Embed Size (px)
Citation preview
Curriculum Vitae Nama : Dr.Andri,SpKJ,FAPMLahir : Tangerang, 19 Desember 1978Pendidikan :
Dokter : Fakultas Kedokteran Universitas Indonesia (Lulus 2003)Psikiater : Fakultas Kedokteran Universitas Indonesia (Lulus 2008) Pendidikan tambahan di bidang psikosomatik medis dari American Psychosomatic Society di Portland, Oregon, USA tahun 2010 dan Academy of Psychosomatic Medicine di Atlanta, USA 2012, di Tucson 2013 dan di Fort- LeDaurdale 2014Pengakuan sebagai Fellow of The Academy of Psychosomatic Medicine (FAPM) November 2013
Organisasi :IDIPDSKJIAmerican Psychosomatic SocietyAcademy of Psychosomatic Medicine
Jabatan : Dosen Psikiatri di FK UKRIDA, JakartaKepala Klinik Psikosomatik Omni Hospital, Alam SuteraKetua Sub Kredensial Komite Medik RS OMNI Alam Sutera
PID FK UKRIDA 2015
A N D R [email protected]
Division of Psychiatry Faculty of Medicine UKRIDA
Facebook : Andri Andri Twitter : @mbahndi
Diagnosis and Treatment of Geriatric Insomnia
Introduction
Almost half of the 29 million Americans age 65 and older complain of inadequate amount or quality of sleep (Spar, 2006)The differential diagnosis of insomnia in the elderly includes the conditions listed below.
Normal Aging ChangesInsomnia Associated with Psychiatric IllnessInsomnia Associated with Physical Illnes Substance Induced InsomniaPrimary Insomnia
Normal Aging Changes
In general, with advancing age, sleep becomes more fragmented, More time is required to fall asleepMore awakenings occurRelatively less deep sleep is experienced, People tend to spend more time in bed. It is common for elderly hospitalized patients to report not sleeping at all, despite nursing observations of 6–8 hours of apparent sleep, complete with snoring
Insomnia Associated With Axis I Psychiatric Illness
Anxiety disordersMood disordersDementiaDeliriumPsychosisAdjustment disorder Normal disruptions in mental life caused by stressful or grief-producing situations
Insomnia Associated With Physical Illness
Physical conditions associated with pain (e.g., arthritis)with difficulty breathing (e.g., congestive heart failure or chronic obstructive pulmonary disease)immobility (e.g., stroke or Parkinson’s disease) urinary obstruction secondary to prostatism or chronic urinary tract infection. Sleep apnea (30%–40% of elderly patients) and is typically associated with obesity and snoring. Nocturnal myoclonus
Substance-Induced Insomnia
Sympathomimetic agents (including decongestants and bronchodilators)methylxanthine derivatives (such as theophylline and aminophylline), Psychostimulants,Certain antidepressants (fluoxetine, bupropion, higher doses of mirtazapine)Medications containing caffeine Beverages such as coffee and many cola drinksHypnotic medications
Inadequate Sleep Hygiene1. Daytime napping at least two times each week2. Having variable wake-up times or bedtimes3. Experiencing frequent periods (two to three times per week) of extendedamounts of time spent in bed4. Routinely using products containing alcohol, tobacco, or caffeine in the periodpreceding bedtime5. Scheduling exercise too close to bedtime6. Engaging in exciting or emotionally upsetting activities too close to bedtime7. Frequently using the bed for nonsleep-related activities (e.g., television watching, reading, studying, snacking)8. Sleeping on an uncomfortable bed (e.g., poor mattress, inadequate blankets)9. Allowing the bedroom to be too bright, too stuffy, too cluttered, too hot, toocold, or in some way not conducive to sleep10. Performing activities demanding high levels of concentration shortly before bed11. Allowing mental activities, such as thinking, planning, and reminiscing, tooccur in bed
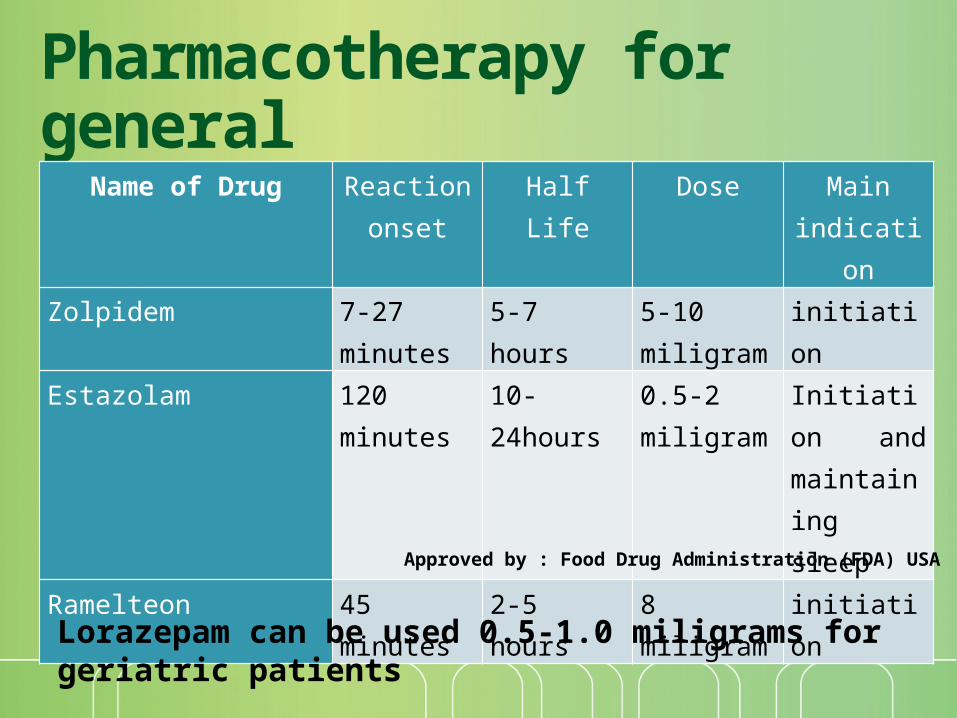
Pharmacotherapy for general
Name of Drug Reaction onset
Half Life Dose Main indication
Zolpidem 7-27 minutes
5-7 hours 5-10 miligram
initiation
Estazolam 120 minutes 10-24hours 0.5-2 miligram
Initiation and maintaining sleep
Ramelteon 45 minutes 2-5 hours 8 miligram initiation
Approved by : Food Drug Administration (FDA) USA
Lorazepam can be used 0.5-1.0 miligrams for geriatric patients
Dietary Supplements for General Use
Not FDA regulated !!!ValerianKava-KavaMelatoninPassion flowerSkullcapLavenderHops
COGNITIVE-BEHAVIORAL TREATMENT For INSOMNIA
IndicationsPrimary Insomnia
Psychophysiological InsomniaInadequate Sleep Hygiene
Comorbid InsomniaWith a medical conditionWith a mental disorder
Important to combine both cognitive and behavioral components
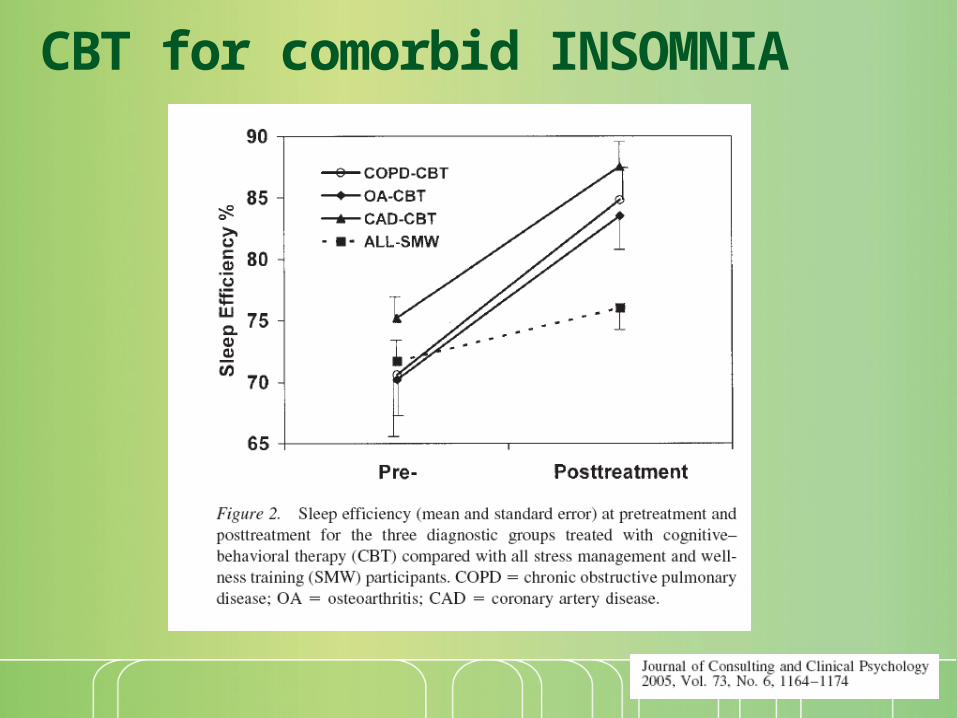
CBT for comorbid INSOMNIA
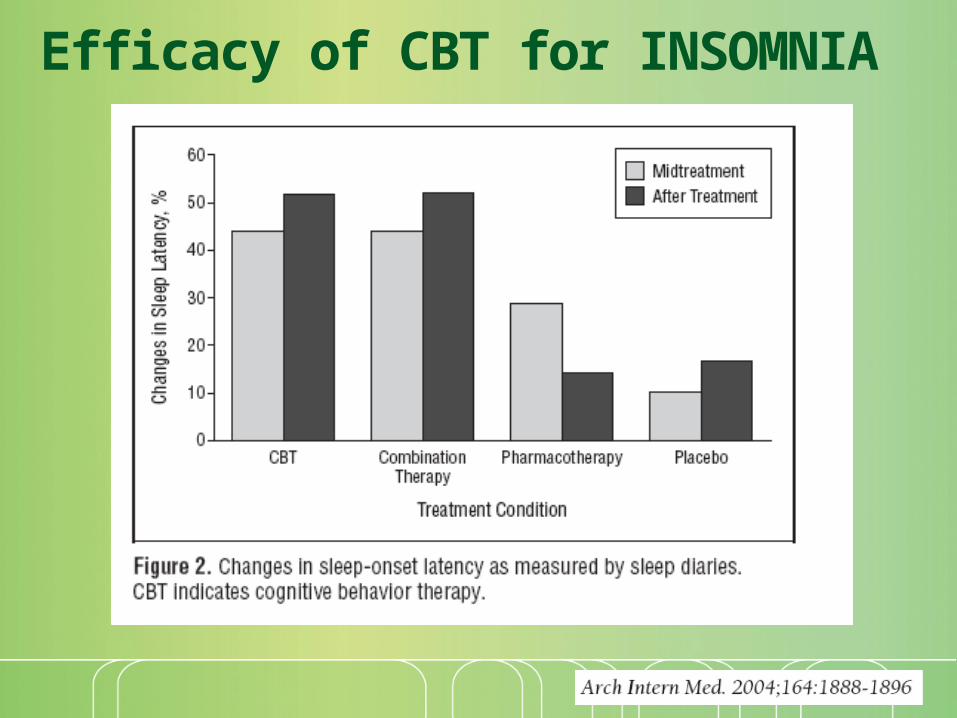
Efficacy of CBT for INSOMNIA
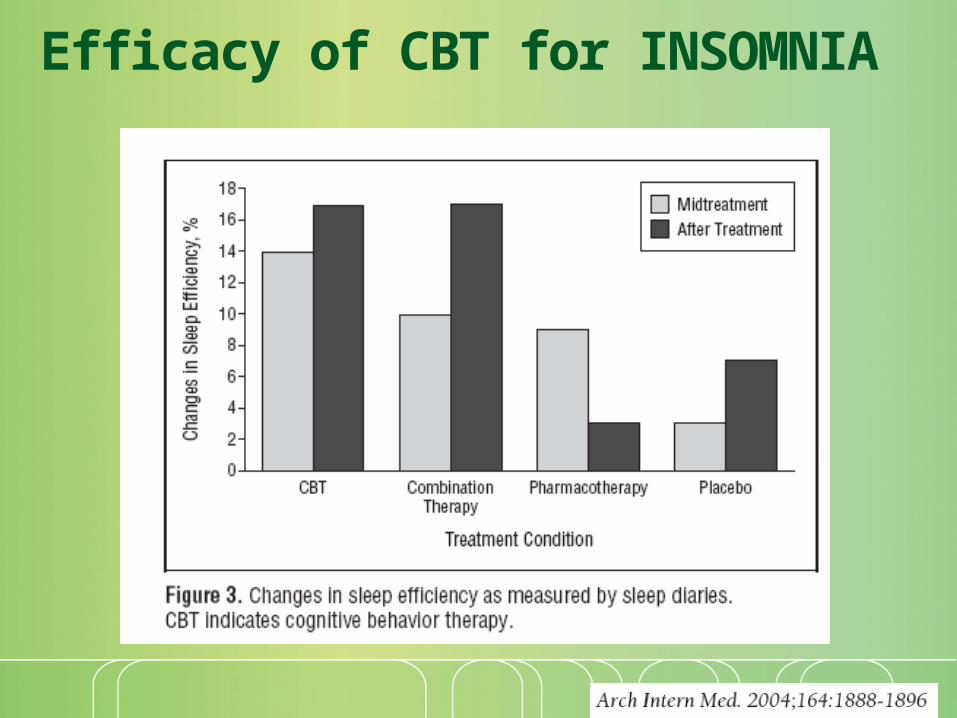
Efficacy of CBT for INSOMNIA

COGNITIVE THERAPY
Cognitive restructuringRational-Emotive therapySpecific techniques for rumination
Thought-stoppingMeditation techniques
COGNITIVE THERAPY
Five domains of cognitive activity hypothesized to contribute to insomnia
Worry and ruminationAttentional bias and monitoring for sleep-related threatUnhelpful beliefs about sleepMisperception of sleep and daytime deficitsThe use of safety behaviors that maintain unhelpful beliefs
BEHAVIORAL TREATMENTS
Sleep hygiene educationSpecific behaviors will directly interfere with the ability to sleepThe behaviors can be changed with educationNo sufficient as a ‘stand alone’ treatment
Sleep restriction therapyIncreased propensity to sleep by increasing homeostatic sleep drive with partial sleep deprivationSystematic reduction of time in bed to the amount of total sleep time from sleep log dataIncrease time in bed by 15 minutes only when sleep efficiency exceeds 90% for 5 nights
BEHAVIORAL TREATMENTS
Stimulus control therapyAssumes that there is a learned associated between wakefulness and the bedroomTo break the cycle, the patient must not spend time wide awake in the bedroomGo to bed only when sleepyDo not use the bedroom for sleep-incompatible activitiesLeave the bedroom if awake for more than 20 minutesReturn to bed only when sleepyDo not nap during the dayArise at the same time every morning
THANK YOU