Embed Size (px)
DESCRIPTION
International SYMPOSIUM on OROFACIAL MYOFUNCTIONAL Therapy roma 6,7,8 giugno 2014
Citation preview

INTERDISCIPLINARY DETECTION OF OROFACIAL DISFUNCTIONS
IN CHILDREN AND ADOLESCENTS Grandi, Diana (MS, SLP); Bo3ni, Elsa (Orthodon:st) & Lapitz, Lyda (SLP) -‐ Barcelona, SPAIN.
Introduction The Interdisciplinary Orofacial Examination Protocol for Children and Adolescents, authored by a group of professionals consisting of ENTs, Orthodontists, and SLPs (Bottini E., Carrasco A., Coromina J., Donato G., Echarri P., Grandi D., Lapytz L. & Vila E. , Barcelona, 2008) is an efficient and easy to use resource that facilitates the interdisciplinary detection of alterations in the Stomatognatic System.
Normal. Class I Convex. Class II Concave. Class III
Yes No
INTERDISCIPLINARY OROFACIAL EXAMINATION PROTOCOL FOR CHILDREN AND ADOLESCENTS(For ENT, Pediatricians, Dentists and Speech Therapists)
Concept:
Extra and intra-oral interdisciplinary orofacial exploration, which includes the examination to detect possible morphological alterations and/or dysfunctions.
1.Speed (5-8 minutes)2.Simplicity
This suggestion is an approximation to the exploration protocol which entails 2 characteristics:
Parents Anamnesis:
1- Does your child usually snore while sleeping?2- Have you noticed that your child has difficulties in breathing or he/she breathes with lots of effort?3- Have you noticed in your child while sleeping:
Break or pause in breathing?Restless or agitated sleep?Abnormal head postures (hyperextension, etc)?Excessive sweating?
4- Does he/she wet the bed with saliva?5- Does he get easily tired after running or doing exercises?6- Does your child keep his/her mouth open while watching TV or using the computer?7- Does he/she drool during the day?8- Does he frequently catch a cold?9- Is he/she allergic?10- Habits: pacifier/ thumb sucking / nail-biting/ cheilophagia / other11- Does he/she frequently get voiceless?12- Does he/she have pronunciation problems?
Don’t know
Breathing:
Nasal Buccal Mixed
Profile:
Patient personal data:
Name:...................................................................................Age:...................Date:......................................................
Sex:..............Weight:..............Height:................Record:.................................................................................................
By:..................................................................................................................Specialty:................................................
Nostrils configuration (with forced breathing)
Level 0 Level 1 Level 2 Level 3A Level 3B Level 4 Level 5 Both dilate Doesn’t collapse
nor dilateUnilateral partial closure
Bilateral partialclosure
Unilateral totalclosure
Total closure and partial closure
Bilateral totalclosure
1
2
3
4
Authors: Elsa Bottini, Alberto Carrasco, Jordi Coromina, Graciela Donato, Pablo Echarri, Diana Grandi, Lyda Lapitz & Emma Vila.
Malocclusion (Angle)
Class I (Normal) Class II/1 Class II/2 Class III
Lips
Lip contact in rest
Tonsils
Level 0 Level 1 Level 2 Level 3 Level 4 Level 5
Inferior lingual frenum (Ask patient to lift his/her tongue with the completely open mouth, and to try to touch his/her palate)
Previous tonsillectomy
Very small tonsils (< 25%)
No visible tonsils Tonsils occupy 1/3 of pharyngeal space (25% - 50%)
Tonsils occupy 2/3 of pharyngeal space (50% - 75%)
Tonsils occupy 3/3 of pharyngeal space (>75%)
6
7
8
Dry or chapped lipsNo lip contact in rest
Bite Occlusion
Anterior deep bite
Alignment
Normal Spacing Crowding
Swallowing
Tongue thrust or lip thrust while swallowing
Posture alterations
Normal position Lordosis CyphosisLumbar curvatureincreased
Curved back, reduced lumbar curvature shoulders dropped, flat thorax and prominent abdomen
9
10
11
12
Recommended assessment by:
ENT Orthodontist Speech therapist Odontopediatrician14
Open bite Crossbite (uni./bilat.)Normal bite
Normal Makes faces while swallowing
Level 0 Level 1 Level 2 Level 3 Level 4 Level 5Frenectomy Tongue tip
touches the palateAlmost touchesthe palate
The distance between the upper and lower incisors is the same
Reacheslower incisors
Doesn’t reach lower incisors
5
13 Adenoids:
Phonetical test(morning)
Positive (different)
Negative (same)
Endoscopy (only ENT)No obstruction
Partial obstructionProfile X-ray (only orthodontists) Severe obstruction
In this poster, we explain the results of a descriptive study involving a Sample Group (SG) population of 185 subjects and a Control Group (CG) of 187 children, all between the ages of 4 and 16 years, which was conducted in Catalonia (Spain) and which used this protocol.
Objectives • Contribute to the area of OM with efficient resources for the early detection of possible
alterations and dysfunctions. • Diffuse the use of the Interdisciplinary Orofacial Examination Protocol for Children and
Adolescents amongst the various professionals who work with the Stomatognatic System • Unify evaluation criteria of the anomalies between the different disciplines to favour inter-
professional understanding and the use of a common terminology • Relate alterations in respiration and swallowing, dental malocclusion, and posture in
accordance with different age groups and compare the presence of said alterations between SG and CG, and analyse the results.
Methodology The Sample Group consisted of young patients between 4 and 16 years who solicited aid from an ENT, an orthodontist, or an SLP. The Control Group consisted of ordinary primary school students the same ages as the Sample Group who had not sought help from any of the afore mentioned professionals. The protocol was used with the SG and the CG. The data was grouped into 3 age subgroups: 4 to 7 years, 8 to 11 years, and 12 to 16 years.
Normal. Class I Convex. Class II Concave. Class III
Yes No
INTERDISCIPLINARY OROFACIAL EXAMINATION PROTOCOL FOR CHILDREN AND ADOLESCENTS(For ENT, Pediatricians, Dentists and Speech Therapists)
Concept:
Extra and intra-oral interdisciplinary orofacial exploration, which includes the examination to detect possible morphological alterations and/or dysfunctions.
1.Speed (5-8 minutes)2.Simplicity
This suggestion is an approximation to the exploration protocol which entails 2 characteristics:
Parents Anamnesis:
1- Does your child usually snore while sleeping?2- Have you noticed that your child has difficulties in breathing or he/she breathes with lots of effort?3- Have you noticed in your child while sleeping:
Break or pause in breathing?Restless or agitated sleep?Abnormal head postures (hyperextension, etc)?Excessive sweating?
4- Does he/she wet the bed with saliva?5- Does he get easily tired after running or doing exercises?6- Does your child keep his/her mouth open while watching TV or using the computer?7- Does he/she drool during the day?8- Does he frequently catch a cold?9- Is he/she allergic?10- Habits: pacifier/ thumb sucking / nail-biting/ cheilophagia / other11- Does he/she frequently get voiceless?12- Does he/she have pronunciation problems?
Don’t know
Breathing:
Nasal Buccal Mixed
Profile:
Patient personal data:
Name:...................................................................................Age:...................Date:......................................................
Sex:..............Weight:..............Height:................Record:.................................................................................................
By:..................................................................................................................Specialty:................................................
Nostrils configuration (with forced breathing)
Level 0 Level 1 Level 2 Level 3A Level 3B Level 4 Level 5 Both dilate Doesn’t collapse
nor dilateUnilateral partial closure
Bilateral partialclosure
Unilateral totalclosure
Total closure and partial closure
Bilateral totalclosure
1
2
3
4
Authors: Elsa Bottini, Alberto Carrasco, Jordi Coromina, Graciela Donato, Pablo Echarri, Diana Grandi, Lyda Lapitz & Emma Vila.
Malocclusion (Angle)
Class I (Normal) Class II/1 Class II/2 Class III
Lips
Lip contact in rest
Tonsils
Level 0 Level 1 Level 2 Level 3 Level 4 Level 5
Inferior lingual frenum (Ask patient to lift his/her tongue with the completely open mouth, and to try to touch his/her palate)
Previous tonsillectomy
Very small tonsils (< 25%)
No visible tonsils Tonsils occupy 1/3 of pharyngeal space (25% - 50%)
Tonsils occupy 2/3 of pharyngeal space (50% - 75%)
Tonsils occupy 3/3 of pharyngeal space (>75%)
6
7
8
Dry or chapped lipsNo lip contact in rest
Bite Occlusion
Anterior deep bite
Alignment
Normal Spacing Crowding
Swallowing
Tongue thrust or lip thrust while swallowing
Posture alterations
Normal position Lordosis CyphosisLumbar curvatureincreased
Curved back, reduced lumbar curvature shoulders dropped, flat thorax and prominent abdomen
9
10
11
12
Recommended assessment by:
ENT Orthodontist Speech therapist Odontopediatrician14
Open bite Crossbite (uni./bilat.)Normal bite
Normal Makes faces while swallowing
Level 0 Level 1 Level 2 Level 3 Level 4 Level 5Frenectomy Tongue tip
touches the palateAlmost touchesthe palate
The distance between the upper and lower incisors is the same
Reacheslower incisors
Doesn’t reach lower incisors
5
13 Adenoids:
Phonetical test(morning)
Positive (different)
Negative (same)
Endoscopy (only ENT)No obstruction
Partial obstructionProfile X-ray (only orthodontists) Severe obstruction
Malocclusion (Angle)
Class I (Normal) Class II/1 Class II/2 Class III
Lips
Lip contact in rest
Tonsils
Level 0 Level 1 Level 2 Level 3 Level 4 Level 5
Inferior lingual frenum (Ask patient to lift his/her tongue with the completely open mouth, and to try to touch his/her palate)
Previous tonsillectomy
Very small tonsils (< 25%)
No visible tonsils Tonsils occupy 1/3 of pharyngeal space (25% - 50%)
Tonsils occupy 2/3 of pharyngeal space (50% - 75%)
Tonsils occupy 3/3 of pharyngeal space (>75%)
6
7
8
Dry or chapped lipsNo lip contact in rest
Bite Occlusion
Anterior deep bite
Alignment
Normal Spacing Crowding
Swallowing
Tongue thrust or lip thrust while swallowing
Posture alterations
Normal position Lordosis CyphosisLumbar curvatureincreased
Curved back, reduced lumbar curvature shoulders dropped, flat thorax and prominent abdomen
9
10
11
12
Recommended assessment by:
ENT Orthodontist Speech therapist Odontopediatrician14
Open bite Crossbite (uni./bilat.)Normal bite
Normal Makes faces while swallowing
Level 0 Level 1 Level 2 Level 3 Level 4 Level 5Frenectomy Tongue tip
touches the palateAlmost touchesthe palate
The distance between the upper and lower incisors is the same
Reacheslower incisors
Doesn’t reach lower incisors
5
13 Adenoids:
Phonetical test(morning)
Positive (different)
Negative (same)
Endoscopy (only ENT)No obstruction
Partial obstructionProfile X-ray (only orthodontists) Severe obstruction
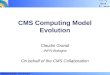
RESULTS for AGE RANGE: 4 to 7 years SAMPLE: 83 subjects WITH ALTERATIONS WITHOUT ALTERATIONS
BREATHING 68 : 81,92%
15 : 18,07%
MALOCLUSSION 70 : 84,33% 13 : 15,66%
SWALLOWING 53 : 63,85% 30 : 36,14%
POSTURE 18 : 21,68% 65 : 78,31%
CONTROL: 58 subjects WITH ALTERATIONS WITHOUT ALTERATIONS
BREATHING 21: 36,20%
37 : 63,79%
MALOCLUSSION 46 : 79,31% 12 : 20,68%
SWALLOWING 22 : 37,93% 36 : 62,06%
POSTURE 9 : 15,51% 49 : 84,48%
We statistically analysed data relating to: Breathing, Swallowing, Malocclusion, and posture.
• In this age range, Malocclusion is the most significant (84% in the SG and 79% in the CG) with remarkable values.
• In the SG, Breathing presented significant alteration (82%). Dysfunctional Swallowing is observed in a considerable percentage of children of this age (64%), but it must be kept in mind that in terms of evolution the swallowing function may have not yet matured.
• However, in the CG, Breathing and Swallowing present a significantly lower percentage of alteration.
• The percentage of Altered Posture in this age range is not significant (15 to 22%)
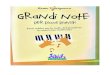
RESULTS for AGE RANGE: 8 to 11 years SAMPLE: 68 subjects WITH ALTERATIONS WITHOUT ALTERATIONS
BREATHING 38 : 55,88%
30 : 44,11%
MALOCCLUSSION 56 : 82,35% 12 : 17,64%
SWALLOWING 40 : 58,82% 28 : 41,17%
POSTURE 25 : 36,76% 43 : 63,23% CONTROL: 95 subjects WITH ALTERATIONS WITHOUT ALTERATIONS
BREATHING 36 : 37,89%
59 : 62,10%
MALOCCLUSION 80 : 84,21% 15 : 15,78%
SWALLOWING 57 : 60,00% 38 : 40,00%
POSTURE 29 : 30,52% 66 : 69,47%
• Malocclusion continues to be the prevalent alteration with a high percentage in both the SG (82%) and the CG (84%).
• Altered Swallowing also presents significant presence in both groups (59% in the SG and 60% in the CG).
• Breathing presents more alteration in the SG (56%) than the CG (38%). • In this age range, Posture shows alteration in similar percentages that are considerable in
both groups (37% in the SG and 31% in the CG). This situation is not repeated in the other two age ranges.
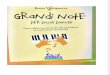
RESULTS for AGE RANGE: 12 to 16 years
SAMPLE: 34 subjects WITH ALTERATIONS WITHOUT ALT.
BREATHING 21 : 61,76 %
13 : 38,23%
MALOCCLUSION 26 : 76,47 % 8 : 23,52%
SWALLOWING 27 : 79,41 % 7 : 20,58%
POSTURE 12 : 35,29 % 22 : 64,70%
CONTROL: 34 subjects WITH ALTERATIONS WITHOUT ALT.
BREATHING 10 : 29,41 %
24 : 70,58 %
MALOCCLUSION 23 : 67,64 % 11 : 32,35 %
SWALLOWING 15 : 44,11% 19 : 55,88 %
POSTURE 6 : 17,64 % 28 : 82,35 %
• Malocclusion is significantly present in both the SG (76%) and the CG (68%). • In this age range, dysfunctional SWALLOWING is the most altered function in the SG
(79%). Altered Respiration presents a some what lower percentage (62%), and both values decrease in the CG.
• Altered Posture presents a not unimportant percentage (35%) in the SG; a value which decreases by half in the CG.
CONCLUSIONS:
• MALOCCLUSION is present in high percentages in all age groups for both the SG and CG (68-84%). • BREATHING is altered in more than 50% of the SG (max. 82% in 4-7 years), a figure that clearly declines in the CG • SWALLOWING shows a higher percentage of alteration in the SG (64- 79%), with the exception of the intermediate age group, in which the alterations show similarity between the SG and CG
(60%). • POSTURE shows the least percentage of alteration in the three age groups, although it must be said that even if the percentage of alterations is not significant among younger patients (15-22%),
this percentage does increase among the older subjects.
- The usefulness of the Protocol is evident as an interdisciplinary tool in the early detection and referral of not only children and adolescents who consult us with orofacial dysfunctions, but also others who may have undetected orofacial dysfunctions. - This way we can direct each patient to the appropriate professionals to conduct the correct diagnosis and necessary treatment at the earliest possible stage.
- Therefore, this protocol represents an essential tool for the individual evaluation if one wishes to give the diagnostic a multidisciplinary focus. - It would be interesting to conduct further studies in different populations, in the three age ranges evaluated, to collect results regarding the prevalence of orofacial alterations and dysfunctions, compare the results and establish lines of intervention.
81,92
36,20
84,33 79,31
63,85
37,93
21,68
15,51
0
10
20
30
40
50
60
70
80
90
100
Títu
lo d
el e
je
MALOCCLUSION BREATHING SWALLOWING POSTURE
SAMPLE GROUP CONTROL GROUP
55,88
37,89
82,35 84,21
58,82 60,00
36,76
30,52
0
10
20
30
40
50
60
70
80
90
100
BREATHING MALOCCLUSION SWALLOWING POSTURE
SAMPLE GROUP CONTROL GROUP
61,76
29,41
76,47
67,64
79,41
44,11
35,29
17,64
0
10
20
30
40
50
60
70
80
90
100
BREATHING MALOCCLUSION SWALLOWING POSTURE
SAMPLE GROUP CONTROL GROUP
Bibliographic references: Arne& GW, Bergman Rt. Facial Keys to orthodon;c diagnosis and treatment planning-‐ Part I. Am J Orthod Dentofacial Orthop. 1993; 103: 299-‐312 -‐ Part II. Am J Orthod Dentofacial Orthop. 1993; 103: 395-‐411. Coromina J, Es;vill E. Tratamiento del niño roncador y/o con apnea obstruc;va del sueño: la reducción amigdalar con láser. En: Coromina J, Es;vill E. El niño roncador. El niño con síndrome de apnea obstruc;va del sueño. Barcelona. 2ª Ed. EDIMSA 2006: 41-‐68. Donato G, Lapitz L, Grandi D. Protocolo de exploración Interdisciplinar orofacial para niños y adolescentes. Revista Logopèdia. Col·∙legi de Logopedes de Catalunya (16), gener 2009. Durán J. Mul;func;on System “MFS”. Las 8 claves de la matriz funcional. Ortodoncia clínica. 2003; 6: 10-‐13. Durán J. Técnica MFS: Diagnós;co de la matriz funcional: codificación. Ortodoncia clínica. 2003; 6:138-‐40. Echarri P, Carrasco A, Vila E, Boini E. Protocolo de exploración Interdisciplinar orofacial para niños y adolescentes. Revista Ortod. Esp., 2009; 49 (2); 107-‐115 Echarri P, Pérez JJ. Historia clínica, examen clínico y estudio de modelos. En Echarri P. Diagnós;co en ortodoncia: estudio mul;disciplinario. Barcelona. Nexus. 2002: 57-‐102. Grandi D, Donato G. Terapia Miofuncional. Diagnós;co y Tratamiento. Lebón, Barcelona, 2006. Ustrell J, Durán J. Diagnós;co en ortodoncia. En Ustrell J, Durán J. Ortodoncia. Primera edición. Barcelona. Ed. Universitat de Barcelona. 2001:61-‐100.
Disclosure: D. Grandi, E. Bottini and L. Lapitz have no relevant financial or non financial relationships to disclose.
[email protected] [email protected] [email protected]