Embed Size (px)
Citation preview

Dislocation of the First Costovertebral Articulation on One Side and Fracture of First Rib on Another Side

Dislocation of the first costovertebral articulation on one side andfracture of first rib on another side
Pankaj Kumar*
ABSTRACT
Costovertebral dislocation of first rib on one side and first rib fracture on other side is a rare injury. We are elaboratingthe diagnosis and its presentation.
Copyright © 2012, Indraprastha Medical Corporation Ltd. All rights reserved.
Keywords: Costovertebral subluxation, First rib, Fracture
INTRODUCTION
From the time that they were originally described the firstrib fractures have been a source of anxiety to attendingdoctors. First rib fractures are fairly common injuries andare frequently associated with massive trauma to other partsof body including the thorax, head and abdomen. The mostcommon associated injuries pneumothorax, haemothorax,pulmonary contusion, a flail chest and myocardial contu-sion occasionally with a haemopericardium. Local injuriesmore directly related to the first rib fracture include traumaof the brachial plexus injuries, Horner syndrome and tear ofthe subclavian artery. In contrast, bilateral first rib fracturesmay follow less significant thoracic trauma, suggesting thatthe mechanism of injury may be different. We were report-ing one case of costovertebral dislocation of first rib oneside and fracture of another rib on another side. This typeof injuries had not been reported in literature.
CASE REPORT
A 35 year’s old man presented to Apollo Reach Hospitalafter being fall from height. The injuries were confined tothe supraorbital region and thorax. The patient was fullyconscious and normotensive. Abdominal examination wasnormal. Examination of limbs revealed no neurological
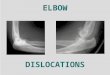
deficits but there was Horner syndrome. The chest radio-graph showed costovertebral dislocation of right rib andfracture of left rib (Figs. 1 and 2). Management entailedanalgesics and close observation of respiratory function.The patient was discharged at 7 days of admission. Onreview a month later he was found to be good health;specifically, there were no upper limb neurovascular deficitor neuropathies.
DISCUSSION
The costovertebral articulations consist of two gliding typesynovial joints, the costocentral and the costotransverse.When subjected to severe trauma, these joints may be sub-luxed or dislocated. The costotransverse joint is more likelyof the two to be injured. The first costotransverse joint isespecially vulnerable because of its unique position at thetop of the rib cage.1 The first rib attaches at the sternum,turns at the base of the cervical spine and inserts at the T1vertebral junction. The brachial plexus is intimately situatedaround the first rib, with the C7 and C8 nerve roots actuallysurrounding the rib on their way to becoming the cords ofthe brachial plexus. The first rib, like any other joint, cansubluxate, usually in a superior and outward position. Withsome practice, a clinician can feel the first rib as it is moresuperiorly displaced in the cervical space. This may be
Apollo Reach Hospital, Karimnagar, India.*North Avenue, Plot No-6, Beside Apollo Reach Hospital, Karimnagar 505001, India. Tel.: þ91 9618123678, email: [email protected]
Received: 19.8.2012; Accepted: 22.9.2012; Available online 29.9.2012Copyright � 2012, Indraprastha Medical Corporation Ltd. All rights reserved.http://dx.doi.org/10.1016/j.apme.2012.09.002
Apollo Medicine 2012 DecemberVolume 9, Number 4; pp. 343e344 Case Report

significant in that many patients with neck pain difficult toresolve may actually have a first-rib subluxation, promotinga restricted cervical movement that is resistant to adjustmentsof the cervical themselves. A proper evaluation of the neuro-logical system is the only way to know which side to addressas primary. But for those just starting out in the fun world ofneurology, knowing about the first rib may very well makeall the difference in those difficult cases no one else hasbeen able to solve.2 Pain and dysaesthesia affecting theneck and upper limb is a common isolated complaint, whichmay be accompanied by paresis and vasomotor and trophicchanges of the arm and hand. The peripheral nervessupplying the upper limb may be vulnerable to entrapment
at a number of points along their course through the cervicalroot canals, the thoracic outlet and the axilla. The majorarteries and veins serving the upper limb are closely relatedto the nerve structures at the thoracic outlet and symptoms ofischaemia and/or venous obstruction may accompany theneurological findings, or present in isolation. A comprehen-sive account of the compressive syndromes of the thoracicoutlet is given in the excellent monograph by Lord andRosati (1971).3 Cervical ribs (Halsted and Reid, 1916)4
have long been recognized as a source of nerve and/orvascular compression; though the association of their pres-ence with signs of neurovascular entrapment is not a simpleone. Cervical ribs (Halsted and Reid, 1916)4 have long beenrecognized as a source of nerve and/or vascular compression,though the association of their presence with signs of neuro-vascular entrapment is not a simple one. Injuries to the firstrib synchondrosis are uncommon in sport. The potential forserious complications following posterior displacement issimilar to that seen with posterior sternoclavicular joint dislo-cation. Conservative treatment is invariably effective witha return to sport in 4e6 weeks.5 Treatment options for dis-placed costochondral injuries are poorly described in theliterature. They include conservative treatment or closedreduction under general anaesthesia. If open reduction andfixation is necessary, the risk of migration of fixation devicesshould be considered.6
CONFLICTS OF INTEREST
The author has none to declare.
REFERENCES
1. Christensen EE, Dietz GW. Injuries of the first costovertebralarticulation. Radiology. 1980 Jan;134(1):41e43.
2. Romero DC, DACNB Edgar. Vascular concomitants secondaryto 1st rib subluxation. Dynamic Chiropractic. June 4, 2007;vol.25(Issue 12).
3. Lord Jr JW, Rosati LM. Thoracic outlet syndrome. Clin Symp.1971;23(2):1e32.
4. Halsted WS, Reid MR. An experimental study of circum-scribed dilatation of an artery immediately distal to a partiallyoccluding band and its bearing on the dilatation of the subcla-vian artery observed in certain diseases of cervical rib. J ExpMed. 1916;24:271e286.
5. Kemp SPT, Targett SGR. Injury to the first rib synchondrosis ina rugby footballer. Br J Sports Med. 1999;33:131e133.
6. Lyons FA, Rockwood Jr CA. Migration of pins used in opera-tions on the shoulder. J Bone Joint Surg Am. 1990;72:1262e1267.
Fig. 1 Inferior subluxation of first rib on right side and fractureof first rib on left side.
Fig. 2 Subluxation of first rib fracture on right side and fractureof first rib on left side.
344 Apollo Medicine 2012 December; Vol. 9, No. 4 Kumar

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/