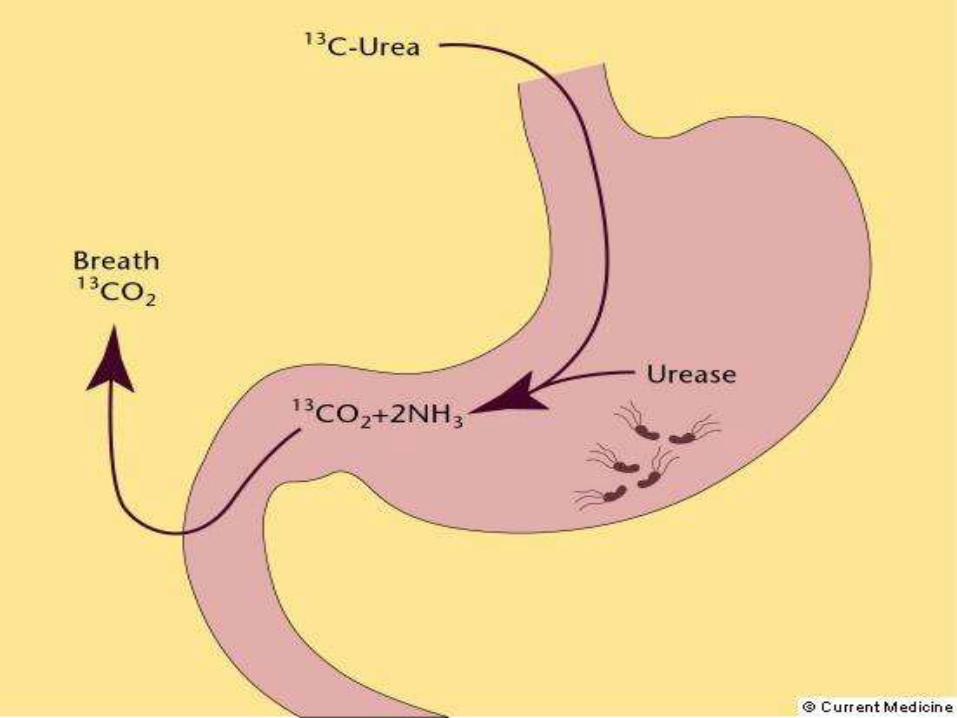
–In the presence of urease
produced by H pylori, labeled
carbon dioxide (heavy isotope,
carbon-13, or radioactive isotope,
carbon-14) is produced in the
stomach, absorbed into the
bloodstream, diffused into the
lungs, and exhaled.
–Fecal antigen testing identifies
active H pylori infection by
detecting the presence of H
pylori antigens in stools.
–This test is more accurate than
antibody testing and less
expensive than urea breath tests.
• Special studies
–Obtaining a serum gastrin is
useful in patients with recurrent,
refractory, or complicated PUD
and is useful in patients with a
family history of PUD to screen
for Zollinger-Ellison syndrome.
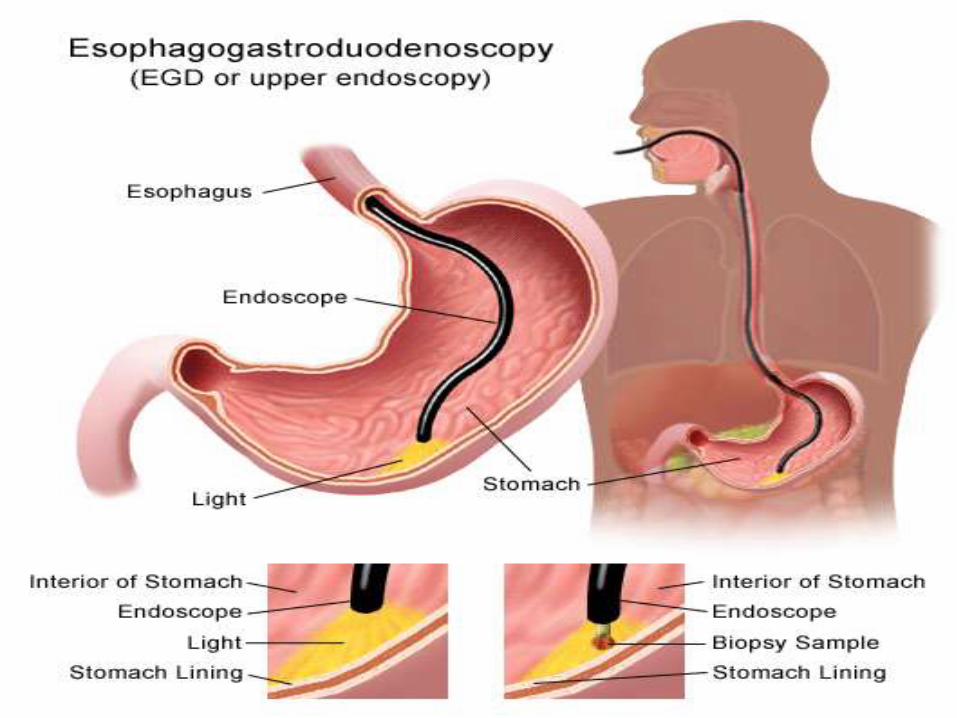
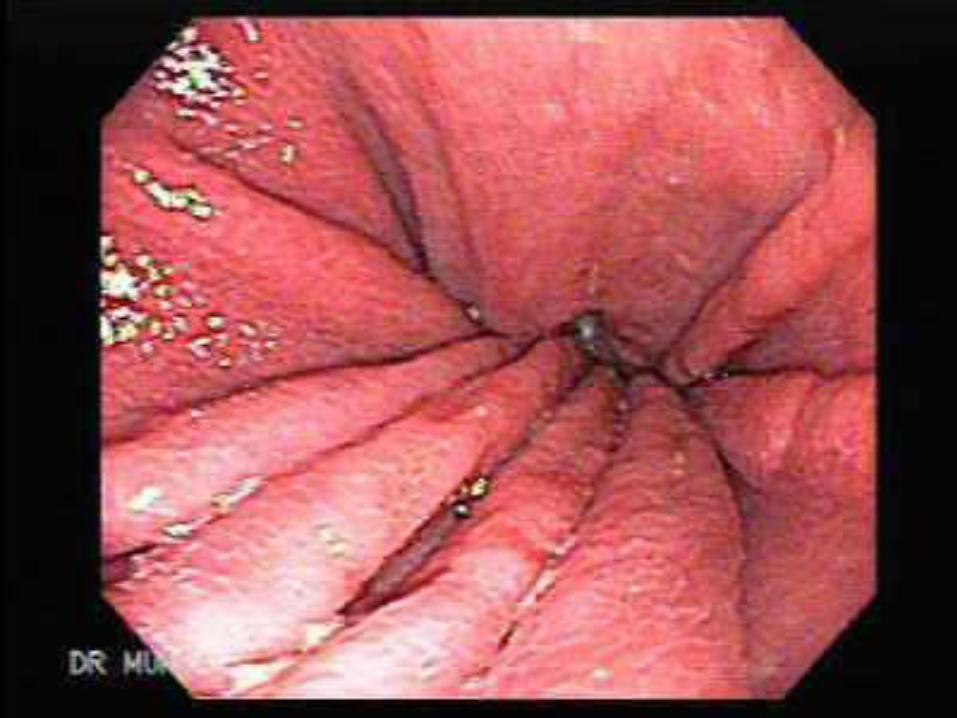
Procedures
• Upper GI endoscopy :
–Preferred diagnostic test in the
evaluation of patients with
suspected PUD
–Highly sensitive for the diagnosis
of gastric and duodenal ulcers.
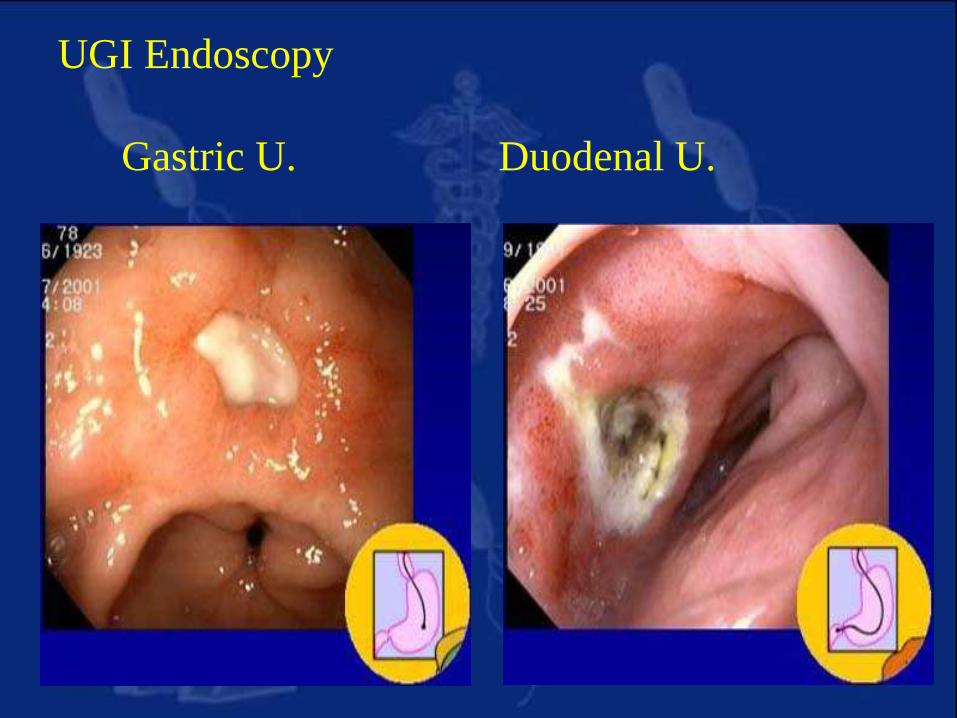
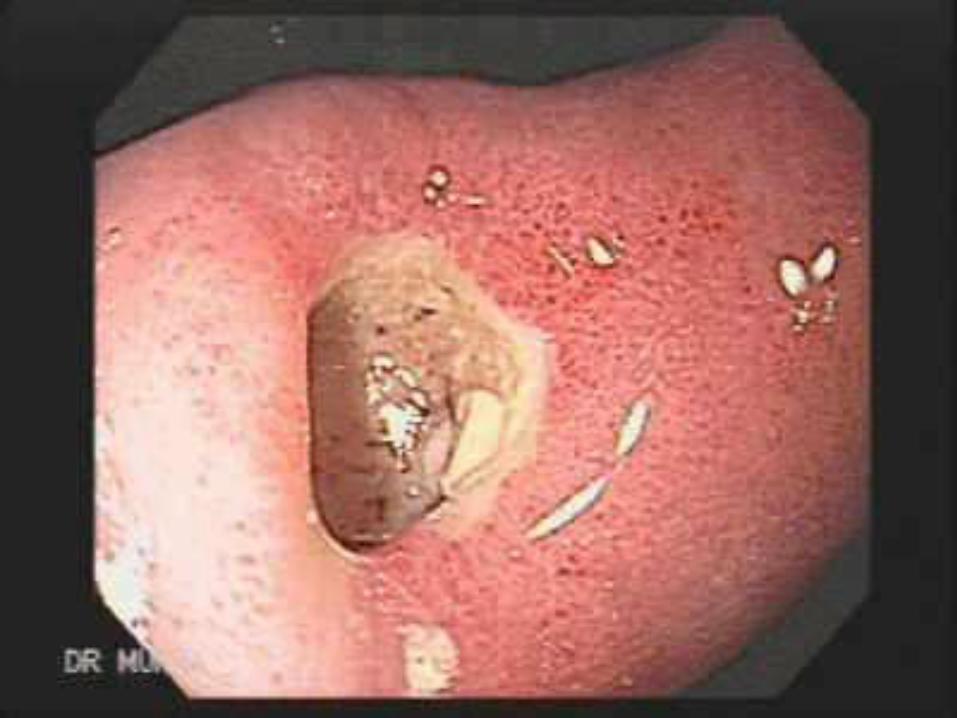
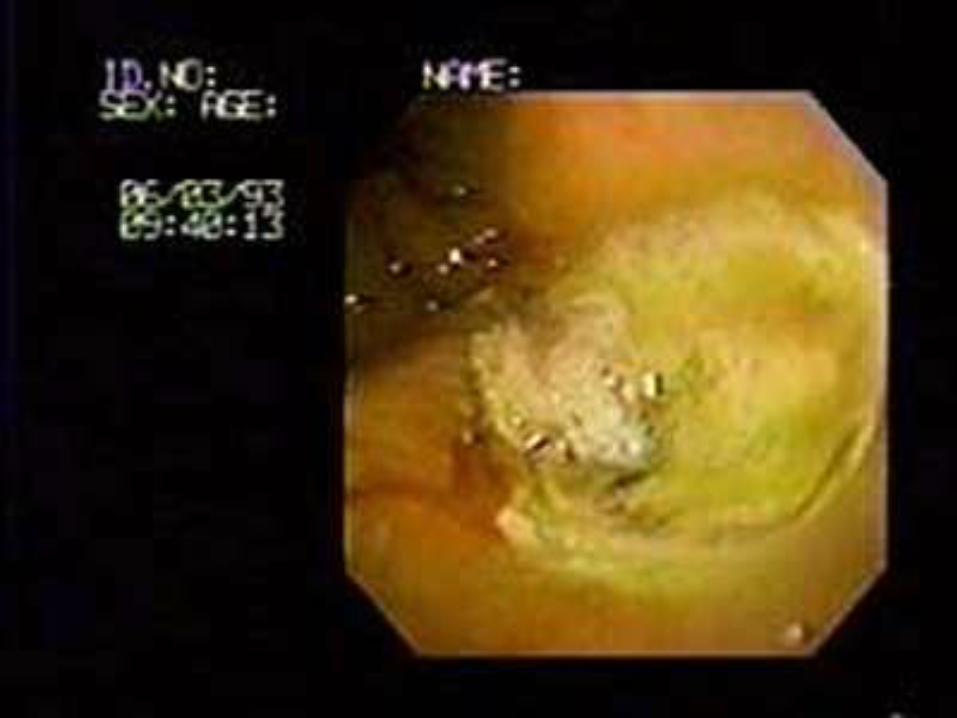
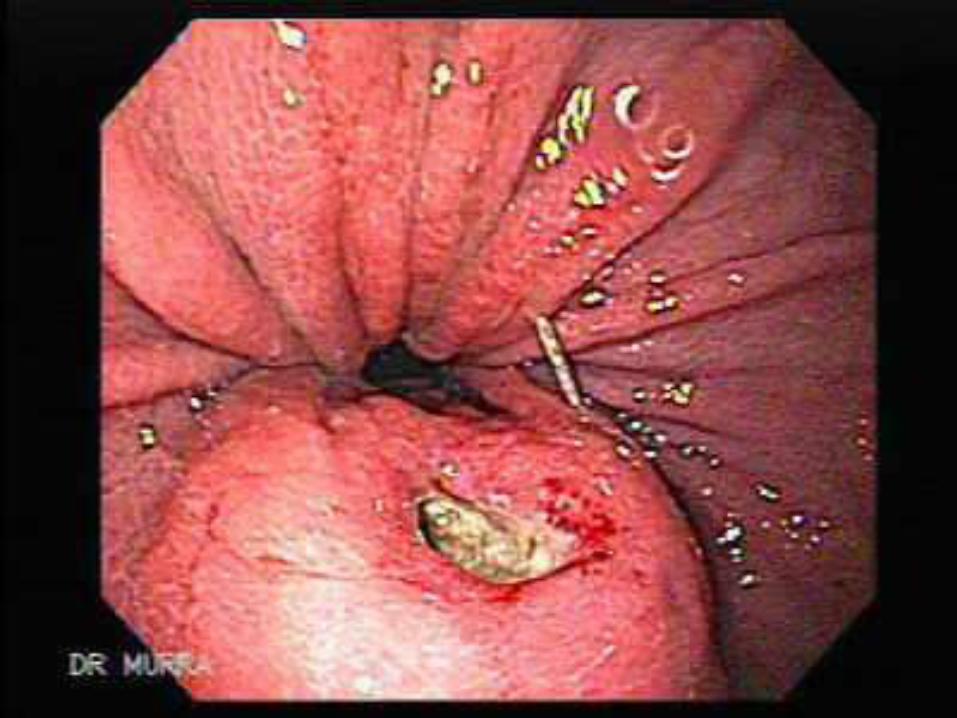
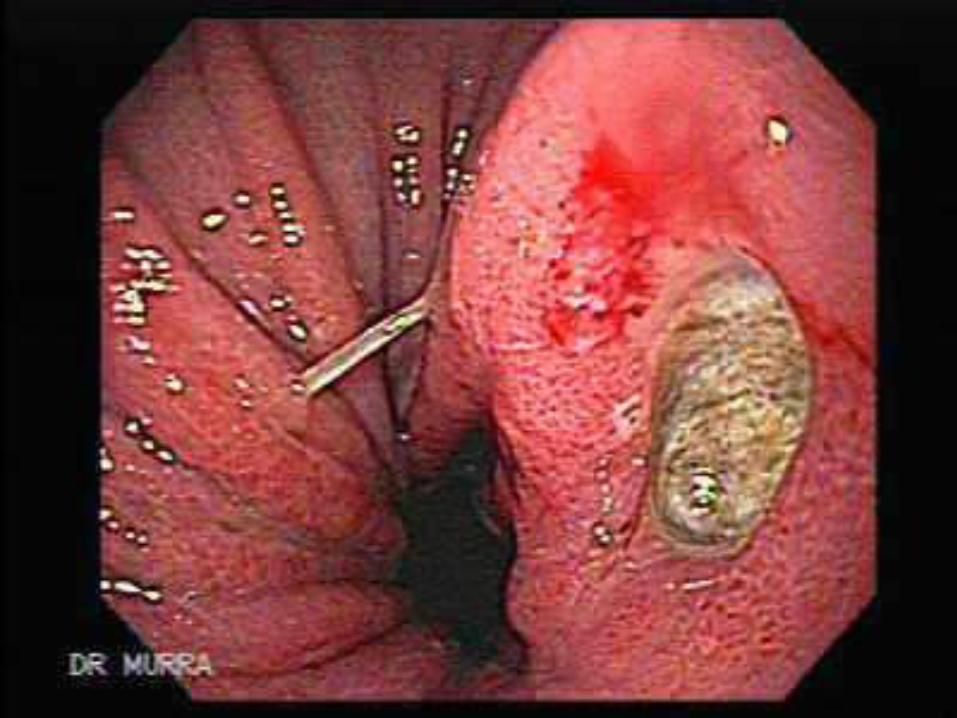
UGI Endoscopy
Gastric U. Duodenal U.





–Allows for biopsies and
cytologic brushings in the setting
of a gastric ulcer in order to
differentiate a benign ulcer from
a malignant lesion
–Allows for detection of H pylori
infection with antral biopsies for
a rapid urease test and/or
histopathology in patients with
PUD.


Complications
• Hemorrhage: Mild to severe hemorrhage is
the most common complication of peptic
ulcer disease.
• Symptoms include hematemesis (vomiting
of fresh blood or "coffee ground" material);
passage of bloody or black tarry stools
(hematochezia and melena, respectively);
and weakness, orthostasis, syncope, thirst,
and sweating caused by blood loss.
• Other Complications:
–Perforation
–Penetration
–Obstruction
Prognosis
• When the underlying cause is
addressed, the prognosis is
excellent. Most patients are
treated successfully with the cure
of H pylori infection, avoidance
of NSAIDs, and the appropriate
use of antisecretory therapy.
• Cure of H pylori infection
changes the natural history of
the disease, with a decrease in
the ulcer recurrence rate from
60-90% to approximately 10-
20%.
TREATMENT
• Given current understanding of the
pathogenesis of PUD, the majority
of patients with PUD are treated
successfully medically with cure of
H. pylori infection and/or
avoidance of NSAIDs, along with
appropriate use of antisecretory
therapy.
• A number of treatment options exist
for patients presenting with
symptoms suggestive of PUD or
ulcerlike dyspepsia, including
empiric antisecretory therapy,
empiric triple therapy for H pylori
infection, endoscopy followed by
appropriate therapy based on
findings, and H pylori serology
followed by triple therapy for
infected patients.
• Breath testing for active H pylori
infection may be used.
• Perform endoscopy early in
patients older than 45-50 years and
in patients with associated so-
called alarm symptoms, such as
dysphagia, recurrent vomiting,
weight loss, or with signs of
bleeding.
MEDICATION
• Treat all patients with peptic ulcers
and associated H pylori infection
with triple therapy, which results in
a cure rate of infection and healing
in approximately 85-90% of cases.
• In addition to effectiveness,
consider compliance, adverse
effects, drug interactions, and cost
when choosing a regimen.
• Treat NSAID-induced ulcers with
cessation of NSAIDs, if possible,
and an appropriate course of
standard ulcer therapy with a
histamine 2 (H2)–receptor
antagonist or a proton pump
inhibitor.
• If NSAIDs are continued, prescribe
a proton pump inhibitor.
• H pylori–negative ulcers that are
not caused by NSAIDs can be
treated with appropriate
antisecretory therapy, either H2-
receptor antagonists or proton
pump inhibitors.
• Begin testing for other causes.
• Drug Category: Triple therapies
for H pylori infection -- Triple
therapy for 14 days is considered
the treatment of choice for H pylori
infection.
• Two forms of triple therapy are
available, including proton pump
inhibitor–based triple therapy and
bismuth-based triple therapy.
• Proton pump inhibitor–based triple
therapy consists of a proton pump
inhibitor and 2 antibiotics, each bid
for 2 weeks.
• In the setting of an active ulcer,
continue qd proton pump inhibitor
therapy for additional 2 weeks.
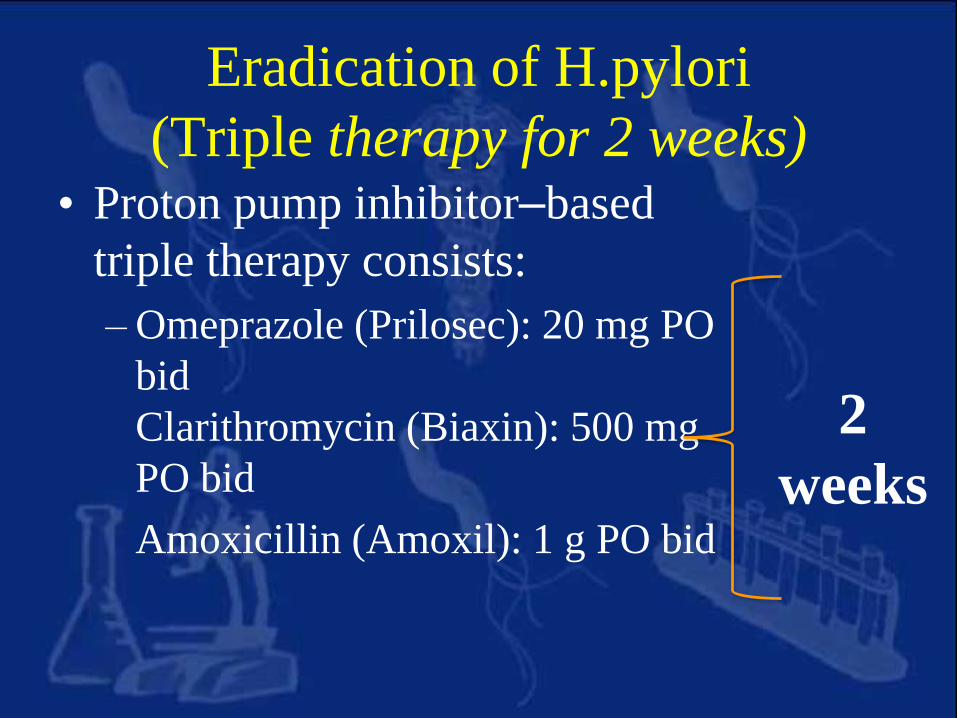
Eradication of H.pylori
(Triple therapy for 2 weeks)• Proton pump inhibitor–based
triple therapy consists:
– Omeprazole (Prilosec): 20 mg PO
bid
Clarithromycin (Biaxin): 500 mg
PO bid
Amoxicillin (Amoxil): 1 g PO bid
2
weeks
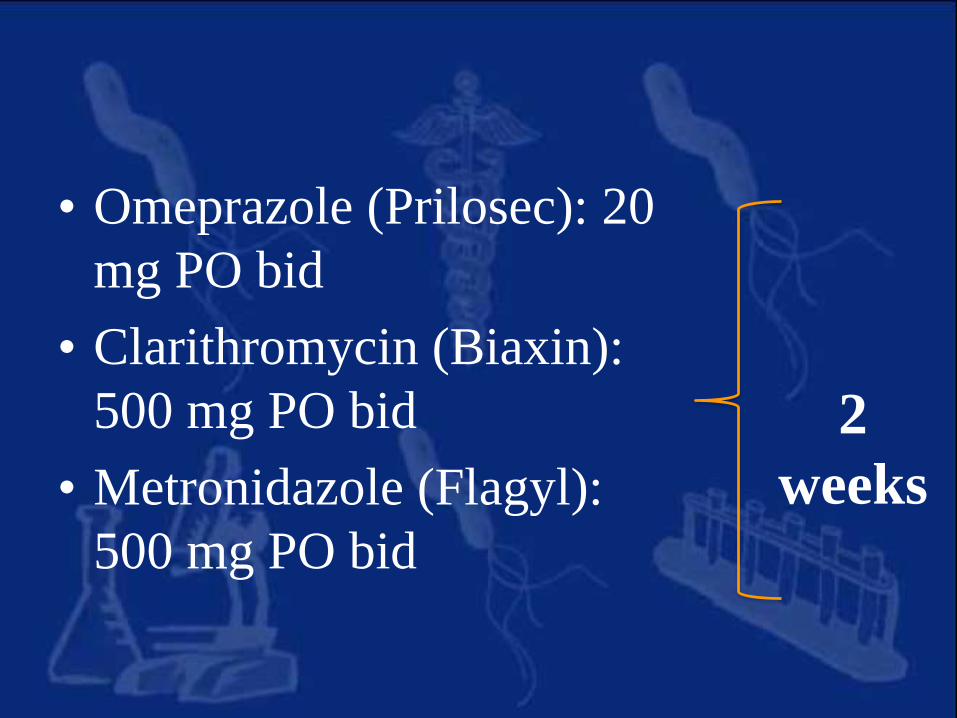
• Omeprazole (Prilosec): 20
mg PO bid
• Clarithromycin (Biaxin):
500 mg PO bid
• Metronidazole (Flagyl):
500 mg PO bid
2
weeks
• Omeprazole (Prilosec): 20 mg PO bid
• Amoxicillin (Amoxil): 1 g PO bid
• Metronidazole (Flagyl): 500 mg PO bid
2
weeks
Diet
• Soft bland diet. It is better to be small and
frequent.
• Avoid irritant foods and smoking.
• Avoid excessive milk intake as it may
increase acidity due to its calcium content.
H2 Blockers:
For 4.-6 weeks to ensure ulcer healing)
• Ranitidine (ZantaC®) 300 mg/D.
• Famotidine (Antodine®) 20-40 mg/D .
PPI ( For 4 -8 Weeks)
• Omeprazole 20 mg/D.
• Pantoprazole 40 mg/D.
• Lanzoprazole 30 mg/D.
Surgical treatment of PUD
• Indication for surgery:-
– Failure of medical treatment.
– Recurrent uncontrollable hemorrhage.
– Perforation or penetration.
– Pyloric obstruction.
– Possible malignancy (See gastric carcinoma) .
Types of Surgery
1. Partial gastrectomy:
– Billroth I - the lower part of the stomach is
removed and stomach remnant is connected to
duodenum (a)
– Billroth II - the remnant of the stomach is
connected to the first loop of jejunum
(polyagastrectomy) (b).
2. Highly selective vagotomy (c)
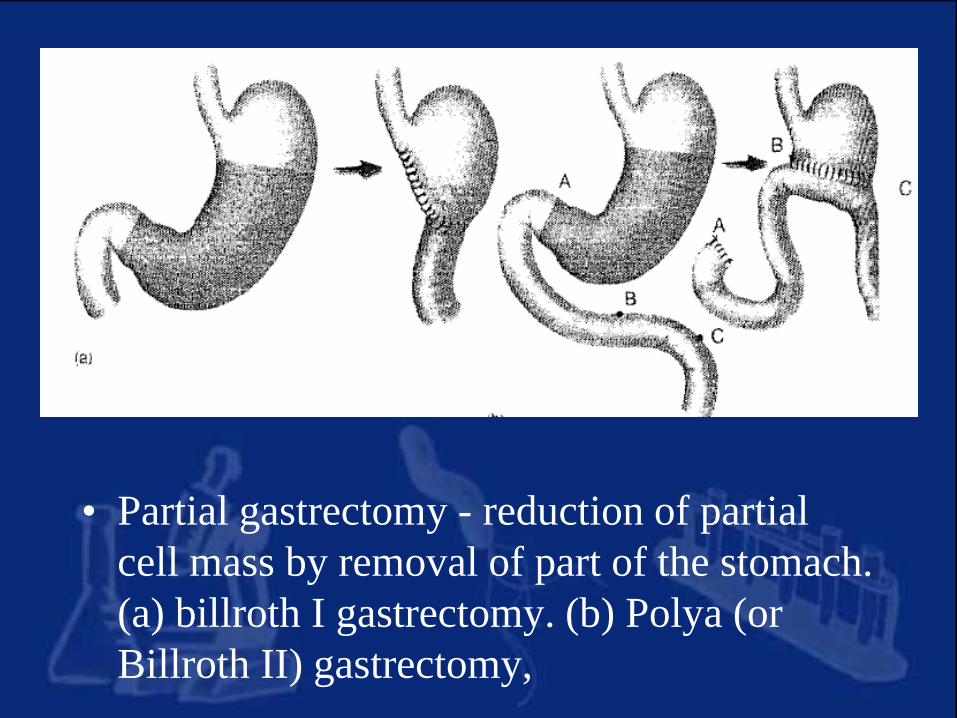
• Partial gastrectomy - reduction of partial
cell mass by removal of part of the stomach.
(a) billroth I gastrectomy. (b) Polya (or
Billroth II) gastrectomy,
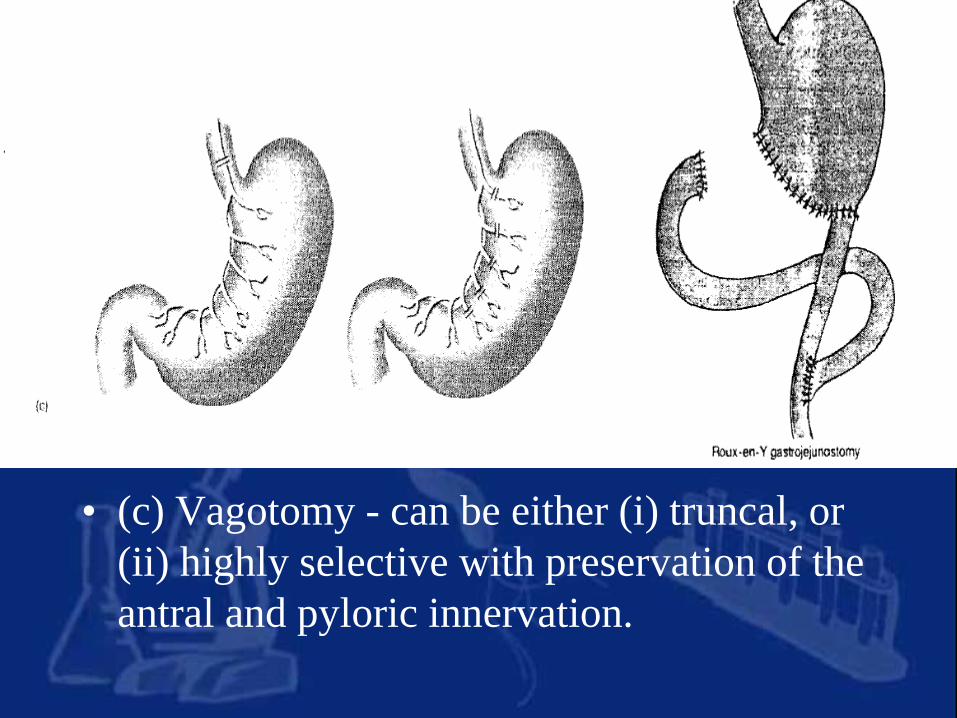
• (c) Vagotomy - can be either (i) truncal, or
(ii) highly selective with preservation of the
antral and pyloric innervation.
Treatment of Complication
• 1. Hemorrhage:• - Omeprazole: by I.V infusion or ranitidine infusion.
• - Endoscopic injection of adrenaline or use of heater
probe or laser therapy.
• - Blood transfusion: to restore the blood volume
rapidly.
• - Surgery: for resistant cases.
• 2. Perforation or penetretion: nasogastric
suction, IV fluids, antibiotics & analgesics,
surgery is performed to repair the
perforation with omental patch and drain
the abdomen.
Further Outpatient Care
• Endoscopy is required to document
healing of gastric ulcers and to rule
out gastric cancer.
• This usually is performed 6-8
weeks after the initial diagnosis of
PUD.
• Documentation of H pylori cure
with a noninvasive test, such as the
urea breath test or fecal antigen
test, is appropriate in patients with
complicated ulcers.
Prevention
• Primary prevention of NSAID-
induced ulcers includes the
following:
–Avoid unnecessary use of NSAIDs and
Use the lowest effective dose of an
NSAID.
–Use acetaminophen or nonacetylated
salicylates when possible.
Patient Care
Patient education
• Smoking delays ulcer healing
• Anticholinergics, TCAs, Ca channelblockers decrease lower oesophagealsphincter tone giving rise to GERD,eventually leading to oesophagitis.
• Patients should be warned of GIT riskbefore beginning NSAID or aspirin
• Patients sensitive to penicillin need aneradication regimen without amoxicillin
• Patients receiving eradication therapyshould be advised of the need of acombination of three drugs for a shortperiod of time.
Patient monitoring• Treatment success in peptic ulcer disease is
measured by review of the patient in termsof symptom control.
• Following eradication therapy, somepatients continue to experience symptoms ofabdominal pain.
• Patients should be reassured that thesesymptoms will resolve spontaneously.
• Anaemic patients following bleeding ulcerare prescribed iron therapy
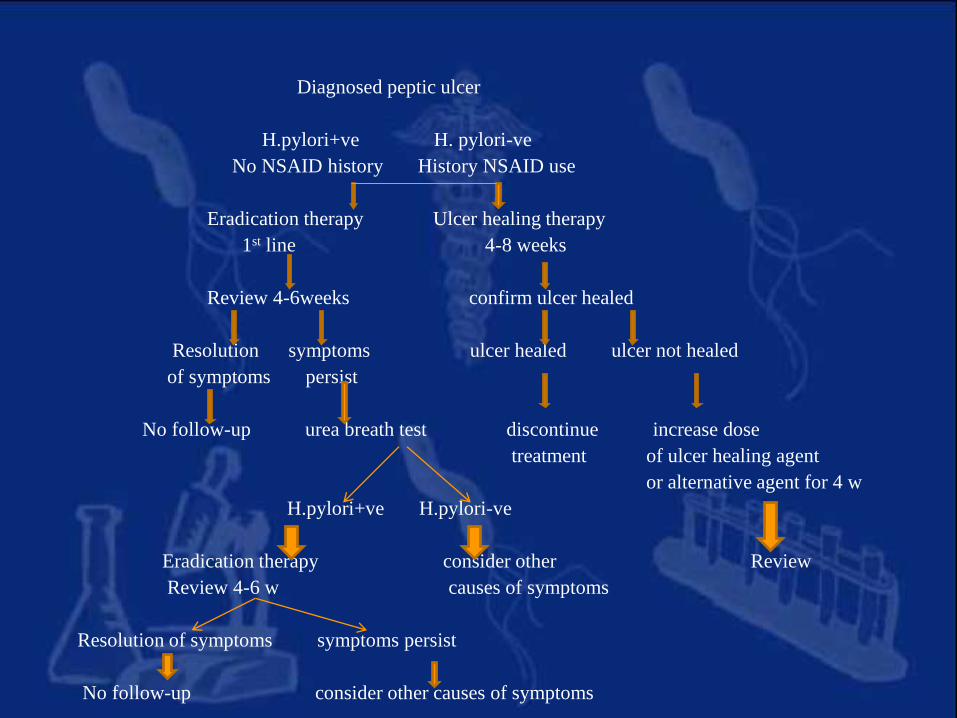
Diagnosed peptic ulcer
H.pylori+ve H. pylori-ve
No NSAID history History NSAID use
Eradication therapy Ulcer healing therapy
1st line 4-8 weeks
Review 4-6weeks confirm ulcer healed
Resolution symptoms ulcer healed ulcer not healed
of symptoms persist
No follow-up urea breath test discontinue increase dose
treatment of ulcer healing agent
or alternative agent for 4 w
H.pylori+ve H.pylori-ve
Eradication therapy consider other Review
Review 4-6 w causes of symptoms
Resolution of symptoms symptoms persist
No follow-up consider other causes of symptoms
Future treatment
• Immunization against H. pylori will be a
future option in the management of peptic
ulcer disease.
OVERVIEW
• A peptic ulcer is disruption in a
segment of the GI mucosal integrity,
typically in the stomach (gastric
ulcer) or the first few centimeters of
the duodenum (duodenal ulcer).
• Nearly all ulcers are caused by
Helicobacter pylori infection or
NSAID use.
• Symptoms typically include burning
epigastric pain that is often relieved
by food.
• Diagnosis is by endoscopy and
testing for H. pylori. Treatment
involves acid suppression,
eradication of H. pylori (if present),
and avoidance of NSAIDs.