Embed Size (px)
DESCRIPTION
Citation preview

Differential Diagnosis of Red Eye

Differential Diagnosis of Red Eye
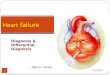
Pain?
Scleritis Acanthamoeba keratitis Herpes Zoster keratitis
Visible skin lesions on same side?
Herpes Zoster keratitis Unilateral
Superficial or deep fl- stain
Associated anterior uveitis
Y
Urgent referral to GP for anti-viral treatment
Scleritis Acanthamoeba keratitis
N
Diffuse or localised deep bluish injection
Immobile on palpation? Scleritis Bilateral/Unilateral
Associated with rheumatoid arthritis and
herpes zoster
Urgent referral to GP for anti-inflammatory treatment. Thinning
may cause perforation
Acanthamoeba keratitis Moderate signs
Severe symptoms C/L wearer
Uses tap water for cleaning or storage
Urgent referral to hospital
eye casualty for treatment. Complete loss
of sight possible in 48 hours
Y N
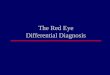
Moderate or Severe Anterior Uveitis
Angle-closure glaucoma
Type of trauma?
N
Moderate or Severe Anterior Uveitis Scleritis
Acanthamoeba keratitis Angle-closure glaucoma
Penetrating trauma Chemical burn Photokeratitis
Herpes Zoster keratitis Orbital Cellulitis
Reduced Visual Acuity? Moderate or Severe Anterior Uveitis
Angle-closure glaucoma Penetrating trauma
Chemical burn
Y Scleritis
Acanthamoeba keratitis Photokeratitis
Herpes Zoster keratitis Orbital Cellulitis
N
History of trauma? Y
N
Moderate or Severe Anterior Uveitis
Penetrating trauma Chemical burn
blunt
Moderate or severe anterior uveitis
Check IOP
sharp
Penetrating trauma
Hyphaema Seidel’s
test
chemical
Chemical burn Irrigate with
water Remove solid
debris
Urgent referral to hospital eye casualty department
UV exposure?
Photokeratitis Bilateral
6-12 hours from exposure superficial punctate fl- stain
No other abnormality
Y
Tx – oral analgesia Ocular lubricant Self-resolving in 24-48 hours
Scleritis Acanthamoeba keratitis Herpes Zoster keratitis
Orbital Cellulitis
N
Raised IOP > 40mmHg?
Moderate or Severe Anterior Uveitis Miotic reactive pupil Deep circumlimbal flush
Angle-closure glaucoma mid-dilated fixed pupil
corneal oedema diffuse circumlimbal flush narrow/closed AC angles
Y
Urgent referral to hospital eye casualty department
Pain on eye movement?
Orbital cellulites Unilateral
Severely swollen lids Proptosis
Urgent referral to hospital eye casualty department as brain can
be affected
Y
See flow-chart 1 continuation sheet
N
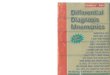
Marginal lid skin lesions?
Small foreign body Herpes Simplex Keratitis Bacterial Conjunctivitis
Dry Eye Episcleritis
H202 solution exposure
Trauma? Y
Small foreign body Unilateral
Fl- staining track Evert upper lid and check
Anaesthetise and lift off
with moist sterile cotton bud if superficial
Urgent referral to hospital eye casualty department
Herpes Simplex Keratitis Bacterial Conjunctivitis
Dry Eye Episcleritis
H202 solution exposure
C/L
wearer?
Bacterial Conjunctivitis Dry Eye
H202 solution exposure
N
Y Herpes Simplex Keratitis Bacterial Conjunctivitis
Dry Eye Episcleritis
Mucopurulent discharge?
N
N
Severe conjunctival injection? H202 solution exposure
Bilateral Diffuse corneal punctate
fl- staining C/L removal
C/L removal Cold compresses Prophylactic anti-
infective if staining is severe
Resolves in 48 hours
Mucopurulent discharge?
Bacterial Conjunctivitis Bilateral
Papillae in palpebral conj Conj injection most at
fornix
Y Y
Refer urgently to GP for Tx due to the potential for
serious infections
Herpes Simplex Keratitis Dry Eye
Episcleritis Herpes Simplex
Keratitis Unilateral
Dendritic ulcer
Y
N
Dry Eye Episcleritis
N
Localised redness beneath
conjunctiva?
N
N Y
Artificial tears Refer to GP for Tx if severe
Episcleritis Unilateral
Pain on palpation
Refer to GP for Tx and systemic diagnosis
Y
Dry Eye H202 solution exposure
Dry Eye Small tear prism
Low TBUT Low tear quality
Punctate fl- staining Diffuse RB staining
Refer urgently to GP for Tx due to the
potential for visual loss
Moderate tosevere ordeep pain
Mild orpricking pain
Follicles
Viral Conjunctivitis Chlamydial Conjunctivitis
Allergic Conjunctivitis C/L solution sensitivity
Canaliculitis Blepharitis
Mild Anterior Uveitis
Discharge? Y
Viral Conjunctivitis Chlamydial Conjunctivitis
Allergic Conjunctivitis
C/L solution sensitivity Canaliculitis Blepharitis
Mild Anterior Uveitis
Lid margin
swollen/red? Canaliculitis Blepharitis
N
Y C/L solution sensitivity Mild Anterior Uveitis
Localised swelling?
N
Y Flare and cells in AC? Mild Anterior
Uveitis Unilateral Check IOP
Reassure patient Cease C/L wear
Refer to C/L practitioner
Y
Canaliculitis Unilateral
Mucopurulent discharge expressable from punctum
Refer to GP if causing irritation or bacterial
conjunctival infections
Blepharitis Bilateral
Self-limiting
Reassure and advise on use of lid scrubs
N
Refer to GP for Tx and investigation
N
C/L solution sensitivity Bilateral
Uses a preserved C/L cleaning or soaking
solution
Discharge?
Viral Conjunctivitis Allergic Conjunctivitis
Chlamydial Conjunctivitis Allergic Conjunctivitis
Watery Mucous
Upper lid eversion
Viral Conjunctivitis Bilateral
Preauricular node tenderness
Superficial punctate fl- staining
Highly contagious
Counsel and clean
Refer to GP for sick note
Papillae Conjunctival
chemosis N
Cold compresses Refer to GP for Tx
Y Allergic Conjunctivitis Bilateral
Superficial punctate fl- stain
Chlamydial Conjunctivitis Bilateral
Young adult Follicles and papillae
Corneal infiltrates Superior Pannus
History of new sexual partner
Refer to GP for Tx and further investigation
Itching or discomfort
Subconjunctival haemorrhage Chronic Anterior Uveitis
Pinguecula Pterygium
Sectoral redness?
Y Subconjunctival haemorrhage
Pinguecula Pterygium
Chronic Anterior Uveitis Bilateral
Associated systemic condition Low level AC flare and cells
Check IOP
Triangular with apex at cornea
Solid red beneath
conjunctiva Subconjunctival
haemorrhage Unilateral
Resolves in 7-10 days
Pinguecula Pterygium
Y N
Counsel patient Refer to GP if recurrent
Shape and colour of lesion
Round or oval, white/yellow
Refer to GP for Tx with artifical tears if staining
extends to cornea
Pinguecula Bilateral
Asymmetrical May cause local fl- stain
Pterygium Bilateral
Asymmetrical Present in individuals
exposed to sun and dry, dusty environments May cause local fl-
staining
Refer to hospital via GP for Tx if lesion extends
to pupil margin or VA is reduced
N
Refer to GP for diagnosis and Tx if not previously detected
No pain or discomfort

Moderate to severe or deep pain
Moderate or Severe Anterior Uveitis Scleritis
Acanthamoeba keratitis Angle-closure glaucoma
Penetrating trauma Chemical burn Photokeratitis
Herpes Zoster keratitis Orbital Cellulitis
Reduced Visual Acuity? Y
N

Moderate to severe or deep pain, reduced VA
N
Moderate or Severe Anterior Uveitis Angle-closure glaucoma
Penetrating trauma Chemical burn
Y
History of trauma? Y

Moderate to severe or deep pain, reduced VA, history of trauma
Type of trauma?
Y Moderate or Severe Anterior Uveitis
Penetrating trauma Chemical burn
blunt sharp chemical

Moderate to severe or deep pain, reduced VA, history of blunt trauma
blunt
Moderate or severe anterior uveitis
Check IOP
Urgent referral to hospital eye casualty department

Moderate to severe or deep pain, reduced VA, history of sharp trauma
sharp
Penetrating trauma
Hyphaema Seidel’s
test
chemical
Urgent referral to hospital eye casualty department

Moderate to severe or deep pain, reduced VA, history of chemical trauma
chemical
Chemical burn Irrigate with
water Remove solid
debris
Urgent referral to hospital eye casualty department

Moderate to severe or deep pain, reduced VA, no history of trauma
Moderate or Severe Anterior Uveitis
Angle-closure glaucoma
N
History of trauma?
Chemical burn Irrigate with
water Remove solid
debris
Raised IOP > 40mmHg?
Y

Moderate to severe or deep pain, reduced VA, no history of trauma, IOP > 40mmHg
Angle-closure glaucoma mid-dilated fixed pupil
corneal oedema diffuse circumlimbal flush narrow/closed AC angles
Y
Urgent referral to hospital eye casualty department

Moderate to severe or deep pain, VA unaffected
Scleritis Acanthamoeba keratitis
Photokeratitis Herpes Zoster keratitis
Orbital Cellulitis
N
UV exposure? Y

Moderate to severe or deep pain, VA unaffected, history of UV exposure
N
Photokeratitis Bilateral
6-12 hours from exposure superficial punctate fl- stain
No other abnormality
Y
Tx – oral analgesia Ocular lubricant Self-resolving in 24-48 hours

Moderate to severe or deep pain, VA unaffected, no history of UV exposure
Scleritis Acanthamoeba keratitis Herpes Zoster keratitis
Orbital Cellulitis
N
Pain on eye movement?
Y
N

Moderate to severe or deep pain, VA unaffected, no history of UV exposure, pain on eye movement
Orbital cellulites Unilateral
Severely swollen lids Proptosis
Urgent referral to hospital eye casualty department as brain can
be affected
Y

Moderate to severe or deep pain, VA unaffected, no history of UV exposure, no pain on eye movement
Scleritis Acanthamoeba keratitis Herpes Zoster keratitis
Visible skin lesions on same side?

Moderate to severe or deep pain, VA unaffected, no history of UV exposure, no pain on eye movement,
visible skin lesions on same side
Herpes Zoster keratitis Unilateral
Superficial or deep fl- stain
Associated anterior uveitis
Y
Urgent referral to GP for anti-viral treatment

Moderate to severe or deep pain, VA unaffected, no history of UV exposure, no pain on eye movement, no
visible skin lesions on same side
Scleritis Acanthamoeba keratitis
N
Diffuse or localised deep bluish injection
Immobile on palpation?

Moderate to severe or deep pain, VA unaffected, no history of UV exposure, no pain on eye movement, no visible skin lesions on same side, deep bluish injection
Scleritis Bilateral/Unilateral
Associated with rheumatoid arthritis and
herpes zoster
Urgent referral to GP for anti-inflammatory treatment. Thinning
may cause perforation
Y

Moderate to severe or deep pain, VA unaffected, no history of UV exposure, no pain on eye movement, no
visible skin lesions on same side, no deep bluish injection
Acanthamoeba keratitis Moderate signs
Severe symptoms C/L wearer
Uses tap water for cleaning or storage
Urgent referral to hospital
eye casualty for treatment. Complete loss
of sight possible in 48 hours
N

Mild or pricking pain
Small foreign body Herpes Simplex Keratitis Bacterial Conjunctivitis
Dry Eye Episcleritis
H202 solution exposure
Trauma? Y Herpes Simplex Keratitis Bacterial Conjunctivitis
Dry Eye Episcleritis
H202 solution exposure
N

Mild or pricking pain, history of trauma
Small foreign body Unilateral
Fl- staining track Evert upper lid and check
Anaesthetise and lift off
with moist sterile cotton bud if superficial
Urgent referral to hospital eye casualty department

Mild or pricking pain, no history of trauma
Herpes Simplex Keratitis Bacterial Conjunctivitis
Dry Eye Episcleritis
H202 solution exposure
C/L
wearer?
Y N

Mild or pricking pain, no history of trauma, C/L wearer
Bacterial Conjunctivitis Dry Eye
H202 solution exposure
Mucopurulent discharge?

Mild or pricking pain, no history of trauma, C/L wearer, mucopurulent discharge
Bacterial Conjunctivitis Bilateral
Papillae in palpebral conj Conj injection most at
fornix
Y Y
Refer urgently to GP for Tx due to the potential for
serious infections

Mild or pricking pain, no history of trauma, C/L wearer, no mucopurulent discharge
N
Severe conjunctival injection?
Y
Dry Eye H202 solution exposure

Mild or pricking pain, no history of trauma, C/L wearer, no mucopurulent discharge, severe
conjunctival injection
H202 solution exposure Bilateral
Diffuse corneal punctate fl- staining
C/L removal
C/L removal Cold compresses Prophylactic anti-
infective if staining is severe
Resolves in 48 hours

Mild or pricking pain, no history of trauma, C/L wearer, no mucopurulent discharge, mild
conjunctival injection
Artificial tears Refer to GP for Tx if severe
Dry Eye Small tear prism
Low TBUT Low tear quality
Punctate fl- staining Diffuse RB staining

Mild or pricking pain, no history of trauma, not a C/L wearer
Herpes Simplex Keratitis Bacterial Conjunctivitis
Dry Eye Episcleritis
N
Mucopurulent discharge?
Y

Mild or pricking pain, no history of trauma, not a C/L wearer, no mucopurulent discharge
Marginal lid skin lesions?
Herpes Simplex Keratitis Dry Eye
Episcleritis
N
N

Mild or pricking pain, no history of trauma, not a C/L wearer, no mucopurulent discharge, lid
margin skin lesions
Herpes Simplex Keratitis
Unilateral Dendritic ulcer
Y
Refer urgently to GP for Tx due to the
potential for visual loss

Mild or pricking pain, no history of trauma, not a C/L wearer, no mucopurulent discharge, no lid
margin skin lesions
Dry Eye Episcleritis
N
Localised redness beneath
conjunctiva?
N
Y

Mild or pricking pain, no history of trauma, not a C/L wearer, no m/p discharge, no lid margin skin
lesions, localised sub-conjunctival redness
Episcleritis Unilateral
Pain on palpation
Refer to GP for Tx and systemic diagnosis
Y

Itching or discomfort
Viral Conjunctivitis Chlamydial Conjunctivitis
Allergic Conjunctivitis C/L solution sensitivity
Canaliculitis Blepharitis
Mild Anterior Uveitis
Discharge? Y C/L solution sensitivity
Canaliculitis Blepharitis
Mild Anterior Uveitis
N

Itching or discomfort, discharge present
Viral Conjunctivitis Chlamydial Conjunctivitis
Allergic Conjunctivitis
Discharge? Watery Mucous

Itching or discomfort, watery discharge present
Follicles
Discharge?
Viral Conjunctivitis Allergic Conjunctivitis
Watery
Upper lid eversion
Papillae

Itching or discomfort, watery discharge present, follicles present
Follicles
Viral Conjunctivitis Bilateral
Preauricular node tenderness
Superficial punctate fl- staining
Highly contagious
Counsel and clean
Refer to GP for sick note

Itching or discomfort, watery discharge present, papillae present
Cold compresses Refer to GP for Tx
Allergic Conjunctivitis Bilateral
Superficial punctate fl- stain

Itching or discomfort, mucous discharge present
Chlamydial Conjunctivitis Allergic Conjunctivitis
Mucous
Conjunctival chemosis
N
Y Allergic Conjunctivitis Bilateral
Superficial punctate fl- stain

Itching or discomfort, mucous discharge present, conjunctival chemosis
Cold compresses Refer to GP for Tx
Chlamydial Conjunctivitis Bilateral
Young adult Follicles and papillae
Corneal infiltrates Superior Pannus
History of new sexual partner
Refer to GP for Tx and further investigation

Itching or discomfort, no discharge present
C/L solution sensitivity Canaliculitis Blepharitis
Mild Anterior Uveitis
Lid margin
swollen/red?
N
Y

Itching or discomfort, no discharge present, lid margin swollen and red
Canaliculitis Blepharitis
Y
Localised swelling?
Y Blepharitis Bilateral
Self-limiting
N

Itching or discomfort, no discharge present, lid margin locally swollen and red
Canaliculitis Unilateral
Mucopurulent discharge expressable from punctum
Refer to GP if causing irritation or bacterial
conjunctival infections Chlamydial Conjunctivitis Bilateral
Young adult Follicles and papillae
Corneal infiltrates Superior Pannus
History of new sexual partner

Itching or discomfort, no discharge present, lid margin generally swollen and red
Blepharitis Bilateral
Self-limiting
Reassure and advise on use of lid scrubs

Itching or discomfort, no discharge present, no lid swelling
C/L solution sensitivity Mild Anterior Uveitis
N
Flare and cells in AC?
Y N

Itching or discomfort, no discharge present, no lid swelling, no AC flare/cells
Reassure patient Cease C/L wear
Refer to C/L practitioner
C/L solution sensitivity Bilateral
Uses a preserved C/L cleaning or soaking
solution

No pain or discomfort
Subconjunctival haemorrhage Chronic Anterior Uveitis
Pinguecula Pterygium
Sectoral redness?
Y
Chronic Anterior Uveitis Bilateral
Associated systemic condition Low level AC flare and cells
Check IOP
N

No pain or discomfort, sectoral redness
Subconjunctival haemorrhage Pinguecula Pterygium
Solid red beneath
conjunctiva
Y

No pain or discomfort, sectoral redness, solid red beneath conjunctiva
Subconjunctival haemorrhage
Unilateral Resolves in 7-10 days
Counsel patient Refer to GP if recurrent

No pain or discomfort, sectoral redness, broken red
Triangular with apex at cornea
Solid red beneath
conjunctiva Pinguecula Pterygium
N
Shape and colour of lesion
Round or oval, white/yellow
Pinguecula Bilateral
Asymmetrical May cause local fl- stain
Pterygium Bilateral
Asymmetrical Present in individuals
exposed to sun and dry, dusty environments May cause local fl-
staining

No pain or discomfort, sectoral redness, broken red, round or oval yellow/white lesion
Round or oval, white/yellow
Refer to GP for Tx with artifical tears if staining
extends to cornea
Pinguecula Bilateral
Asymmetrical May cause local fl- stain

No pain or discomfort, sectoral redness, broken red, triangular lesion with apex at cornea
Triangular with apex at cornea
Pterygium Bilateral
Asymmetrical Present in individuals
exposed to sun and dry, dusty environments May cause local fl-
staining
Refer to hospital via GP for Tx if lesion extends
to pupil margin or VA is reduced

No pain or discomfort, general redness
Chronic Anterior Uveitis Bilateral
Associated systemic condition Low level AC flare and cells
Check IOP
N
Refer to GP for diagnosis and Tx if not previously detected

Differential Diagnosis of Red Eye - Clinical Pearls
• Remember the importance of pain and acuity loss– The only red-eye condition with moderate to severe pain
that does not necessarily require referral to a hospital eye casualty is photokeratitis
• Remember pupil reflexes and size are a good clue to distinguish between severe iritis and ACG when the eye is too painful for IOP assessment
• Never use anaesthetic to relieve ocular pain, unless it is to allow irrigation (which you are finding otherwise impossible) in the case of chemical trauma

Differential Diagnosis of Red Eye - Clinical Pearls
• Viral conjunctivitis is extremely contagious. After the examination wash you hands and swab all the consulting room equipment that has been in contact with the patient
• Remember that it is possible for two or more red-eye conditions to co-exist
• If in doubt refer your patient to ophthalmological care