Embed Size (px)
Citation preview

Imaging department Imaging department
reportreport Dr Vu Thi DinhDr Vu Thi Dinh

Nguyen Hong Linh , F, 19 Nguyen Hong Linh , F, 19 months, A16 months, A16
Dx: Dx: Sus Sus LungLung abscesabsces





DiagnosisDiagnosis
Hiatal herniaHiatal hernia

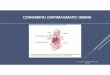
Diaphragmatic herniaDiaphragmatic hernia

Diaphragmatic herniaDiaphragmatic hernia
Congenital: Congenital: two main types:two main types:Bochdalek hernia : most common (75-90%), located : most common (75-90%), located
posteriorly, presents earlierposteriorly, presents earlier Morgagni hernia : smaller, anterior and presents : smaller, anterior and presents
later later Congenital hiatus hernias may also occur, but are Congenital hiatus hernias may also occur, but are
uncommon and distinct.uncommon and distinct.
AcquiredAcquiredTraumatic Traumatic diaphragmatic rupture Hiatus herniaIatrogenic

DiagnosisDiagnosis
UltrasoundUltrasound Chest radiographChest radiograph Esophagogastroduodenal seriesEsophagogastroduodenal series EndoscopyEndoscopy CTCT MRIMRI

UltrasoundUltrasound
Sonographic findings include:Sonographic findings include: cardiomediastinal shift + / - abnormal cardiac cardiomediastinal shift + / - abnormal cardiac
axis axis the stomach being at same transverse level as the stomach being at same transverse level as
the heart : this makes left sided hernias the heart : this makes left sided hernias comparatively easier to detect on ultrasound comparatively easier to detect on ultrasound (as opposed to herniaion of echogenic liver on (as opposed to herniaion of echogenic liver on the right side) the right side)
portal veins in thorax (Doppler) portal veins in thorax (Doppler) absent bowel loops in the abdomen absent bowel loops in the abdomen there may be there may be polyhydramnios as an ancilliary as an ancilliary
sonographic feature sonographic feature

US of chest-there are multiple fluid-filled loops of the bowel within the left hemithorax

Chest radiograph Chest radiograph
indistinct diaphragm with indistinct diaphragm with opacification of part of or all the opacification of part of or all the hemithorax (typically left sided) hemithorax (typically left sided)
scaphoid abdomen scaphoid abdomen deviation of lines: endotracheal tube, deviation of lines: endotracheal tube,
nasogastic tube, umbilical arterial nasogastic tube, umbilical arterial and venous catheters and venous catheters

“scaphoid abdomen “

Bochdalek hernia
Most common Most common Left > rightLeft > right Hernia may contain intestine, Hernia may contain intestine,
stomach, spleen, liver or omentumstomach, spleen, liver or omentum Hypoplasia of ipsilateral lung occurs Hypoplasia of ipsilateral lung occurs
from mass effect of bowel from mass effect of bowel

Bochdalek hernia
4-day-old infant


A 2-year-old girl who presented with intermittent abdominal pain and mild shortness of breath caused by a small Bochdalek hernia

Morgagni hernia Herniation through the Herniation through the foramen of Morgagni
which is located immediately adjactent to the which is located immediately adjactent to the xiphod process. The majority of hernias xiphod process. The majority of hernias occur on the right side and are generally occur on the right side and are generally asymptomatic.asymptomatic.
As compared to the Bochdalek hernia, the As compared to the Bochdalek hernia, the Morgagni hernia is:Morgagni hernia is:
-Rare -Rare - Small - Small
-Anterior , -Anterior , Right > left (heart protects) Right > left (heart protects) -At low risk of prolapse -At low risk of prolapse

A 2-week-old boy with Morgagni defect

A 7-day-old boy with aMorgagni hernia.

Hiatus hernia
A A hiatus herniahiatus hernia occurs where there occurs where there is herniation of stomach through the is herniation of stomach through the oesophageal hiatus of the diaphragm oesophageal hiatus of the diaphragm
Sub types:Sub types:
- Sliding hiatus hernia (95%)- Sliding hiatus hernia (95%)
- Rolling (para-oesophageal) hiatus - Rolling (para-oesophageal) hiatus hernia (5%)hernia (5%)


Sliding hiatus herniaSliding hiatus hernia
The gastro-oesophageal junction (GOJ) is The gastro-oesophageal junction (GOJ) is usually displaced by more than 1cm usually displaced by more than 1cm above the hiatus. The oesophageal hiatus above the hiatus. The oesophageal hiatus is often abnormally widened to 3 - 4cm : is often abnormally widened to 3 - 4cm : the upper limit is 15mm. the upper limit is 15mm.
The gastric fundus may also be displaced The gastric fundus may also be displaced above the diaphragm and present as a above the diaphragm and present as a retrocardiac mass on a chest radiograph. retrocardiac mass on a chest radiograph. The presence of an air-fluid level in the The presence of an air-fluid level in the mass suggests the diagnosis. mass suggests the diagnosis.


Sliding hiatus hernia: (a)Infant, vestibule closed. (b) Infant, vestibule open. (c) ,Adult, vestibule open, inferior esophageal sphincter contracted. The latter produces a rounded ring at the proximal end of the vestibule on an esophagogram.

Those patients with a congenital hiatal hernia demonstrated one on more of the following signs:
(1) an abnormally high position of the inferior esophageal sphincter;
(2) a beak formation at the gastric candia; (3) linear orientation of gastric folds toward the
esophagus at the candia (irregularity of the cardia);
(4) visualization of gastric folds above the diaphragm;
(5) a funnel formation at the cardia; (6) an air- filled hole at the cardia; (7) an epiphrenic loculus; (8) a distal esophageal web; (9) the presence of delayed gastroesophageal
reflux.

A: normal childB: 3 month infant with hiatal hernia

The “beak” sign- 2 month infant

4 month old male infant: Re-fluoroscopy with manual compression of the stomach

Gastric folds above the diaphragm of 10 month old male infant

“Funnel” sign

The “hole” sign

The “epiphrenic loculus

Delayed GER- 30 minute

a distal esophageal web




Radiograph of a patient with a small axial hiatal hernia

a. The vestibule has completely closedb. The vestibule has opened (16 day old infant)





DiscussionDiscussion
The roentgenologic diagnosis of hiatal herniae in the young is difficult because:
Many roentgen landmarks seen in adults cannot be demonstrated in infants
The involved structures are small Events occur so rapidly that the
roentgenologist may experience difficulty in recording the findings at the optimum moment, if he uses conventional filming techniques

DiscussionDiscussion
The smallest herniae cause significant The smallest herniae cause significant symptoms and complications, symptoms and complications, distressing reflux symptoms.distressing reflux symptoms.
The failure to diagnose hiatal herniae The failure to diagnose hiatal herniae in children, moreover, can have in children, moreover, can have serious consequences. serious consequences.
The presence of hiatal hernia in infants The presence of hiatal hernia in infants should always be considered when the should always be considered when the appropriate clinical symptoms appear.appropriate clinical symptoms appear.

Rolling (para-oesophageal) Rolling (para-oesophageal) hiatus herniahiatus hernia
The GOJ remains in its normal The GOJ remains in its normal location while a portion of the location while a portion of the stomach herniates above the stomach herniates above the diaphragm diaphragm


A 4-month-old girl with a paraesophageal hernia who presented with vomiting.
Rolling (para-oesophageal) Rolling (para-oesophageal) hiatus herniahiatus hernia

Differential diagnosisDifferential diagnosis
congenital cystic adenomatoid congenital cystic adenomatoid malformation (CCAM) malformation (CCAM)
retrocardiac lung abscess retrocardiac lung abscess retrocardiac empyema retrocardiac empyema Pulmonary sequestration Pulmonary sequestration epiphrenic oesophageal diverticulum epiphrenic oesophageal diverticulum

Congenital Cystic Adenomatoid Malformation (CCAM)

Congenital Cystic Adenomatoid Malformation (CCAM)

ndications for this additional studyare: (i) appropriate clinical history (vom-iting, dysphagia, failure to gain weight,gastrointestinal bleeding, anemia, repeatedpulmonary infections); on (2) observationof an abnormality of the candioesophagea

Indications for this additional study are: (i) appropriate clinical history
(vomiting, dysphagia, failure to gain weight, gastrointestinal bleeding, anemia, repeated pulmonary infections);
(2) observation of an abnormality of the candioesophageal junction during a routine fluoroscopy

The hiatal hernia-reflux examination The hiatal hernia-reflux examination immediately follows completion of a routine immediately follows completion of a routine upper gastrointestinal series fluoroscopy and upper gastrointestinal series fluoroscopy and begins with the patient supine on slightly begins with the patient supine on slightly Tnendelenburg in position. Tnendelenburg in position.
A spoonful of barium is then given and the A spoonful of barium is then given and the movement of contrast through the esophagus is movement of contrast through the esophagus is fluoroscopically observed-especially noting the fluoroscopically observed-especially noting the inferior esophageal sphincter and its level inferior esophageal sphincter and its level relative to the diaphragmrelative to the diaphragm
When satisfactony mucosal coating is seen, When satisfactony mucosal coating is seen, multiple spot film noentgenograms of the multiple spot film noentgenograms of the cardioesophageal region are taken in the cardioesophageal region are taken in the antenopostenior and slight right and left antenopostenior and slight right and left anterior oblique projections. anterior oblique projections.

A second spoonful of thickened barium A second spoonful of thickened barium is given, the child is immediately turned is given, the child is immediately turned into the horiontal prone position, and into the horiontal prone position, and multiple spot film roentgenograms are multiple spot film roentgenograms are taken in the posteroanterior and slight taken in the posteroanterior and slight right and left oblique position. right and left oblique position.
These supine and prone spot film These supine and prone spot film roentgenognams are mucosal views roentgenognams are mucosal views designed to show (I) the junction designed to show (I) the junction between the esophageal and gastric between the esophageal and gastric folds and (2) the location of this folds and (2) the location of this junction relative to the diaphragm.junction relative to the diaphragm.

Allowing the infant to nurse on a sugar Allowing the infant to nurse on a sugar nipple on having the older child undergo nipple on having the older child undergo “dry swallows” often assists in obtaining “dry swallows” often assists in obtaining optimal mucosal detail.optimal mucosal detail.
The patient is then turned back into a The patient is then turned back into a horizontal supine position and evidence horizontal supine position and evidence of spontaneous gastroesophageal reflux of spontaneous gastroesophageal reflux or relux secondary to increased intra-or relux secondary to increased intra-abdominal pressure (using manual abdominal pressure (using manual pressure on the stomach) is noted to be pressure on the stomach) is noted to be present or absent.present or absent.

After the initial fluoroscopy and standard After the initial fluoroscopy and standard overtable roentgenograms are taken, the overtable roentgenograms are taken, the child is held in the erect (preferably), child is held in the erect (preferably), prone on right lateral decubitus (right prone on right lateral decubitus (right side down position for at least 30 side down position for at least 30 minutes. At this time a supine minutes. At this time a supine roentgenogram of the abdomen (including roentgenogram of the abdomen (including the distal thoracic esophagus) is obtained the distal thoracic esophagus) is obtained and the patient is placed again into the and the patient is placed again into the erect, prone or night lateral position. erect, prone or night lateral position.

If contrast material is seen in the If contrast material is seen in the esophagus on this noentgenogram in an esophagus on this noentgenogram in an initially negative study, the child should be initially negative study, the child should be held erect until he or she can be held erect until he or she can be refluoroscoped. Often reflux can be seen refluoroscoped. Often reflux can be seen immediately after the patient is replaced immediately after the patient is replaced into the supine position for fluonoscopy. It into the supine position for fluonoscopy. It is frequently possible to demonstrate a is frequently possible to demonstrate a hiatal hernia at this point (with on without hiatal hernia at this point (with on without another swallow of thickened barium) even another swallow of thickened barium) even though the initial fluonoscopy was though the initial fluonoscopy was negativenegative