Embed Size (px)
DESCRIPTION
Citation preview

Diagnostic evaluation of hypertensionHany A. AbdelWahab
(Assistant lecturer of cardiology)Zagazig University
October, 2011

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Aim of the diagnostic procedures
1) Establishing blood pressure levels.
2) Identifying secondary causes of hypertension.
3) Evaluating the overall cardiovascular risk by
searching for other risk factors, target organ
damage and concomitant diseases.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
The diagnostic procedures comprise:
1) Repeated blood pressure measurements.
2) Medical history.
3) Physical examination.
4) Investigations.

BLOOD PRESSURE MEASUREMENTS

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Blood pressure is characterized by large
spontaneous variations therefore the diagnosis
of hypertension should be based on at least 2
blood pressure measurements per visit and at
least 2 to 3 visits, although in severe cases the
diagnosis can be based on measurements taken
at a single visit.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Office or clinic BP measurement
• Allow the patients to sit for several minutes in a quiet room before beginning BP measurements.
• Take at least two measurements spaced by 1– 2 minutes, and additional measurements if the first two are quite different.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Use a standard bladder size (12–13 cm long and 35 cm wide) but have a larger and a smaller bladder available for fat and thin arms, respectively. Use the smaller bladder in children.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Have the cuff at the heart level, whatever the position of the patient.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Measure BP in both arms at the first visit to detect possible differences due to PVD. In this instance, take the higher value as the reference one.
• Measure BP 1 and 5 min after assumption of the standing position if postural hypotension is suspected like in elderly & diabetic patients.
• Measure heart rate by pulse palpation (at least 30 sec) after the second measurement in the sitting position.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Ambulatory BP measurement

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Many studies have also shown that ambulatory blood pressure:
1) Correlates with hypertension-related organ damage and its changes by treatment more closely than does office blood pressure.
2) It can predict cardiovascular risk greater than office blood pressure values in populations as well as in untreated and treated hypertensives.
3) Measures the extent of blood pressure reduction by treatment more accurately than clinic blood pressure.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• It obtains information on both daytime and nighttime BP profiles, day-night BP difference, morning BP rise and BP variability.
• The prognostic value of nighttime BP has been found to be superior to that of daytime blood pressure.
• Subjects in whom nocturnal decrease in blood pressure is blunted (non dippers) have been reported to have a greater prevalence of organ damage and a less favourable outcome.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• 24-h ambulatory BP monitoring should be considered, in particular, when:
1- Considerable variability of office BP.
2- High office BP is measured in subjects otherwise at low total cardiovascular risk.
3- There is a marked discrepancy between BP values measured in the office and at home.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
4- Resistance to drug treatment is suspected.
5- Hypotensive episodes are suspected, particularly in elderly and diabetic patients.
6- Office BP is elevated in pregnant women and preeclampsia is suspected.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Home BP measurement

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Self-measurement of BP at home is of clinical value and its prognostic significance is now demonstrated.
• These measurements should be encouraged in order to:
• Provide more information on the BP lowering effect of treatment at trough.
• Improve patient’s adherence to treatment regimens.
• If there are doubts on technical reliability/ environmental conditions of ambulatory BP data.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Normal values are different for office,
ambulatory and home
BP measurements.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Blood pressure thresholds (mmHg) for definition ofhypertension with different types of measurement
BP measure type SBP DBP
Office or clinic 140 90
24 – hour 125 – 130 80
Day 130 – 135 85
Night 120 70
Home 130 - 135 85

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Isolated office (white coat) hypertension
• If the office blood pressure is persistently elevated (≥140/90 mmHg on at least 3 occasions) while daytime or 24-hour blood pressure, or home blood pressure are within their normal range.
• Isolated office hypertension may be present in about 15% of the general population and that it may account for a noticeable fraction (one third or more) of hypertensive patients.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• There is evidence that in individuals with isolated office hypertension cardiovascular risk is less than in individuals with both raised office and ambulatory blood pressure. However, several, although not all studies, have reported this condition to be associated with a prevalence of organ damage and metabolic abnormalities greater than that of normotensive subjects, which suggests that it may not be a clinically innocent phenomenon.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• This condition is more common when there is
Grade 1 (mild) hypertension in females. older ages.Non smokers. Hypertension of recent onset.Limited number of office BP measurements.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Isolated ambulatory (masked) hypertension
• The reverse phenomenon of ‘white coat hypertension’ has also been described: individuals with normal office BP (<140/90 mmHg) may have elevated ambulatory or home BP values, a condition termed ‘isolated ambulatory hypertension’ or ‘masked hypertension’.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• The prevalence in the population is about the same as that of isolated office hypertension.
• Such individuals have been shown to have greater than normal prevalence of organ damage, with an increased prevalence of metabolic risk factors compared with subjects with a truly normal blood pressure.

MEDICAL HISTORY

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Guidelines for Family and Clinical History
1. Duration and previous level of high blood pressure.2. Indications of secondary hypertension:
- Family history of renal disease (polycystic kidney).- Renal disease, urinary tract infection, haematuria, analgesic abuse (parenchymal renal disease).- Drug/substance intake: oral contraceptives, liquorice, carbenoxolone, nasal drops, cocaine, amphetamines, steroids, NSAIDs, erythropoietin, cyclosporine.- Episodes of sweating, headache, anxiety, palpitation (phaeochromocytoma).- Episodes of muscle weakness and tetany (aldosteronism).

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
3. Risk factors:- Family and personal history of hypertension and cardiovascular disease.- Family and personal history of dyslipidaemia.- Family and personal history of diabetes mellitus.- Smoking.- Dietary habits.- Obesity & amount of physical exercise. - Snoring; sleep apnea ( information also from partner)- Personality.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
4. Symptoms of target organ damage:- Brain and eyes: headache, vertigo, impaired vision, TIAs & sensory or motor deficit.- Heart: palpitation, chest pain, shortness of breath &swollen ankles.- Kidney: thirst, polyuria, nocturia & haematuria.- Peripheral arteries: cold extremities & intermittent claudications.
5. Previous antihypertensive therapy:
- Drug(s) used, efficacy and adverse effects.

PHYSICAL EXAMINATION

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Physical Examination for Secondary Hypertension, Target organ Damage and Visceral Obesity
Signs suggesting secondary hypertension
• Features of Cushing Syndrome.• Skin stigmata of neurofibromatosis (phaeochromocytoma).• Palpation of enlarged kidneys (polycystic kidney).• Auscultation of abdominal murmurs (renovascular
hypertension).• Auscultation of precordial or chest murmurs & delayed femoral
pulses (aortic coarctation or aortic disease).

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Signs of organ damage
• Brain: murmurs over carotid arteries, motor or sensory defects.
• Retina: fundoscopic abnormalities.• Heart: apical impulse, abnormal cardiac rhythms,
ventricular gallop, pulmonary rales & peripheral oedema.
• Peripheral arteries: absence, reduction, or asymmetry of pulses, cold extremities, ischaemic skin lesions.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Evidence of visceral obesity
• Increased waist circumference (standing position) M: >102 cm & W: >88 cm
• Increased body mass index: •body weight (Kg)/ height (m²)•Overweight ≥25 Kg/m² & Obesity ≥30 Kg/m²

INVESTIGATIONS

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Laboratory Investigations• Routine tests
• Fasting plasma glucose.
• Fasting lipid profile:• Serum total cholesterol• Serum LDL-cholesterol• Serum HDL-cholesterol• Serum triglycerides
• Serum potassium.
• Serum uric acid.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Serum creatinine.
• Estimated creatinine clearance (Cockroft-Gault formula) or glomerular filtration rate (MDRD formula).
• Haemoglobin and haematocrit.
• Urine analysis (complemented by microalbuminuria dipstick test and microscopic examination).
• Electrocardiogram.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Recommended tests• Echocardiogram.• Carotid ultrasound.• Quantitative proteinuria (if dipstick test positive).• Ankle-brachial BP index.• Fundoscopy.• Glucose tolerance test (if fasting plasma glucose >102
mg/dL).• Home and 24h ambulatory BP monitoring .• Pulse wave velocity measurement (where available).

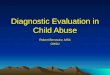
Peripheral vascular disease
Morbidity
Disability
Renal disease
CADCHFLVHStroke
Hypertension
National High Blood Pressure Education Program Working Group. Arch Intern Med. 1993;153:186-208.
Searching for subclinical organ damage

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Heart
• Electrocardiogram should be part of all routine assessment of subjects with hypertension in order to detect: LVH & patterns of “strain” - Ischaemic & conduction defects and arrhythmias.
• Echocardiography is recommended whenever a more sensitive detection of LVH & diastolic and systolic dysfunction can also be evaluated.

LVH

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• The relation between left ventricular mass index and cardiovascular risk is continuous & thresholds of 125 g/m2 for men, and 110 g/m2 for women are widely used for conservative estimates of left ventricular hypertrophy.
• Concentric hypertrophy, eccentric hypertrophy, concentric remodelling all predict an increased incidence of cardiovascular disease, but concentric hypertrophy has consistently been shown to be the condition which most markedly increases the risk.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Blood vessels
• Carotids ultrasound is also recommended whenever
detection of vascular hypertrophy (increased thickness
of common carotid intima-media; IMT > 0.9 mm ) or
asymptomatic atherosclerosis (thickening of carotid
bifurcation and internal carotid arteries, presence of
plaques) can predict the occurrence of stroke and MI.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
• Large artery stiffening (an important vascular
alteration leading to isolated systolic hypertension;
ISH in the elderly) can be measured in a relatively
simple way by pulse wave velocity.
• A low ankle- brachial BP index < 0.9 signals
peripheral artery disease.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Kidney• The diagnosis of hypertension- related renal damage
is based on the finding of a reduced renal function or the detection of albuminuria in hypertensive patients.
(A) Routine measurement of: - Serum creatinine. - Glomerular filtration rate (MDRD formula) or creatinine
clearance (Cockroft- Gault formula).- Micro and macro albuminuria (dipstick test).
This allows classification of renal dysfunction and stratification of cardiovascular risk.

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Fundoscopy• Examination of eye grounds is recommended in severe
hypertensive patients. This is because the mildest retinal changes (grade 1: arteriolar narrowing; grade 2: arterio venous nipping) appear to be largely non-specific alterations except in young patients.
• In contrast grade 3 (haemorrhages and exudates) and 4 (papilloedema), only present in severe hypertension, are associated with an increased risk of cardiovascular events.
• More sensitive methods for quantitatively assessing retinal vascular changes are being developed.


ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Brain
• Silent brain infarcts, lacunar infarction, microbleeds
and white matter lesions are not infrequent among
hypertensives and can be detected by MRI or CT
(MRI being generally superior to CT).

ESC and ESH Guidelines, 2007. European Heart Journal (2007) 28, 1462–1536
Take home message
• Proper and repeated BP measurements are essential for proper diagnosis of hypertension.
• History, physical exam and investigations are essential to search for secondary causes of hypertension, target organ damage, concomitant diseases and estimate the cardiovascular risk.

Thank You