Embed Size (px)
Citation preview

Direct Hyperbilirubinaemia
Dr. Tareq rahman , Resident Phase B , Neonatology,
Bangabandhu Sheikh Mujib Medical University( BSMMU).

NASPGHAN Definition :
Prolonged conjugated hyperbilirubinemia thatoccurs in the newborn period with conjugatedbilirubin concentration >1 mg/dl if the totalbilirubin <5.0mg/dl or >20% of the totalbilirubin if the total bilirubin >5.0 mg/dl.
(Moyer et al J PEDIATR GASTROENTEROL NUTR 2004;39:115)

IAP Definition:
Neonatal cholestasis is defined as
conjugated hyperbilirubinemia > 1.5-2
mg% in a newborn/ infant with passage of
high coloured urine with or without acholic
stools.
(Consensus report on neonatal cholestasis syndrome,INDIAN PEDIATRICS
2000;37:845-851)

PATHOPHYSIOLOGY



PREVALENCE

• Neonatal cholestasis: 1 in 2500 live birth.
• Biliary atresia: 1 in 10000 to 15000 infants.
• Idiopathic neonatal hepatitis: 1 in 5000 to 10000 live birth.
(McKiernan PJ et al. Lancet 2000)

ETIOLOGY

ETIOLOGY
Intrahepatic causes
Extrahepatic causes

INTRAHEPATIC ETIOLOGIES
Hepatocellular causes Bile duct injury (Neonatal hepatitis)
Idiopathic: INHToxic Intrahepatic bile ductGenetic/Chromosomal hypoplasia or paucityInfectiousMetabolicMiscellaneous

EXTRAHEPATIC ETIOLOGIES
Extrahepatic biliary atresia
Choledochal cyst
Bile duct stenosis
Spontaneous perforation of the bile duct
Cholelithiasis
Inspissated bile/mucus plug
Extrinsic compression of the bile duct

Neonatal Hepatitis
35%
Biliary Atresia
26%
INH24%
Others15%
(Bazlul Karim AS, Kamal M, Cholestatic jaundice during infancy: experience at a tertiary-care center in Bangladesh, Indian J Gastroenterology, 2005 Mar-Apr;24(2):52-4.)

Hepatocellular causes:Neonatal hepatitis
idiopathic TORCHSepsisOthers(UTI)
MetabolicMiscellaneousObstructive causes: Biliary atresia Choledochal cystDuctal paucityIdiopathic
53%47%64%22%08%06%04%02%38%34%04%03%06%
(Consensus report on neonatal cholestasis syndrome,INDIAN PEDIATRICS 2000;37:845-851)

• TPN Related Cholestasis Most common in developed country

Sepsis-induced cholestasis
Gram-negatives predominated (77%)
• Klebsiella species (25%)
• Escherichia coli (15%)
• Staphylococcus aureus (18%)
• Group B streptococci ( 7%)
• Others –
Pseudomonas , Bacteroids , Tuberculosis
• (Ziadi et al.Pathogens associated with sepsis in newborns and young infants in developing
countries. Pediatr Infect Dis J. 2009 Jan;28)

Mechanisms of Hyperbilirubinemia in Sepsis
• Hemolysis
- Increased Bilirubin Load
• Hepatic dysfunction
- Decreased canalicular transport
- Decreased clearance of conjugated bilirubin
- Hepatic ischemia
- Hepatocellular injury
• Cholestasis
- Decreased basolateral transport of bile acids
- Decreased basolateral membrane fluidity
- Inhibition of basolateral membrane Na-K-ATPase activity
- Decreased canalicular transport of bile acids
- Down-regulation of transporters

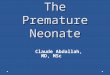
Approach

Evaluation

When to suspect ?

Cardinal Features
– Jaundice
– Dark urine
– Pale stools (+/-)
– Hepatomegaly

HistoryAge at presentation-
within first 3months of life.
Sex- INH is common in male & BA is common in female.
Family history
- Consanguinity- Metabolic disease.
- Same type of illness.
Antenatal Fever TORCH infection.RashAbortion, miscarriage- metabolic diseases.
NatalTerm- BA. Preterm- INH.
Birth weightSGA/LBW- INH.AGA- BA.

Postnatal
Onset of jaundice
Less feeding
Lethargy
Hoarse cry hypothyroidism
Constipation
Delayed passage of meconium
Convulsion- congenital infection
Examination
General examinationAppearance
• Irritable, lethargic- cong infection, metabolic diseases
• Dysmorphic Alagille syndrome.
Down syndrome.
Hypothyroidism,
Large anterior fontanel-• Hypothyroidism, Down syndrome.
Pallor
Jaundice

Skin survey
Rash- sepsis.
Hypothyroidism
Anthropometry
OFC- microcephaly in cong. infection.
Weight, height- FTT in INH, cong infection

Eye examination (slit lamp)
Cataract- galactosemia.
Choreoretinitis- CMV, Rubella, Toxoplasma.
Cherry red spots- Niemen-Pick disease.
Posterior embryotoxon- Alagille syndrome.
Optic Hypoplasia- Panhypopituitarism

Alimentary system
Oral cavity
• cleft lip, cleft palate- BA.
Abdomen
• Pott belly, umbilical hernia- hypothyroidism
• Hepatosplenomegaly- BA, cong infection, galactosemia.
• Right hypochondriac mass- Choledochal cyst.
• Ascites-

Investigations
A. Initial investigations:
To establish cholestasis and determine severity of
liver disease-
Fractionated S. Bilirubin
Liver function test:
ALT, AST, GGT, Alkaline phosphatase
S.albumin, PT

B. To detect conditions that require immediate treatment-
CBC / septic screeningBlood glucoseIndicated cultures of blood & urineSerum T4, TSHTo detect metabolic conditions- Urinalysis,
urine for reducing substanceTORCHS titres

C. To differentiate extrahepatic from intrahepatic causes of cholestasis-
1. Imaging studies-Ultrasonography of Hepatobiliary system-Hepatobiliary scintigraphy
2. Percutaneous liver biopsy (safe and most useful for diagnosis.)
3. Exploratory laparotomy with intraoperative cholangiogram( gold standard for biliary atresia )

E. Establish other diagnosis- S. Alpha-1-antitrypsin level
Sweat chloride (cystic fibrosis)
Urine/serum amino acids (metabolic conditions)
X-ray skull and long bones (cong. infection)
Echo (cong. infection, Alagille syn.)
X-ray chest (cong. infection)
Bone marrow study (Storage disease)

Management

Supportive management
Parental counseling
Nutritional support
Choleretics and bile acid-binders

Specific treatment
1. INH- no specific treatment.
2. BA- Kasai surgery ( Roux-en-Y portoenterostomy )
3. Hypothyroidism- life long thyroxine.
4. Galactosemia- avoid galactose containing diet.
5. Choledochal cyst- excision of the cyst.
6. Congenital infection- according to causative organism.
7. Liver transplantation

Liver transplantation
Decompensated liver disease (ascites and/or encephelopathy)
Biliary atresia is the most common indication for transplant.
Indications-
When initial treatment was given lately/ Portoenterostomy not done.
Failed portoenterostomy.
Decompensated cirrhosis and end stage liver disease despite initial successful Kasai.

Prognosis
Depends on: Etiology and early diagnosis/treatment
Severity of insult
Progression to cirrhosis
Portal hypertension
Liver transplantation
Age at intervention is the most important factor for outcome.

Prognosis
Biliary atresia
50-80% will die without LT by 1 yr, if Kasai not done.
90-100% will die by age 3 yrs
70-80% require LT after Kasai during 1st 2 decade.
80-90% long term survival after LT.
Idiopathic neonatal hepatitis
In sporadic case, 60-70%disease free survival,<5% severe liver disease or cirrhosis.
In familial case, 20-30%recover, 10-15% CLD with cirrhosis, require LT.

Take-Home Message
Any Jaundice>2 weeks requires investigation.
Always do fractionated bilirubin
(Total + Direct bilirubin).
Early diagnosis and management (<2 months old) is critical for the best outcome

Thank you all









![[lbca] tareq al suwaidan](https://img.pdfslide.us/doc/110x75/568ca5db1a28ab186d8ecdd0/lbca-tareq-al-suwaidan.jpg)