Embed Size (px)
Citation preview
Esophageal Diverticula
Dr. Aiydarus Ali Ahmed ( Fowzi )
Medical Doctor of Internal Medicine
and SurgeryMBBS, MD
Lecture 4 ESOPHAGEAL DIVERTICULA
ESOPHAGEAL DIVERTICULA
• An esophageal diverticulum is an outpouching of mucosa through the muscular layer of the esophagus
• It can be asymptomatic or cause dysphagia and regurgitation.
• Diagnosis is made by barium swallow; surgery is rarely required.
• There are several types of esophageal diverticula, each of different origin.

Types of esophageal diverticula.
1. Upper esophageal, also called Zenker's diverticulum (which is arguably a hypopharyngeal lesion; this could be a trick question).
2. Mid-esophageal, also called traction diverticulum.
3. Distal esophageal, also called epiphrenic diverticulum.

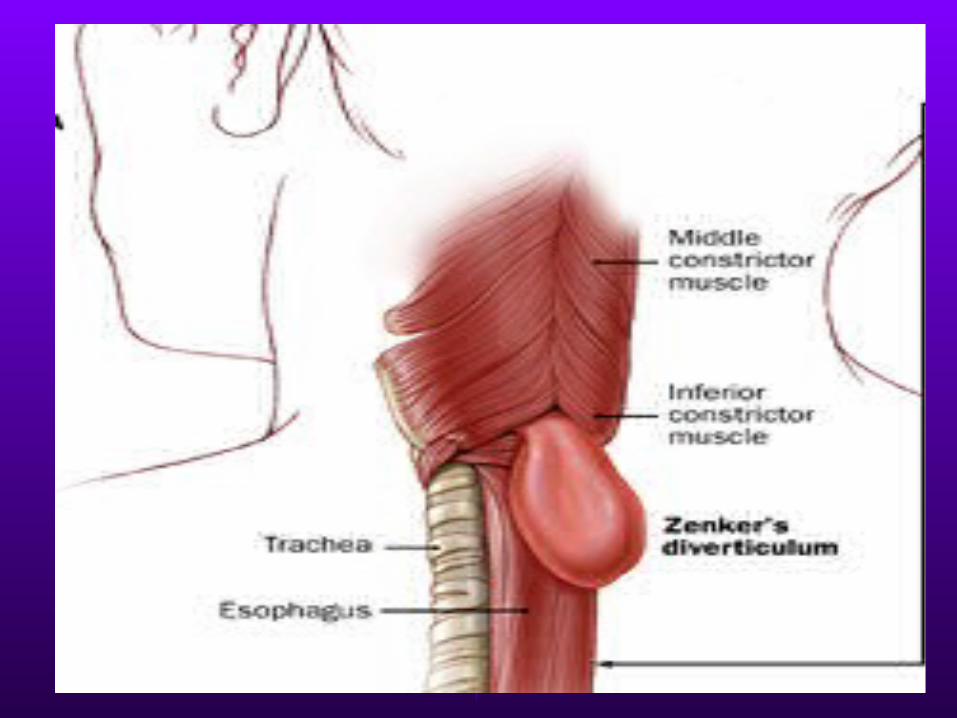
Zenker's (pharyngeal) diverticula
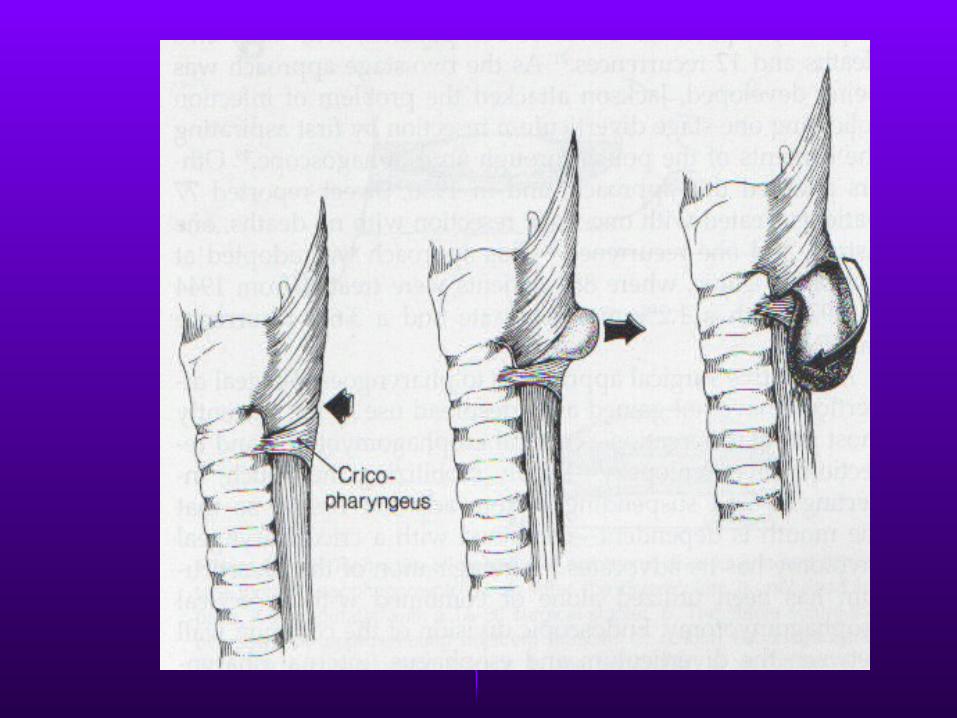
• Zenker's (pharyngeal) diverticula are posterior outpouchings of mucosa and submucosa through the cricopharyngeal muscle, probably resulting from an incoordination between pharyngeal propulsion and cricopharyngeal relaxation.
What causes Zenker's diverticulum?
• This has been long debated, with initially contradictory studies. The lesion is more common in elderly patients.
• Impaired cricopharyngeal compliance, usually caused by fibrotic changes, causes increased intrabolus pressure with swallowing.
•Relaxation of the upper esophageal sphincter (UES) is usually normal. The result is increased hypopharyngeal pressure, with herniation at a weak point just above the cricopharyngeus.
What is the typical history of Zenker's diverticulum?
• Patients may complain of regurgitation of undigested food, bad breath, a visible lump on the side of the neck, and dysphagia in the lower neck area.
• Midesophageal (traction) diverticula are caused by traction from mediastinal inflammatory lesions or, secondarily, by motility disorders.
• Epiphrenic diverticula occur just above the diaphragm and usually accompany a motility disorder (achalasia, diffuse esophageal spasm).
Symptoms and Signs
• Traction and epiphrenic diverticula are rarely symptomatic, although their underlying cause may be.
Diagnosis and Treatment
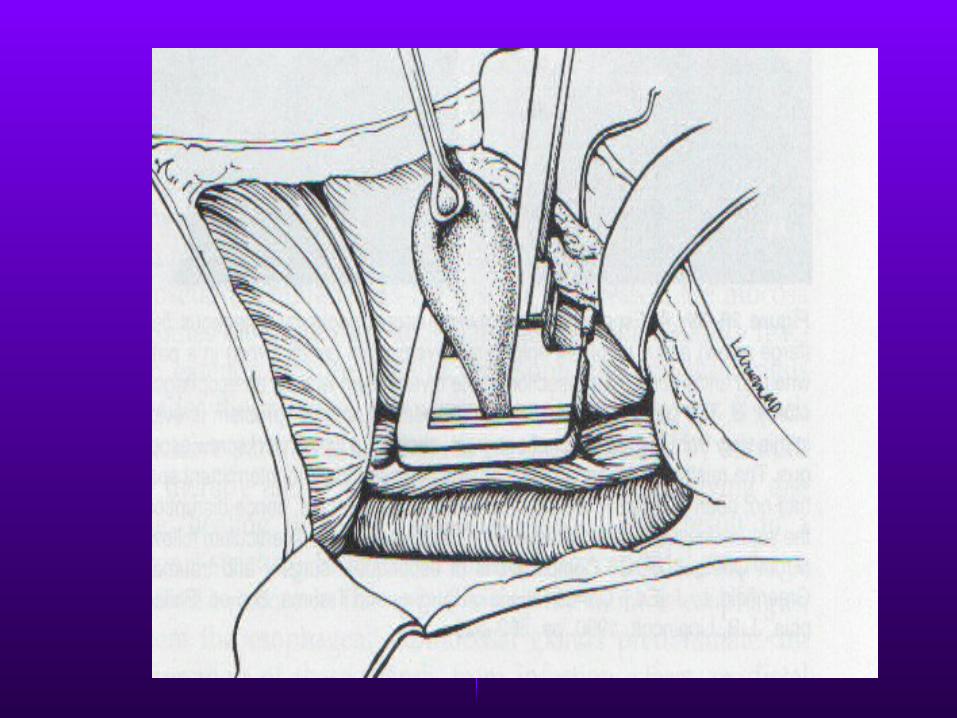
• All diverticula are diagnosed by video taped barium swallow. Specific treatment is usually not required, although resection is occasionally necessary for large or symptomatic diverticula.
• Diverticula associated with motility disorders require treatment of the primary disorder.
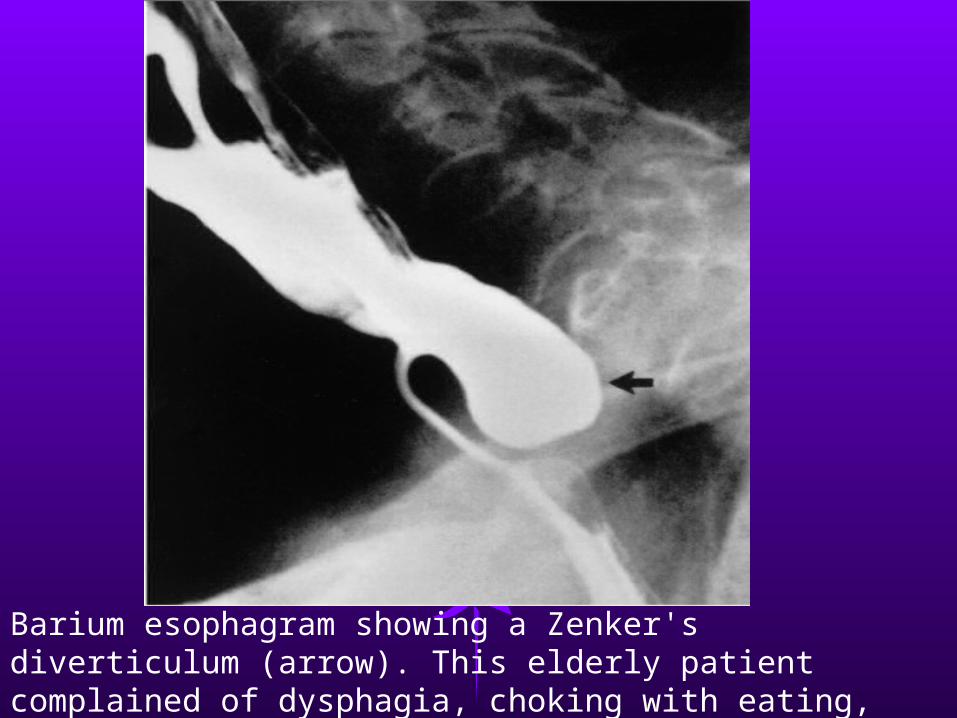
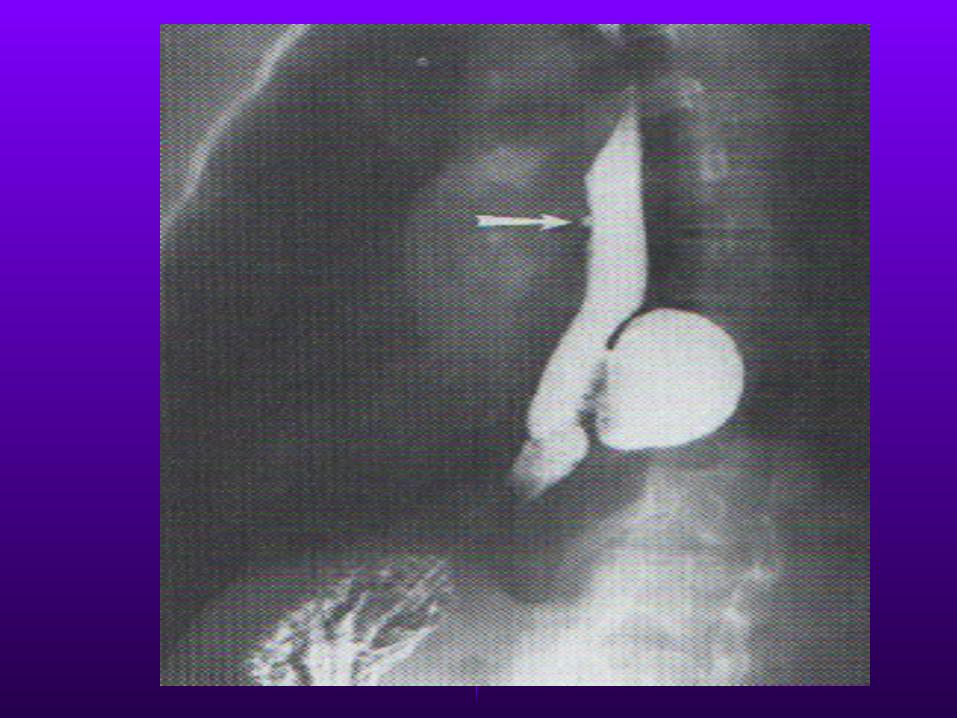
Barium esophagram showing a Zenker's diverticulum (arrow). This elderly patient complained of dysphagia, choking with eating, and recurrent pneumonia.
• For example, case reports suggest the performance of cricopharyngeal myotomy at the time of resection of a Zenker’s diverticulum.
Diverticula of the Esophagus
OVERVIEW
Esophageal Diverticula
• Almost all are acquired and occur predominantly in adulthood
• Are classified according to their:• Site of occurrence
1. Pharyngoesophageal2. Parabronchial3. Epiphrenic
• Wall thickness•True•False
• Mechanism of formation•Pulsion•Traction
Pharyngoesophageal Diverticula (Zenker)
• The most common esophageal diverticulum
• Occurs between the ages of 30-50 (believed to be acquired)
• Arises within the inferior pharyngeal constrictor, between the oblique fibers of the thyropharyngeus muscle and the cricopharyngeus muscle

• Is a pulsion diverticulum• Complaints are of cervical
dysplasia, effortless regurgitation of food or pills sometimes consumed hours earlier
• Sometimes a gurgling sensation in the neck after swallowing is felt
KEY POINTS: FOUR SYMPTOMS OF ZENKER'S DIVERTICULUM
• Regurgitation of undigested food • Bad breath • Lump on side of neck • Dysphagia in lower neck
Diagnosis and Treatment
• Barium swallow establishes the diagnosis
• Surgery is indicated in symptomatic patients regardless of the size
• It is the degree of cricopharyngeal muscle dysfunction and not the size of the diverticulum that determines the relative severity of cervical dysphagia
Midesophageal (Traction) Diverticula
• Are typically associated with mediastinal granulomatous disease (TB, histoplasmosis)
• They are usually small with a blunt tapered tip that points upward
• These are usually an incidental finding on barium swallow

• They rarely cause symptoms or require treatment
• Need to be differentiated from pulsion diverticula which can also occur in this location (associated with neuromotor esophageal dysfunction)
Epiphrenic (Supradiaphragmatic)
Diverticula
• Generally occur within the distal 10cm of the thoracic esophagus
• These are pulsion diverticula that arise due to esophageal motor dysfunction or mechanical distal obstruction
• Many patients are asymptomatic when diagnosed
• When symptomatic their symptoms are difficult to differentiate from: hiatal hernia, DES, achalasia, reflux esophagitis and carcinoma
• Dysphagia and regurgitation are common symptoms
Diagnosis and Treatment
• Diagnosis is easily made with barium swallow
• Esophageal function studies should also be performed to rule out any motor disturbances
• Lesions < 3 cm often require no treatment
• Extreme symptomatic patients sometimes require surgical repair

Swallow Carefully!!

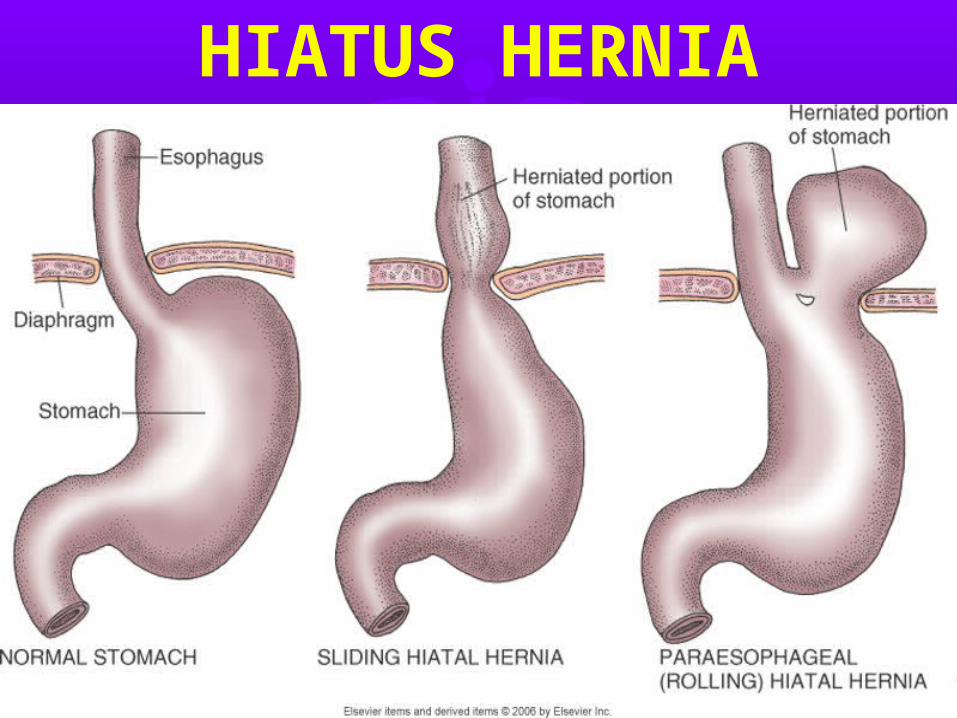
HIATUS HERNIA
Definition• Hiatus hernia is a protrusion of the
stomach through the diaphragmatic hiatus.
• Most hernias are asymptomatic, but an increased incidence of acid reflux may lead to symptoms of gastroesophageal reflux disease (GERD).
• Diagnosis is by barium swallow. Treatment is directed at symptoms of GERD if present.
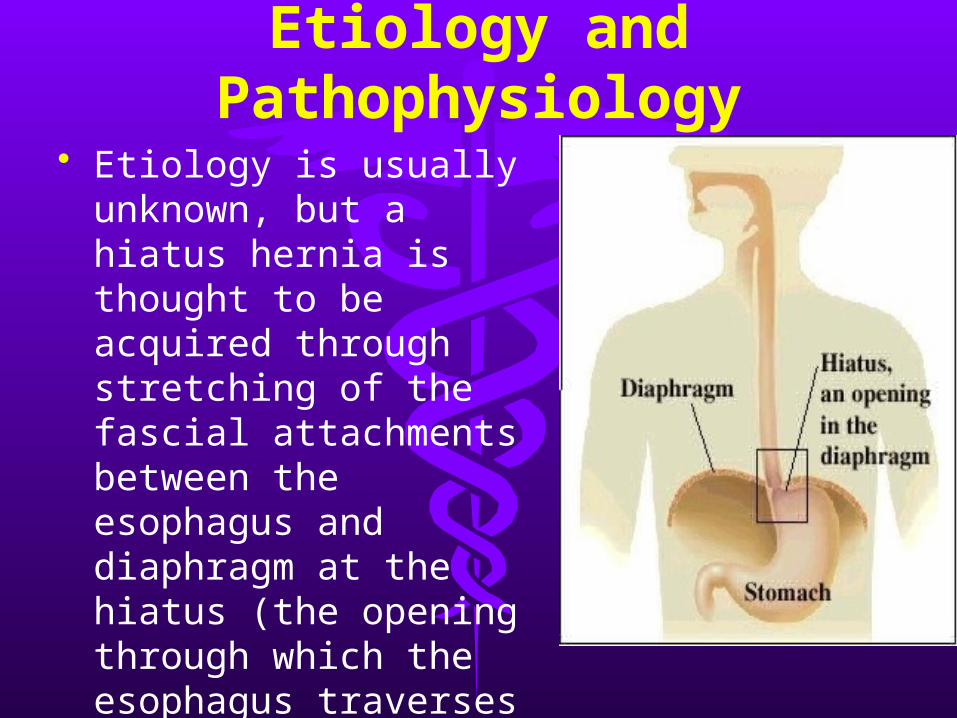
Etiology and Pathophysiology
• Etiology is usually unknown, but a hiatus hernia is thought to be acquired through stretching of the fascial attachments between the esophagus and diaphragm at the hiatus (the opening through which the esophagus traverses the diaphragm)
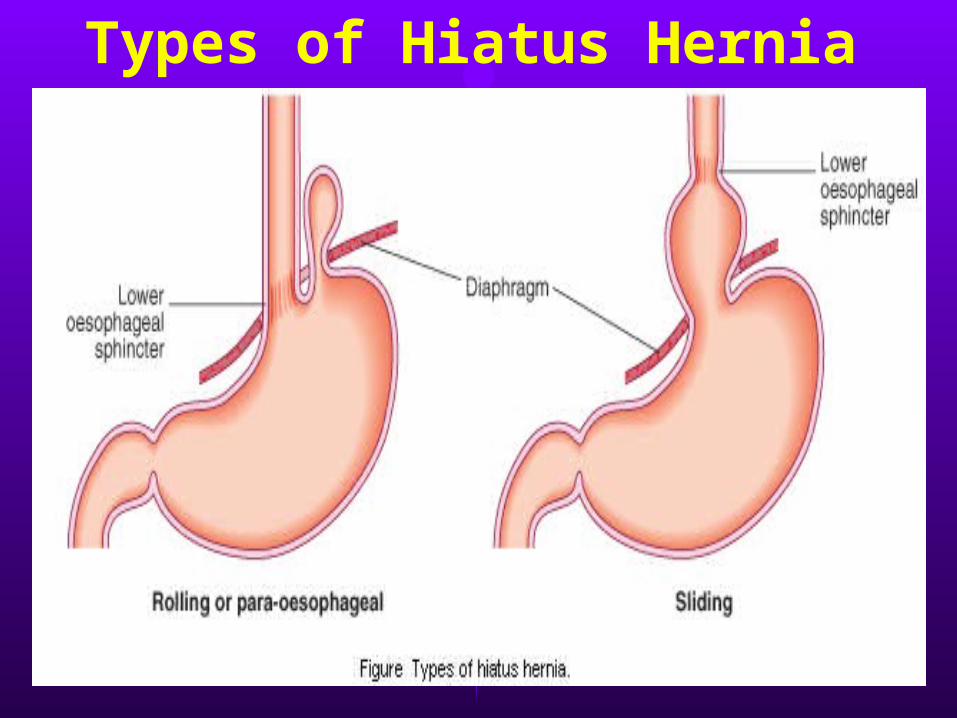
Types of Hiatus Hernia
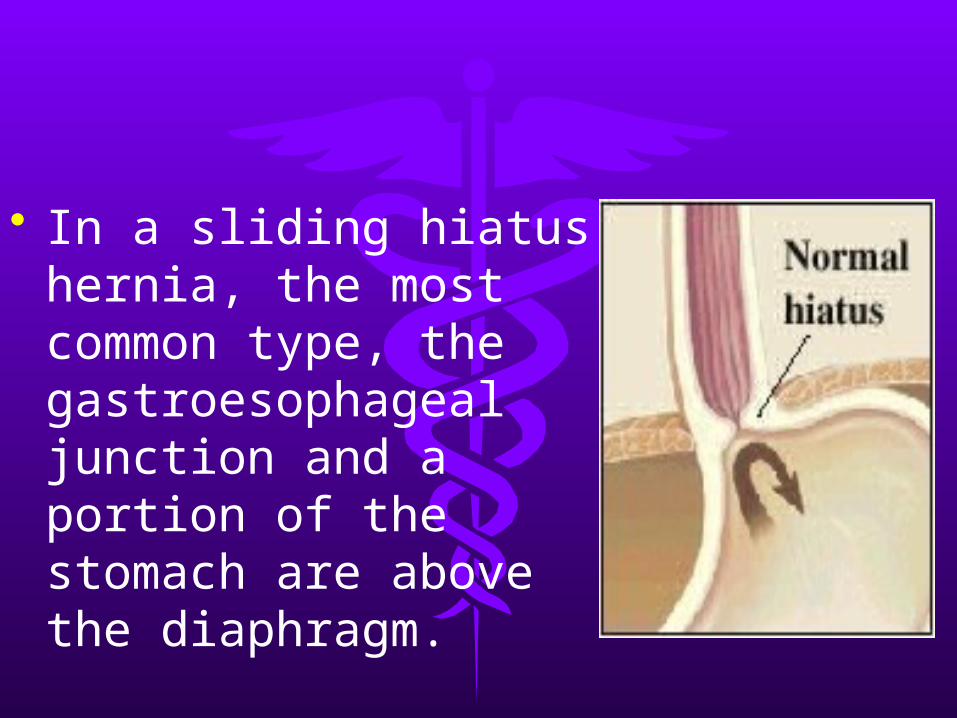
• In a sliding hiatus hernia, the most common type, the gastroesophageal junction and a portion of the stomach are above the diaphragm.
• Hernias may also occur through other parts of the diaphragm
• In a paraesophageal hiatus hernia, the gastroesophageal junction is in the normal location, but a portion of the stomach is adjacent to the esophagus.
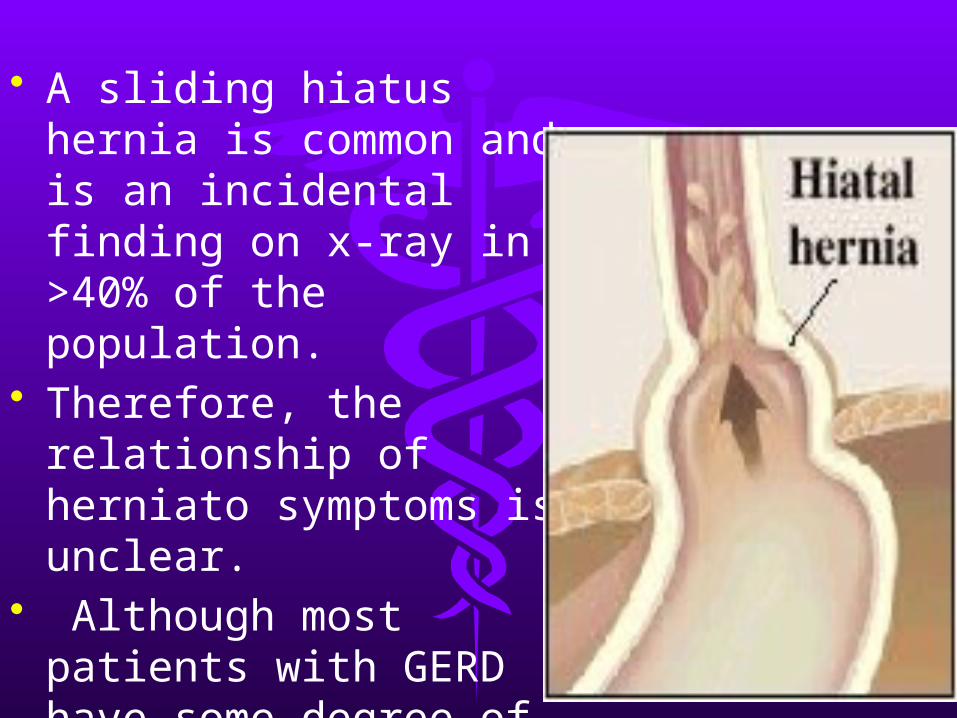
• A sliding hiatus hernia is common and is an incidental finding on x-ray in >40% of the population.
• Therefore, the relationship of herniato symptoms is unclear.
• Although most patients with GERD have some degree of hiatus hernia, <50% of patients with hiatus hernia have GERD.
Symptoms and Signs• Most patients with a sliding hiatus
hernia are asymptomatic, But chest pain and other reflux symptoms can occur.
• A paraesophageal hiatus hernia is generally asymptomatic but, unlike a sliding hiatus hernia, may incarcerate and strangulate.
• Occult or massive GI hemorrhage may occur with either type.
Diagnosis and Treatment• A large hiatus hernia is often
discovered incidentally on chest x-ray. Smaller hernias are diagnosed with a barium swallow.
• An asymptomatic sliding hiatus hernia requires no specific therapy. Patients with accompany ing GERD should be treated.
• A paraesophageal hernia should be reduced surgically because of the risk of strangulation.