Embed Size (px)
DESCRIPTION
Dentist in pune. (BDS. MDS) - Dr. Amit T. Suryawanshi. Seminar-Canine Impaction. Email ID- [email protected] Contact -Ph no.-9405622455
Citation preview

Lab investigations in Lab investigations in Dentistry & Oral surgeryDentistry & Oral surgery
Dr. Amit T. SuryawanshiDr. Amit T. SuryawanshiDentist &Oral and Maxillofacial SurgeonDentist &Oral and Maxillofacial Surgeon
Pune, IndiaPune, India
Contact details :Email ID - [email protected] No - 9405622455

My sincere thanks to youAll staff members who has Guiding my way
through this seminar topic:
MY HOD – Dr Kiran DesaiMy Guide – Dr Navin ShahMy Co Guide – Dr Rakesh ShahMy Teachers - Dr Deval Mehta Dr Dixit Shah Dr Kruti Shah Dr Arvind Agrawal Dr Rohit Tatu Dr Amit Mahajan Dr Nithin ShenoyMy colleagues – Dr Naiya pathak Dr Adarsh Desai Dr Vijayendra kumar Singh

Contents
a) Routine blood investigations:
1. Complete blood count
2. Haemoglobin
3. Erythrocytic count
4. Erythrocyte sedimentation rate
5. Total leucocyte count
6. Differential leucocyte count

Contents
7. Haematological indices:a) Packed cell volumeb) Absolute indices:1. Mean corpuscular volume2. Mean corpuscular haemoglobin3. Mean corpuscular haemoglobin
concentration. 4. Color index

Contents
8. Bleeding time & clotting time 9. Prothrombin time10. APTT11. Renal function test12. Blood glucose estimation: a) Random blood sugar b) Post prandial blood sugar13. Liver function test14. Blood group 15. Cross matching of blood16. Serum electrolytes

66
WBC CountWBC Count 4-11x 104-11x 10³ cells/mm³³ cells/mm³
RBC CountRBC Count 4.5 – 6 million/cumm4.5 – 6 million/cumm
HaemoglobinHaemoglobin 14 – 18 gm /dl14 – 18 gm /dl
HaematocritHaematocrit Men: 40 – 54%,Men: 40 – 54%,
Women: 37 – 47 %Women: 37 – 47 %
PlateletsPlatelets 150 – 400 x 10150 – 400 x 10³/mm³³/mm³
RBC IndicesRBC Indices
MCVMCV 80 – 100 fl80 – 100 fl
MCHMCH 27 – 31 pg27 – 31 pg
Blood investigations:1. Complete blood count :
MCHC 32- 36 %

77
Normal Normal valuesvalues
Increased in Increased in conditions ofconditions of
Decreased in Decreased in conditions ofconditions of
Clinical Clinical significancesignificance
Men:Men:
14 -18gm/dl,14 -18gm/dl,
Women:Women:
12-16 gm/dl,12-16 gm/dl,
Newborn:Newborn:
14 – 19 14 – 19 gm/dlgm/dl
PolycythemiaPolycythemia
vera,vera,
Dehydration,Dehydration,
Poorly Poorly compensated compensated heart disease.heart disease.
AnemiaAnemia It determines It determines oxygen oxygen carrying carrying capacity of capacity of blood.blood.
1gm of Hb 1gm of Hb contains contains 3.34 mg of 3.34 mg of iron & carries iron & carries 1.34 ml of 1.34 ml of oxygen.oxygen.
Blood investigations: 2. Haemoglobin

88
HaemoglobinHaemoglobin Haemoglobin is a chromoprotein consisting Haemoglobin is a chromoprotein consisting
of the colorless globin & four red haem of the colorless globin & four red haem molecules. Haem is a metal complex molecules. Haem is a metal complex containing an iron atom in the centre of containing an iron atom in the centre of porphyrin ring. The globin molecule consists porphyrin ring. The globin molecule consists of two peptide chains (alpha & beta), each of two peptide chains (alpha & beta), each made up of several amino acids.made up of several amino acids.
Majority of the adult haemoglobin is Majority of the adult haemoglobin is haemoglobin A ,which constitutes 95-96% of haemoglobin A ,which constitutes 95-96% of total haemoglobin .About 3% of haemoglobin total haemoglobin .About 3% of haemoglobin is haemoglobin A2, where as haemoglobin F is haemoglobin A2, where as haemoglobin F constitutes less than 2% of total constitutes less than 2% of total haemoglobinhaemoglobin..

99
Estimation of HaemoglobinEstimation of Haemoglobin1.1. Calorimetric methodsCalorimetric methods:: The principle is to convert haemoglobin to acid The principle is to convert haemoglobin to acid
haematin, alkaline haematin or haematin, alkaline haematin or cyanmethaemoglobin & compare the color of cyanmethaemoglobin & compare the color of the compound thus produced with the glass the compound thus produced with the glass standard in a comparator.standard in a comparator.
2.2. Gasometric method Gasometric method –– The oxygen carrying capacity of blood is The oxygen carrying capacity of blood is
measured & haemoglobin is estimated measured & haemoglobin is estimated indirectly.indirectly.
3.3. Chemical method Chemical method –– Haemoglobin is determined from the iron Haemoglobin is determined from the iron
content of the blood.content of the blood.

1010
Acid Haematin methodAcid Haematin method PrinciplePrinciple: : Haemoglobin is converted into acid haematin Haemoglobin is converted into acid haematin
(brown colored) by diluting with weak acid.This (brown colored) by diluting with weak acid.This resultant color is compared after dilution with a resultant color is compared after dilution with a standard brown reference glass of Sahli standard brown reference glass of Sahli haemoglobinometer.haemoglobinometer.
Range of HbRange of Hb:: InfancyInfancy - -1.1. Cord blood or New born : 14-19 gm/dlCord blood or New born : 14-19 gm/dl2.2. At 1 yearAt 1 year : 11 gm/dl : 11 gm/dl
3.3. Children (upto 10 years):Children (upto 10 years):12gm/dl12gm/dl AdultsAdults:: Males : 14-18 gm/dlMales : 14-18 gm/dl Females : 12-16 gm/dlFemales : 12-16 gm/dl

1111
Abnormal value of Hb seen in Abnormal value of Hb seen in
IncreasedIncreased : : DecreasedDecreased::1.1. Polycythemia Vera 1. AnaemiaPolycythemia Vera 1. Anaemia2.2. Dehydration 2. Haemorrhage Dehydration 2. Haemorrhage 3. Increased Altitude 3. Dilution 3. Increased Altitude 3. Dilution 4. Heavy smoking 4. Alcohol4. Heavy smoking 4. Alcohol5. Birth physiology 5. Drugs5. Birth physiology 5. Drugs 6. Pregnancy6. Pregnancy

What information is obtained from Hb & Hct values ?
The Hb is an indicator of oxygen carrying capacity of blood. It is dependent primarily on no. of RBCs & less significantly on the amount of Hb per cell. Hb is known to vary by as much as 1 gm/dl diurnally, with peaks in the morning. The relation between Hb & Hct is given by :
Hb x 3 = Hct R.B.C (millions) x 3 = Hb R.B.C x 9 = Hct

Are haemoglobin & haematocrit primary indicators of blood loss & the need for
Transfusion ? No. These are poorly early measures of bleeding
because one loses plasma & Rbc in equal measures. It takes 2 – 3 hrs or following fluid resuscitation before the Hb/Hct will reflect blood loss. Previously, surgical transfusion guidelines were 10 gm/dl or 33 % Hct , then 9 gm/dl or 25 – 30 %. Today most patients are transfused for Hb < 7 gm/dl but the best guidelines are the vital signs & symptoms such as shortness of breath & exercise tolerance. Initially low Hct value suggest chronic blood loss, which should be supported by low MCV & a high reticulocyte count.

Morphologic changes on Smears:
Poikilocytosis – Irregularly shaped RBCsAnisocytosis – Irregular RBC sizeSickle cell – Crescent or sickle shaped
RBCs seen with decreased oxygen tension.
Howel jolly bodies – Large RBC basophilic inclusions, megaloblastic anemia, splenectomy, hemolysis.

Basophilic stippling – Small RBC blue inclusions (Lead poison, thalassemia, heavy metals)
Spherocytes – Spherical RBC(autoimmune hemolytic anemia, hereditary).
Burr cells – Spiny RBC(Liver disease, anorexia, increase bile acids).
Schistocyte – Helmet RBCs(Severe anemia, hemolytic transfusion reaction).
Dohle’s inclusion bodies – PMNs (Burns,infection).
Toxic granulation – PMNs(burns, sepsis,fever). Auer bodies – Acute myelogenous leukemia. Hypersegmentation – PMNs with 6 – 7 lobes
(megaloblastic anaemia, Liver disease)

Abnormal HaemoglobinsAbnormal Haemoglobins::
Abnormalities of Hb may be associated Abnormalities of Hb may be associated either with defect in the haem molecule or the either with defect in the haem molecule or the globin molecule.globin molecule.
a)a) Defect in the haem moietyDefect in the haem moiety::
1.1. PorphyriasPorphyrias::
2.2. Formation of abnormal pigmentsFormation of abnormal pigments: : Carboxyhaemoglobin, methaemoglobin, Carboxyhaemoglobin, methaemoglobin, sulphhaemoglobin.sulphhaemoglobin.
3.3. Defect in the globin moietyDefect in the globin moiety::
a)a) QuantitativeQuantitative: eg. Thalessemia: eg. Thalessemia
b)b) QualitativeQualitative: Like formation of abnormal : Like formation of abnormal haemoglobins.They are differentiated by haemoglobins.They are differentiated by electrophoretic & chromatographic techniques. electrophoretic & chromatographic techniques.

1717
Normal Normal valuesvalues
Increased in Increased in conditions ofconditions of
Decreased in Decreased in conditions ofconditions of
Clinical Clinical significancesignificance
Adult males:Adult males:
4.5 – 5.9 4.5 – 5.9 million/cummmillion/cumm
Adult female:Adult female:
4.5 – 5.1 4.5 – 5.1 million/cummmillion/cumm
High High altitudes, altitudes, After After exercise, exercise, pregnancy, pregnancy, polycythemia polycythemia veravera
AnemiasAnemiasa)a) AplasticAplastic
b)b) HemorrhagicHemorrhagic
c)c) HemolyticHemolytic
WormWorm
infectioninfection
Bone Bone marrow marrow poisoningpoisoning
Transport of Transport of oxygen & oxygen & CO2 through CO2 through agency of agency of Hb.Hb.
Blood investigations:3.Erythrocytic count:

1818
Erythrocytic countErythrocytic count
Erythrocytes are flexible, elastic, non-Erythrocytes are flexible, elastic, non-nucleated biconcave discs. It contains a no. nucleated biconcave discs. It contains a no. of antigens on the cell surface responsible for of antigens on the cell surface responsible for blood groups.blood groups.
The function of RBC is transport of oxygen & The function of RBC is transport of oxygen & CO2 through agency of haemoglobin in a CO2 through agency of haemoglobin in a functional state with the help of enzymes functional state with the help of enzymes methaemoglobin reductase & glutathione methaemoglobin reductase & glutathione peroxidase. peroxidase.
At birth marrow is the only organ concerned At birth marrow is the only organ concerned with the production of erythrocytes. Its life with the production of erythrocytes. Its life span is 120 days. Spleen is considered as span is 120 days. Spleen is considered as the graveyard of the RBCs.the graveyard of the RBCs.

1919
ObjectiveObjective: To determine whether patient has : To determine whether patient has polycythemia Or Anaemia. polycythemia Or Anaemia.
PrinciplePrinciple::
Blood is diluted exactly 1:200 in a Thoma’s Blood is diluted exactly 1:200 in a Thoma’s pipette using an isotonic Haem’s fluid.Diluted pipette using an isotonic Haem’s fluid.Diluted blood is then placed in a haemocytometer blood is then placed in a haemocytometer chamber.The cells in the measured volume chamber.The cells in the measured volume are then counted & the figure thus obtained is are then counted & the figure thus obtained is then multiplied by an appropriate factor then multiplied by an appropriate factor (10000) to get the no. of cells per cu. mm of (10000) to get the no. of cells per cu. mm of blood.blood.

EquipmentEquipment::1.1. Thoma’s pipette with red bead Thoma’s pipette with red bead
(R.B.C.pipette)(R.B.C.pipette)2.2. Levy- Hausser chamber with improved Levy- Hausser chamber with improved
Neubauer ruling.Neubauer ruling.3.3. Diluting fluidDiluting fluidHaem’s solutionHaem’s solution::1.1. Sodium sulphate : 2.5 gmsSodium sulphate : 2.5 gms2.2. Sodium chloride : 0.5 gmsSodium chloride : 0.5 gms3.3. Mercuric chloride : 0.25 gmsMercuric chloride : 0.25 gms4.4. Distilled water to 100 mlDistilled water to 100 ml

2121
Adult females : 4.5 – 5.1 million/cu. mm Adult females : 4.5 – 5.1 million/cu. mm Adult males : 4.5 – 5.9 million/cu. MmAdult males : 4.5 – 5.9 million/cu. Mm The abnormal values for erythrocyte The abnormal values for erythrocyte
count are seen in :count are seen in : IncreasedIncreased DecreasedDecreased
1.1. High altitudes AnaemiasHigh altitudes Anaemias
2.2. After exercise 1. AplasticAfter exercise 1. Aplastic
3.3. Pregnancy 2. HaemorrhagicPregnancy 2. Haemorrhagic
4.4. Polycythemia vera 3. HemolyticPolycythemia vera 3. Hemolytic

2222
Normal values Normal values at the end of 1 at the end of 1 hrhr
Increased in Increased in cases ofcases of
Decreased in Decreased in cases ofcases of
Clinical Clinical significancesignificance
Wintrobe’s Wintrobe’s method:method:
Males:Males:
0 – 7.5 mms0 – 7.5 mms
Females:Females:
0 – 15 mms0 – 15 mms
Westergren’s Westergren’s method:method:
Males Males 0 – 15 mm0 – 15 mm
Females:Females:
0 – 20 mm0 – 20 mm
Acute & Acute & chronic chronic infections,infections,
Malignancy,Malignancy,
Rheumatoid Rheumatoid arthritis,arthritis,
Tuber Tuber sclerosis, sclerosis,
Anaemia,Anaemia,
M.I.M.I.
Polycythemia,Polycythemia,
C.C.F.C.C.F.Useful in Useful in distinguishing distinguishing functional functional from organic from organic disease.disease.
Blood investigations:4.E.S.R.

2323
Erythrocyte Sedimentation RateErythrocyte Sedimentation Rate If an anticoagulant is added to a specimen of blood & If an anticoagulant is added to a specimen of blood &
the blood is allowed to stand in a tube , erythrocytes the blood is allowed to stand in a tube , erythrocytes settle at the bottom of tube, while the plasma remains settle at the bottom of tube, while the plasma remains as a clear supernatant fluid. The rate at which the as a clear supernatant fluid. The rate at which the erythrocytes settle is known as erythrocyte erythrocytes settle is known as erythrocyte sedimentation rate.sedimentation rate.
PrinciplePrinciple:: Sedimentation is due to changes on the surface charge Sedimentation is due to changes on the surface charge
of RBCs,which tend them to aggregate.These changes of RBCs,which tend them to aggregate.These changes are related to alterations in the plasma.Increase in are related to alterations in the plasma.Increase in fibrinogen & cholesterol causes acceleration of fibrinogen & cholesterol causes acceleration of E.S.R.The larger the volume of RBCs the more rapid is E.S.R.The larger the volume of RBCs the more rapid is the sedimentation.It takes place in three stages the sedimentation.It takes place in three stages namely:namely:
1.1. Formation of rouleaux Formation of rouleaux 2.2. Sinking of rouleauxSinking of rouleaux3.3. Packing of rouleauxPacking of rouleaux

2424
Factors influencing E.S.R :Factors influencing E.S.R :1.1. Fasting sample of blood should be used.Fasting sample of blood should be used.2.2. Vertical position of tube.Vertical position of tube.3.3. Temperature must be constant.Temperature must be constant.4. There should be no haemolysis.4. There should be no haemolysis. MethodsMethods:: There are two methods of estimation of E.S.R. viz.There are two methods of estimation of E.S.R. viz.1.1. Wintrobe methodWintrobe method2.2. Westergen’s methodWestergen’s method3.3. Wintrobe methodWintrobe method:: EquipmentEquipment: All equipment for collection of venous : All equipment for collection of venous
blood,oxalated blood, wintrobe’s haemotocrit tube with blood,oxalated blood, wintrobe’s haemotocrit tube with gradations from 0 to 10 from above downwards.gradations from 0 to 10 from above downwards.
SpecimenSpecimen: Oxalated venous blood sample is : Oxalated venous blood sample is used.This investigation should be done within an hour used.This investigation should be done within an hour of the collection of the blood.This oxalated blood of the collection of the blood.This oxalated blood sample should be gently shaked before doing the test.sample should be gently shaked before doing the test.

2525
MethodMethod::1.1. Fill the wintrobe’s tube up to mark 10 with Fill the wintrobe’s tube up to mark 10 with
blood by putting the pipette to the bottom of blood by putting the pipette to the bottom of the tube & then fill from below upward. During the tube & then fill from below upward. During the maneuver gradually withdraw the pipette, the maneuver gradually withdraw the pipette, no air bubbles should get inside the column of no air bubbles should get inside the column of the blood.the blood.
2.2. Set the tube in a vertical position in the stand.Set the tube in a vertical position in the stand.3.3. Record the reading at the end of 1 hour.Record the reading at the end of 1 hour.4.4. If anaemia is present, do PCV & find out the If anaemia is present, do PCV & find out the
anemia correction factor from the chart.anemia correction factor from the chart. Normal valuesNormal values:: At the end of one hour:At the end of one hour: Males: 0 – 7.5 mmsMales: 0 – 7.5 mms Females: 0 – 15 mmsFemales: 0 – 15 mms

AdvantagesAdvantages::
1.1. Technically it is a convenient method.Technically it is a convenient method.
2.2. There is no factor of dilution by anticoagulant.There is no factor of dilution by anticoagulant.
3.3. P.C.V & E.S.R can be done on the same P.C.V & E.S.R can be done on the same sample.sample.
UsesUses::
1.1. Estimation of E.S.REstimation of E.S.R
2.2. Estimation of P.C.VEstimation of P.C.V
3.3. From the thickness of buffy coat of leucocytes From the thickness of buffy coat of leucocytes one can suspect the presence of leukemia.one can suspect the presence of leukemia.
4.4. From the yellowish appearance of the From the yellowish appearance of the supernatant plasma, one can suspect Jaundice.supernatant plasma, one can suspect Jaundice.

2727
Significance of E.S.R.Significance of E.S.R. : :
Serial E.S.R estimations are useful in Serial E.S.R estimations are useful in prognosis of certain diseases & in prognosis of certain diseases & in evaluation of their treatment. These evaluation of their treatment. These diseases are tuberculosis, A.R.F. & M.I., diseases are tuberculosis, A.R.F. & M.I., Infections , after vaccination or injection of Infections , after vaccination or injection of foreign proteins.foreign proteins.
E.S.R. is low in polycythemia & C.C.F.E.S.R. is low in polycythemia & C.C.F.

2828
Blood investigations:Blood investigations:5. 5. Total Leucocyte CountTotal Leucocyte Count
PrinciplePrinciple:: Blood is diluted exactly 1 in 20 in a leucocyte pipette Blood is diluted exactly 1 in 20 in a leucocyte pipette
using leucocyte diluting fluid.Diluted blood is then put using leucocyte diluting fluid.Diluted blood is then put in a haemocytometer. Leucocytes in the measured in a haemocytometer. Leucocytes in the measured volume are counted. This figure is multiplied by an volume are counted. This figure is multiplied by an appropriate factor to get the no. of leucocytes per cu. appropriate factor to get the no. of leucocytes per cu. Mm of blood. If count is suspected to be very high e.g. Mm of blood. If count is suspected to be very high e.g. in leukemia, higher dilution is done employing in leukemia, higher dilution is done employing erythrocyte pipette.erythrocyte pipette.
EquipmentEquipment::1.1. Haemocytometer with Neubauer ruling.Haemocytometer with Neubauer ruling.2.2. W.B.C. pipette with white bead.W.B.C. pipette with white bead.3.3. Leucocyte diluting fluid.Leucocyte diluting fluid.

CompositionComposition: : Glacial acetic 3 ml ( lyse the RBC)Glacial acetic 3 ml ( lyse the RBC)Methylene blue Few drops(coloring agent Methylene blue Few drops(coloring agent
which renders nuclei prominent)which renders nuclei prominent)Distilled water 97 mlDistilled water 97 mlNormal valuesNormal values : :Adults: 4000 – 11000 per cu. mm. of bloodAdults: 4000 – 11000 per cu. mm. of blood Infants:10000 – 20000 per cu.mm.of bloodInfants:10000 – 20000 per cu.mm.of blood

3030
Blood investigationsBlood investigations::6. 6. Differential Leucocyte countDifferential Leucocyte count
The relative proportion of different series of leucocytes The relative proportion of different series of leucocytes can be known by examination of stained blood smear. can be known by examination of stained blood smear. It is expressed in term of the percentage of each type It is expressed in term of the percentage of each type of leucocyte out of total of 100.of leucocyte out of total of 100.
MethodMethod::1.1. Preparation of blood smearPreparation of blood smear:: A small drop of blood is placed in the centre of the A small drop of blood is placed in the centre of the
slide. The spreading edge of the spreader is then slide. The spreading edge of the spreader is then placed at an angle of 30 - 40placed at an angle of 30 - 40° on the slide, just in front ° on the slide, just in front of the drop & moved little back so as to touch the drop. of the drop & moved little back so as to touch the drop. As soon as the contact is made the drop will quickly As soon as the contact is made the drop will quickly spread by a rapid smooth forward movement of the spread by a rapid smooth forward movement of the spreader. Dry the smear in the air.spreader. Dry the smear in the air.

Criteria of a Good smearCriteria of a Good smear::
a)a)A good smear must have even surface A good smear must have even surface free from ridges, waves & holes.free from ridges, waves & holes.
b)b) Smear should not extend to the edge or to Smear should not extend to the edge or to the end of the side, but must be atleast 2 “ the end of the side, but must be atleast 2 “ long.long.
c)c) The leucocytes must not be bunched at The leucocytes must not be bunched at the edges or near the end.the edges or near the end.
d)d) The smear should be thin enough, such The smear should be thin enough, such that the erythrocytes just touch each other that the erythrocytes just touch each other but do not overlap.but do not overlap.

3232
Abnormal values for different leucocytesAbnormal values for different leucocytes::1.1. LeucocytosisLeucocytosis:: Common causes are as follows:Common causes are as follows:a)a) Infection: Pyogenic infectionInfection: Pyogenic infectionb)b) Inflammatory conditions:Inflammatory conditions:1.1. Rheumatic feverRheumatic fever2.2. Ischemic necrosisIschemic necrosisc)c) Haematological : C.M.L.Haematological : C.M.L.d)d) Physiological: Heat, exercise, pain.Physiological: Heat, exercise, pain.e)e) Malignant neoplasia: eg. Bronchogenic carcinomaMalignant neoplasia: eg. Bronchogenic carcinomaf)f) Diabetic ketoacidosisDiabetic ketoacidosisg)g) Acute GoutAcute Gouth)h) EclampsiaEclampsiai)i) Tissue damage (M.I., Burn or crush injury)Tissue damage (M.I., Burn or crush injury)j)j) Late PregnancyLate Pregnancyk)k) LabourLabourl)l) NewbornNewborn

3333
2.2. EosinophiliaEosinophilia::
IncreasedIncreased: : DecreasedDecreased::a) Parasitic infection: a) Steroidsa) Parasitic infection: a) Steroids
Intestinal helminths, b) Stress (Infection,Intestinal helminths, b) Stress (Infection,
filaria & guineaworm. Trauma, Burn)filaria & guineaworm. Trauma, Burn)
b) Allergic diseases: c) Increased ACTHb) Allergic diseases: c) Increased ACTH
Asthma, Hay fever, Urticaria. d) Cushing’s syndromeAsthma, Hay fever, Urticaria. d) Cushing’s syndrome
c) Skin disease: c) Skin disease:
Scabies, eczema,Scabies, eczema,
exfoliative dermatitis, pemphigus etc.exfoliative dermatitis, pemphigus etc.
d) Tropical eosinophiliad) Tropical eosinophilia
e) Haematological : C.M.L.e) Haematological : C.M.L.
f) Addison’s diseasef) Addison’s disease
g) Collagen vascular diseases.g) Collagen vascular diseases.

3434
3.3. BasophiliaBasophilia:: IncreasedIncreased DecreasedDecreased
a)a) C.M.L. a) Acute rheumatic FeverC.M.L. a) Acute rheumatic Fever
b)b) Polycythemia b) Lobar pneumoniaPolycythemia b) Lobar pneumonia
c)c) After recovery c) Steroid treatmentAfter recovery c) Steroid treatment
of infection, or d) Stressof infection, or d) Stress
hypothyroidism e) Thyrotoxicosishypothyroidism e) Thyrotoxicosis
(rarely). (rarely).

3535
LymphocytesLymphocytes:: IncreasedIncreased (Lymphocytosis) (Lymphocytosis) DecreasedDecreased : :
a)a) Viral Infections a) UremiaViral Infections a) Uremia
b)b) Acute or chronic b) StressAcute or chronic b) Stress
c) lymphocytic Leukemia c) Burnsc) lymphocytic Leukemia c) Burns
d) Tuberculosis d) Traumad) Tuberculosis d) Trauma
e) Mononucleosis e) Steroidse) Mononucleosis e) Steroids
f) Normal in 20%f) Normal in 20%
of populationof population

3636
MonocytesMonocytes:: Increased (Monocytosis): Decreased:Increased (Monocytosis): Decreased:
a)a) Subacute bacterial a) Aplasia of bone marrow Subacute bacterial a) Aplasia of bone marrow
endocarditisendocarditis
b)b) TBTB
c)c) Protozoal infectionProtozoal infection
d)d) LeukemiaLeukemia
e)e) Collagen diseaseCollagen disease

3737
LeucopeniaLeucopenia:: It is decreased in total no. of leucocytes below It is decreased in total no. of leucocytes below
4000/cu. mm.4000/cu. mm.1.1. Infection: Enteric fever, influenza, measles, Infection: Enteric fever, influenza, measles,
kala azar etc.kala azar etc.2.2. Severe intoxications: By arsenic, Severe intoxications: By arsenic,
sulphonamides, X-ray & radium exposure due sulphonamides, X-ray & radium exposure due to bone marrow damage.to bone marrow damage.
3.3. Blood disease : Severe aplastic anaemia, Blood disease : Severe aplastic anaemia, agranulocytosis.agranulocytosis.
4.4. Disease associated with hypersplenism.Disease associated with hypersplenism.5.5. Nutritional deficiency: Malnutrition, starvation, Nutritional deficiency: Malnutrition, starvation,
cachexia & debility. Leucopenia is usually due cachexia & debility. Leucopenia is usually due to neutropenia consequent to diminished to neutropenia consequent to diminished production in the marrow,increased destruction production in the marrow,increased destruction & loss from circulation due to sequestration in & loss from circulation due to sequestration in the internal organs.the internal organs.

3838
Blood investigations:Blood investigations:Haematological indicesHaematological indices
PurposePurpose : :1.1. To correlate erythrocytic count & haemoglobin To correlate erythrocytic count & haemoglobin
estimation.estimation.2.2. To find out the degree of hemoconcentration.To find out the degree of hemoconcentration.3.3. Morphological classification of anemia, which is helpful Morphological classification of anemia, which is helpful
to some extent in devising the specific treatment.to some extent in devising the specific treatment.4.4. To find out if anaemia or polycythemia is present.To find out if anaemia or polycythemia is present. It includes :It includes :a)a) Packed cell volume (P.C.V.)Packed cell volume (P.C.V.)b)b) Absolute indicesAbsolute indices

3939
Packed cell volume or HaematocritPacked cell volume or Haematocrit::
when a known volume of oxalated when a known volume of oxalated blood is cetrifuged at a constant speed & blood is cetrifuged at a constant speed & for a constant time, the percentage of the for a constant time, the percentage of the total blood volume occupied by the total blood volume occupied by the packed erythrocytes is known as Packed packed erythrocytes is known as Packed cell volume (P.C.V.) or haematocrit.cell volume (P.C.V.) or haematocrit.
EquipmentEquipment::
1.1. Wintrobe’s tubeWintrobe’s tube
2.2. Pasteur’s pipettePasteur’s pipette

4040
3. High speed centrifuge machine.3. High speed centrifuge machine. SpecimenSpecimen: Oxalated venous blood sample is : Oxalated venous blood sample is
gently shaken before use.gently shaken before use. MethodMethod::
Blood is taken in wintrobe’s haematocrit Blood is taken in wintrobe’s haematocrit tube, upto mark 10 & centrifuged at 3000 tube, upto mark 10 & centrifuged at 3000 r.p.m. for 45 min. By this time the erythrocytes r.p.m. for 45 min. By this time the erythrocytes are packed at the bottom & superimposed on are packed at the bottom & superimposed on them is the layer of leucocytes & them is the layer of leucocytes & platelets( buffy layer). Height of column of platelets( buffy layer). Height of column of erythrocytes in mm. gives the % P.C.V.erythrocytes in mm. gives the % P.C.V.
Normal valuesNormal values::
1.1. Male: 41.5 – 50.4 %Male: 41.5 – 50.4 %

4141
1.1. Female: 35.9 – 44.6 %Female: 35.9 – 44.6 % Packed cell volume is altered by change Packed cell volume is altered by change
in erythrocytic count or change in size of in erythrocytic count or change in size of erythrocyte.erythrocyte.
ImportanceImportance::1.1. Fall in values is seen in : AnaemiaFall in values is seen in : Anaemia2.2. Increase in values is seen in : Increase in values is seen in :
Polycythemia, Dehydration.Polycythemia, Dehydration.3.3. Color & opacity of plasmaColor & opacity of plasma : :a)a) Yellow in jaundiceYellow in jaundiceb)b) Milky in LipemiaMilky in Lipemiac)c) Cloudy in plasma cell myelomaCloudy in plasma cell myelomad)d) Red in haemolysisRed in haemolysis

4242
e) Reddish gray layer of packed leucocytes & e) Reddish gray layer of packed leucocytes & platelet ( buffy layer). Normally 0.5 – 1mm in platelet ( buffy layer). Normally 0.5 – 1mm in thickness. Platelets are on upper part of the thickness. Platelets are on upper part of the layer.layer.
2. 2. Absolute indicesAbsolute indices : :
For finding out the absolute indices we For finding out the absolute indices we require:require:
1.1. Haemoglobin (gms %)Haemoglobin (gms %)
2.2. Erythrocytes (millions/c. mm.)Erythrocytes (millions/c. mm.)
3.3. Packed cell volume (P.C.V.)Packed cell volume (P.C.V.)

4343
Important absolute indices are as follows:Important absolute indices are as follows:
1.1. Mean corpuscular volume( M.C.V.)Mean corpuscular volume( M.C.V.)
2.2. Mean corpuscular haemoglobin (M.C.H.)Mean corpuscular haemoglobin (M.C.H.)
3.3. Mean corpuscular haemoglobin concentration Mean corpuscular haemoglobin concentration (M.C.H.C.)(M.C.H.C.)
4.4. Color index (C.I.)Color index (C.I.)

4444
Mean corpuscular volume ( M.C.V.):Mean corpuscular volume ( M.C.V.):
It is the volume of average erythrocyte in It is the volume of average erythrocyte in cubic microns. It is calculated by formula.cubic microns. It is calculated by formula.
MCV = MCV = PCV(%)x10/Erythrocytes(millions per cu. PCV(%)x10/Erythrocytes(millions per cu. mm)mm)
Normal values: 80 – 96 cu. micronsNormal values: 80 – 96 cu. microns

4545
VariationsVariations: : MacrocyticMacrocytic(>100 cu.microns):(>100 cu.microns):
Megaloblastic anaemia(BMegaloblastic anaemia(B¹² or folate ¹² or folate deficiency), Chronic liver disease, deficiency), Chronic liver disease, alcoholism,reticulocytosis,physiologic for alcoholism,reticulocytosis,physiologic for new born.new born.
MicrocyticMicrocytic(<80 cu. microns):(<80 cu. microns):
Iron deficiency, thalassemia, chronic Iron deficiency, thalassemia, chronic disease (cancer, renal, infection), or lead disease (cancer, renal, infection), or lead toxicity.toxicity.

4646
Mean corpuscular haemoglobinMean corpuscular haemoglobin : :
It is the amount of haemoglobin present in It is the amount of haemoglobin present in an average erythrocyte in picograms. It is an average erythrocyte in picograms. It is calculated by the formula.calculated by the formula.
M.C.H. = Hb M.C.H. = Hb (gm)x10/Erythrocytes(millions per cu. (gm)x10/Erythrocytes(millions per cu. mm).mm).
Normal values:27.5 – 33.2 pgNormal values:27.5 – 33.2 pg

4747
SignificanceSignificance::
MCH helps to diagnose chromaticity of MCH helps to diagnose chromaticity of cells because increased Hb content cells cells because increased Hb content cells will have more pigment (hyperchromic) & will have more pigment (hyperchromic) & will be hypochromic in the reverse will be hypochromic in the reverse situation.This tends to parallel changes in situation.This tends to parallel changes in MCV in that macrocytic cells are usually MCV in that macrocytic cells are usually hyperchromic & microcytic or hypochromic hyperchromic & microcytic or hypochromic cells have low MCH.cells have low MCH.

4848
Mean corpuscular haemoglobin Mean corpuscular haemoglobin concentration : (M.C.H.C)concentration : (M.C.H.C)
M.C.H.C = Hb (gm) x 100 /P.C.VM.C.H.C = Hb (gm) x 100 /P.C.V Normal value: 33.4 – 35.5 %Normal value: 33.4 – 35.5 % Increased Increased DecreasedDecreased
1.1. Prolonged severe Prolonged severe Overhydration,Overhydration,
Dehydration Iron deficiencyDehydration Iron deficiency
2.2. Heavy smoking anaemia,Heavy smoking anaemia,
3.3. Intravascular hemolysis Thalassemia,Intravascular hemolysis Thalassemia,
4.4. Spherocytosis SideroblasticSpherocytosis Sideroblastic
anaemiaanaemia

4949
Color index (C.I.)Color index (C.I.)::
It is the average amount of haemoglobin in It is the average amount of haemoglobin in a red cell in comparison to normal.a red cell in comparison to normal.
Color index = Hb (%)/RBC(%)Color index = Hb (%)/RBC(%)
Normal value : 0.85 – 1.15Normal value : 0.85 – 1.15
Abnormal values:Abnormal values:
Low color index : seen in Hypochromic Low color index : seen in Hypochromic anaemiaanaemia
High color index :seen in Megaloblastic High color index :seen in Megaloblastic anaemia.anaemia.

5050
Bleeding time & Clotting timeBleeding time & Clotting time::
1.1. Clotting timeClotting time : :
It is the time required by blood for coagulation.It is the time required by blood for coagulation.
It is measured by Wright’s capillary method & It is measured by Wright’s capillary method & also by Lee & White’s method where venous also by Lee & White’s method where venous blood is taken in a test tube. Every half minute blood is taken in a test tube. Every half minute the test tube is tilted at 45the test tube is tilted at 45° & the time when ° & the time when blood clots is noted.blood clots is noted.
Normal values: 3 – 8 min.Normal values: 3 – 8 min. SignificanceSignificance::
C.T. increases in haemophilia.C.T. increases in haemophilia.

5151
Bleeding timeBleeding time : :
It is the time required by the cut surface to stop It is the time required by the cut surface to stop bleeding.bleeding.
Normal valueNormal value : 1 – 3 min. : 1 – 3 min.SignificanceSignificance: :
It increases in purpura but remains normal in It increases in purpura but remains normal in haemophilia.haemophilia.

5252
How is platelet function assessed & what drug most How is platelet function assessed & what drug most commonly affects the test?commonly affects the test?
Bleeding time is a screening test that assesses Bleeding time is a screening test that assesses platelet no. & function. It is increased by platelet count platelet no. & function. It is increased by platelet count less than 100,000 & by presence of aspirin, antibiotics less than 100,000 & by presence of aspirin, antibiotics (synthetic penicillins), uremia, alcoholism, chronic liver (synthetic penicillins), uremia, alcoholism, chronic liver disease, Ehler- Danlos syndrome & Von – willebrand disease, Ehler- Danlos syndrome & Von – willebrand disease.disease.
Aspirin irreversibly blocks cyclooxygenase function, Aspirin irreversibly blocks cyclooxygenase function, inhibiting platelet aggregation for their 7 – 10 day life inhibiting platelet aggregation for their 7 – 10 day life span because approx. 10 % of platelets are replaced span because approx. 10 % of platelets are replaced each day, it takes an average of 2 -3 days for B.T. to each day, it takes an average of 2 -3 days for B.T. to normalize, but most experts recommend allowing 7 normalize, but most experts recommend allowing 7 days without aspirin prior to surgery.days without aspirin prior to surgery.
Other NSAIDS will alter platelet function only Other NSAIDS will alter platelet function only temporarily, usually less than 24 hrs.temporarily, usually less than 24 hrs.

5353
Tests monitoring Clotting systemTests monitoring Clotting system::
Prothrombin time Prothrombin time ::
PT is normally 11.5 – 13.5 seconds but requires PT is normally 11.5 – 13.5 seconds but requires separate control per reagent.separate control per reagent.
It measures the function of clotting factors 1,2,5,7,10.It measures the function of clotting factors 1,2,5,7,10.
It is increased by warfarin, vitamin K deficiency, Fat It is increased by warfarin, vitamin K deficiency, Fat malabsorption, Liver disease, D.I.C , & artificially malabsorption, Liver disease, D.I.C , & artificially increased torniquet time. Warfarin blocks vitamin K use, increased torniquet time. Warfarin blocks vitamin K use, While broad spectrum antibiotics elevate PT by killing While broad spectrum antibiotics elevate PT by killing normal bowel flora, which decreases vitamin K normal bowel flora, which decreases vitamin K absorption. Heparin in high doses will increase PT by absorption. Heparin in high doses will increase PT by altering factor X. In dental extractions, few bleeding altering factor X. In dental extractions, few bleeding effects are seen with PT effects are seen with PT ≤ 2.5.≤ 2.5.
Fresh frozen plasma will reverse warfarin effects Fresh frozen plasma will reverse warfarin effects immediately, while vitamin K requires 12 – 24 hrs to immediately, while vitamin K requires 12 – 24 hrs to decrease PT.decrease PT.

5454
Activated partial thromboplastin time (APTT)Activated partial thromboplastin time (APTT) : : (27 – 38 seconds)(27 – 38 seconds) This test monitors the function of factors This test monitors the function of factors
I,II,V,VIII,IX,X,XI,XII. APTT is increased by heparin, I,II,V,VIII,IX,X,XI,XII. APTT is increased by heparin, clotting factor deficiency, haemophilia A, haemophilia B, clotting factor deficiency, haemophilia A, haemophilia B, increased torniquet time & partially warfarin. Heparin’s increased torniquet time & partially warfarin. Heparin’s primary effect is to activate antithrombin III, which blocks primary effect is to activate antithrombin III, which blocks coagulation by inhibiting mostly IX & X factorscoagulation by inhibiting mostly IX & X factors
Antithrombin III amounts are significantly decreased in Antithrombin III amounts are significantly decreased in severe malignancy, liver disease, nephrotic syndrome , severe malignancy, liver disease, nephrotic syndrome , Deep venous thrombosis, Septicemia, major surgery , Deep venous thrombosis, Septicemia, major surgery , malnutrition & DIC.malnutrition & DIC.
Low molecular weight heparin also works on Low molecular weight heparin also works on antithrombin III.antithrombin III.
Heparin’s peak effect is at 30 min. to 1 hr after i.v.use & Heparin’s peak effect is at 30 min. to 1 hr after i.v.use & 3 – 4 hrs after s.c. dose. Its duration of effect is 3 – 4 hrs after s.c. dose. Its duration of effect is approximately 3 – 4 hrs when given I.V. & 6 hrs approximately 3 – 4 hrs when given I.V. & 6 hrs subcutaneously.subcutaneously.

5555
RENAL FUNCTION TESTSRENAL FUNCTION TESTS – – They are broadly grouped as under:They are broadly grouped as under:1. Tests to measure glomerular filtration rate.1. Tests to measure glomerular filtration rate.2. Test to measure tubular function2. Test to measure tubular function3. Test to measure renal blood flow & effective 3. Test to measure renal blood flow & effective
renal plasma flow. renal plasma flow. a)a) Tests of glomerular filtrationTests of glomerular filtration : : Three clearance tests – inulin , urea & creatinine often are Three clearance tests – inulin , urea & creatinine often are
used to examine for impairment of glomerular filtration.used to examine for impairment of glomerular filtration.1.1. Inulin a polysaccharide is the ideal exogenous substance Inulin a polysaccharide is the ideal exogenous substance
because it is neither reabsorbed nor secreted by renal tubule because it is neither reabsorbed nor secreted by renal tubule but it is not routinely used in clinical setting because of but it is not routinely used in clinical setting because of necessity for continuous intravenous infusion.necessity for continuous intravenous infusion.
2.2. Determination of urea clearanceDetermination of urea clearance:: Principle: The urea clearance is calculated upon the basis of Principle: The urea clearance is calculated upon the basis of
blood urea concentration, urine urea concentration & rate of blood urea concentration, urine urea concentration & rate of urine excretion.urine excretion.

5656
CalculationCalculation : :
a)a) If per minute excretion of urine is 2ml or more, use If per minute excretion of urine is 2ml or more, use the formula:the formula:
U/B x V = Cm (Maximum clearance)U/B x V = Cm (Maximum clearance)
b)b) If the per minute excretion of urine is under 2 ml, If the per minute excretion of urine is under 2 ml, use the formula:use the formula:
U/B x V = Cs ( Standard clearance )U/B x V = Cs ( Standard clearance )
U = Urine urea mg percentU = Urine urea mg percent
B = Blood urea mg percentB = Blood urea mg percent
V = Volume of urine excreted as ml per minutes.V = Volume of urine excreted as ml per minutes.
Cm/75 x 100 or Cs/54 x 100 = percent of normal Cm/75 x 100 or Cs/54 x 100 = percent of normal clearance .clearance .

5757
Creatinine clearance testCreatinine clearance test : :
Creatinine is formed relatively at a constant Creatinine is formed relatively at a constant rate by muscle from phosphate. Creatinine is rate by muscle from phosphate. Creatinine is useful for measuring the glomerular filtration useful for measuring the glomerular filtration rate as little is transferred across tubular cells.rate as little is transferred across tubular cells.
CalculationCalculation : :
Ccreatinine = U/P x VCcreatinine = U/P x V
U = Urine creatinine concentration in gm/ litre.U = Urine creatinine concentration in gm/ litre.
p = Serum creatinine concentration mg percentp = Serum creatinine concentration mg percent
V = 24 hr urine volume in ml.V = 24 hr urine volume in ml.
The average normal 24 hr endogenous The average normal 24 hr endogenous creatinine clearance is 170 litres.creatinine clearance is 170 litres.

5858
Normal rangeNormal range : : Males: 107 - 139 ml/min.Males: 107 - 139 ml/min. Female : 87 – 107 ml/min.Female : 87 – 107 ml/min. Causes for reduced creatinine clearance:Causes for reduced creatinine clearance:a)a) Acute :Acute : ShockShock HypovolemiaHypovolemia Nephrotoxic chemicals acute glomerulonephritisNephrotoxic chemicals acute glomerulonephritis Malignant hypertensionMalignant hypertension EclampsiaEclampsiab)b) Chronic :Chronic : GlomerulonephritisGlomerulonephritis PyelonephritisPyelonephritis Hypertensive NephrosclerosisHypertensive Nephrosclerosis Polycystic kidneys.Polycystic kidneys.

5959
Glomerular filtration rateGlomerular filtration rate : : Inulin, a polysaccharide is eliminated exclusively Inulin, a polysaccharide is eliminated exclusively
through the glomeruli is neither excreted nor through the glomeruli is neither excreted nor absorbed by the tubules. Inulin clearance is absorbed by the tubules. Inulin clearance is therefore a measure of G.F.R.therefore a measure of G.F.R.
Normal range in adults is :Normal range in adults is : Males : 97 – 137 ml/min./1.73 sq.m of body Males : 97 – 137 ml/min./1.73 sq.m of body
surface.surface. Females: 88 – 128 ml/min./1.73 sq. m. of body Females: 88 – 128 ml/min./1.73 sq. m. of body
surface.surface.B) B) Tubular function testsTubular function tests : : These are concentration & dilution tests, which These are concentration & dilution tests, which
measure the ability of tubules to concentrate measure the ability of tubules to concentrate or dilute the urine, under conditions of water or dilute the urine, under conditions of water depriviation or water loading respectively. depriviation or water loading respectively.

6060
a)a) Dilution test Dilution test ::
The test is done in the morning after a 12 hr fast. The The test is done in the morning after a 12 hr fast. The patient is made to empty the bladder & then he drinks patient is made to empty the bladder & then he drinks 1200 ml water in half an hour. Thereafter bladder is 1200 ml water in half an hour. Thereafter bladder is emptied every hr for 4 hrs. The total volume of urine emptied every hr for 4 hrs. The total volume of urine excreted in 4 hrs should be 80 – 120 % of water excreted in 4 hrs should be 80 – 120 % of water ingested & in atleast one of the four samples the ingested & in atleast one of the four samples the specific gravity should be 1.003 or lower.specific gravity should be 1.003 or lower.
Concentration testConcentration test ::
All fluids are restricted after breakast untill the All fluids are restricted after breakast untill the following morning, the usual diet is allowed omitting following morning, the usual diet is allowed omitting foods containing free fluid. On retiring patient empties foods containing free fluid. On retiring patient empties the bladder & the sample saved. Two additional the bladder & the sample saved. Two additional samples are collected at hourly intervals. Atleast in one samples are collected at hourly intervals. Atleast in one of the three samples the specific gravity should be of the three samples the specific gravity should be 1.025 or higher. The test is contraindicated in old 1.025 or higher. The test is contraindicated in old persons,in patients with heart disease or renal failure.persons,in patients with heart disease or renal failure.

Serum creatinineSerum creatinine:: Creatinine is important in muscle metabolism in Creatinine is important in muscle metabolism in
that it provides storage of high energy of that it provides storage of high energy of phosphate. The body content of creatinine is phosphate. The body content of creatinine is proportional to muscle mass.proportional to muscle mass.
Creatinine is anhydride product of creatine & is Creatinine is anhydride product of creatine & is produced at a reasonably constant rate. Creatinine produced at a reasonably constant rate. Creatinine is freely filtered by glomeruli which gives estimation is freely filtered by glomeruli which gives estimation to serum creatinine an ideal R.F.T.to serum creatinine an ideal R.F.T.
Normal valuesNormal values::
0.6 – 1.2 mg/dl for males0.6 – 1.2 mg/dl for males
0.5 – 1 mg/dl for females 0.5 – 1 mg/dl for females
6161

Blood Urea Nitrogen Blood Urea Nitrogen :: Urea is the major end product of protein & amino Urea is the major end product of protein & amino
acid catabolism & is formed by urea cycle. Most acid catabolism & is formed by urea cycle. Most of the urea is excreted by kidneys. Urea is freely of the urea is excreted by kidneys. Urea is freely filtered by glomeruli & depending upon state of filtered by glomeruli & depending upon state of hydration 40 – 80 % of urea is reabsorbed in hydration 40 – 80 % of urea is reabsorbed in proximal tubule. So blood urea concentration proximal tubule. So blood urea concentration depends upon the state of hydration.depends upon the state of hydration.
Normal value: Normal value:
20 – 35 mg/dl20 – 35 mg/dl
Values in normal person varies depending upon Values in normal person varies depending upon the protein intake & state of protein intake. Low the protein intake & state of protein intake. Low hydration increases value inspite of normal renal hydration increases value inspite of normal renal function.function. 6262

AzotemiaAzotemia is a biochemical abnormality referring is a biochemical abnormality referring to increase in plasma concentration of blood to increase in plasma concentration of blood urea.When it produce symptom it is called urea.When it produce symptom it is called uremia.uremia.
Causes of azotemia are Causes of azotemia are ::
1.1. Prerenal Prerenal
2.2. RenalRenal
3.3. PostrenalPostrenal Pre renal azotemia is caused by CCF,ShockPre renal azotemia is caused by CCF,Shock Renal azotemia is caused by acute or chronic Renal azotemia is caused by acute or chronic
renal dysfunction or glomerulonephritis.renal dysfunction or glomerulonephritis. Post renal azotemia is caused by urinary Post renal azotemia is caused by urinary
obstruction of kidneys like tumor, renal or obstruction of kidneys like tumor, renal or bladder stone etc.bladder stone etc. 6363

Renal biopsyRenal biopsy::
Needle biopsy of kidneys has been Needle biopsy of kidneys has been introduced recently. The tissue bit introduced recently. The tissue bit removed is submitted for histological removed is submitted for histological examination. If positive, it gives the exact examination. If positive, it gives the exact information of the nature of the lesion.information of the nature of the lesion.
6464

Blood glucose estimationBlood glucose estimation:: Fasting blood glucoseFasting blood glucose::
Glucose estimation is done in the blood sample collected in Glucose estimation is done in the blood sample collected in the fluoride bulb to avoid glycolysis. F.B.S. values > 120 mg the fluoride bulb to avoid glycolysis. F.B.S. values > 120 mg per 100ml are indicative of diabetes mellitus.per 100ml are indicative of diabetes mellitus.
Values between 110 – 120 mg per 100 ml are equivocal & Values between 110 – 120 mg per 100 ml are equivocal & should be confirmed by standard tolerance test.should be confirmed by standard tolerance test.
b)b) Two hour post prandial blood glucose estimationTwo hour post prandial blood glucose estimation::
After an overnight fast ( 12 hrs ) the patient is given in After an overnight fast ( 12 hrs ) the patient is given in breakfast 100 gm of carbohydrate. Two hrs later a single breakfast 100 gm of carbohydrate. Two hrs later a single sample of blood is withdrawn.sample of blood is withdrawn.
Blood glucose level of 120 mg is suspicious & levels in Blood glucose level of 120 mg is suspicious & levels in excess of 140 mg are diagnostic.excess of 140 mg are diagnostic.
c)c) Confirmatory test for diabetes mellitus :Confirmatory test for diabetes mellitus : Oral glucose tolerance test :Oral glucose tolerance test :
6565

Oral glucose tolerance testOral glucose tolerance test::
This test is used for confirmation of suspicious mild This test is used for confirmation of suspicious mild cases of diabetes mellitus. An ordinary mixed diet is cases of diabetes mellitus. An ordinary mixed diet is taken for atleast a week before doing the test. The test is taken for atleast a week before doing the test. The test is usually carried out in the morning after a night’s fast but usually carried out in the morning after a night’s fast but if necessary, it may be done five hrs after the last food if necessary, it may be done five hrs after the last food was taken.was taken.
Blood is taken for the determination of the F.B.S. & a Blood is taken for the determination of the F.B.S. & a specimen of urine is collected. 75 gm of glucose specimen of urine is collected. 75 gm of glucose dissolved in about 150 – 200 ml of water is then given. dissolved in about 150 – 200 ml of water is then given. Blood for estimation of blood sugar is taken at ½ hrly Blood for estimation of blood sugar is taken at ½ hrly intervals for 2 ½ hr after the glucose has been intervals for 2 ½ hr after the glucose has been administered. Urine samples are collected at intervals to administered. Urine samples are collected at intervals to check for glycosuria. check for glycosuria.
6666

Time Fasting ½ hr 1 hr 2 hrs 2 ½ hrs
Blood sugar(mg%)
70 - 110 30 – 60AboveFasting level
20 -50Above fasting level
5 -15Above fasting level
Fasting level or below
Urine sugar Absent through out the test
6767
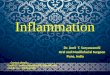
Normal Glucose tolerance curve :

6868
Diminished glucose tolerance
Increased Glucose tolerance
Lag tolerance curve
Diabetes mellitus, Hyperactivity of Thyroid,Injection of ACTH,Severe disease of Pancreas & liver
Hypothyroidism,Hypoadrenalism, Hypopituitarism, Coeliac disease, Sprue , Idiopathic Steatorrhoea.
Impaired absorption of carbohydrate is the cause.
Greater rise in blood sugar is due to delay in insulin mechanism coming into action.This type of curve is termed Lag curve. It is more probably due to an increased rate of absorption of glucose from the intestine, following rapid emptying of stomach.This condition is harmless & not likely to develop into diabetes later.
Abnormal Glucose curve :

What tests are used as marker for liver function?What tests are used as marker for liver function?
Serum albumin, total protein, bilirubin, SGOT, Serum albumin, total protein, bilirubin, SGOT, SGPT, alkaline phosphatase ( ALP ) , SGPT, alkaline phosphatase ( ALP ) , Gamma glutamyl transferase(GGT) , Lactate Gamma glutamyl transferase(GGT) , Lactate dehydrogenase(LDH), PT, bile acids, & blood dehydrogenase(LDH), PT, bile acids, & blood ammonia.ammonia.
6969

Liver function tests Liver function tests ::
a)a) Serum Bilirubin Serum Bilirubin ::
Bilirubin is formed in the cells of R.E. Bilirubin is formed in the cells of R.E. system as the breakdown product of system as the breakdown product of haemoglobin. Bilirubin formed is transported haemoglobin. Bilirubin formed is transported via blood to liver cells.via blood to liver cells.
Normal value: 0.1 - 1.2 mg/dlNormal value: 0.1 - 1.2 mg/dl Increased in JaundiceIncreased in JaundiceSubstance like carotene, vitamin B complex Substance like carotene, vitamin B complex
also affects the result of investigation by also affects the result of investigation by giving false reaction. giving false reaction.
7070

b) b) Tests based on Enzyme activityTests based on Enzyme activity:: Transaminases are the enzymes which participate in transamination Transaminases are the enzymes which participate in transamination
i.e. transfer of amino acids from L-amino acid to the L- keto acid. i.e. transfer of amino acids from L-amino acid to the L- keto acid. Examples are serum glutamic oxaloacetic transaminase ( S.G.O.T) Examples are serum glutamic oxaloacetic transaminase ( S.G.O.T) & serum glutamic pyruvic transaminase ( S.G.P.T.). Liver is rich in & serum glutamic pyruvic transaminase ( S.G.P.T.). Liver is rich in S.G.O.T & S.G.P.T. They are present in the parenchymatous cells of S.G.O.T & S.G.P.T. They are present in the parenchymatous cells of other organs like myocardium, skeletal muscles & brain.other organs like myocardium, skeletal muscles & brain.
When there is necrosis of these cells, S.G.O.T level in blood rises. When there is necrosis of these cells, S.G.O.T level in blood rises. In liver cell damage , S.G.PT. is more helpful than S.G.O.T level.In liver cell damage , S.G.PT. is more helpful than S.G.O.T level.
Normal values: Normal values:
S.G.O.T. : 8 – 33 unitsS.G.O.T. : 8 – 33 units
S.G.P.T. : 4 – 36 unitsS.G.P.T. : 4 – 36 units
Transaminase activity in serum parallels the degree of liver cell Transaminase activity in serum parallels the degree of liver cell damage, the level rises with damage & declines on recovery. In this damage, the level rises with damage & declines on recovery. In this respect the test is very sensitive & helps as evidence of response respect the test is very sensitive & helps as evidence of response to treatment. In hepatocellular disease as in infective hepatitis it to treatment. In hepatocellular disease as in infective hepatitis it may rise markedly while it may show moderate rise in may rise markedly while it may show moderate rise in obstructive jaundice where hepatic damage is produced obstructive jaundice where hepatic damage is produced considerably. considerably. 7171

Serum alkaline phosphataseSerum alkaline phosphatase::
Bones are the most important site of the Bones are the most important site of the production of this enzyme in the body.production of this enzyme in the body.
Normal value : 3 – 13 K.A.Normal value : 3 – 13 K.A.
In obstructive jaundice there is marked elevation In obstructive jaundice there is marked elevation in serum alkaline phosphatase level ( above 30 in serum alkaline phosphatase level ( above 30 K units )K units )
Increased in conditions Increased in conditions ::
Infective hepatitis, Metastatic carcinomaInfective hepatitis, Metastatic carcinoma
Rickets, osteomalacia , Pagets diseaseRickets, osteomalacia , Pagets disease
Osteogenic sarcoma, HyperparathyroidismOsteogenic sarcoma, Hyperparathyroidism
Healing of fracture, children with growing bones.Healing of fracture, children with growing bones.
7272

What is the clinical significance of liver enzymes?What is the clinical significance of liver enzymes? Any increase of hepatic enzymes indicates cellular Any increase of hepatic enzymes indicates cellular
damage. Increased specificity for liver damage damage. Increased specificity for liver damage occurs with elevation of ALT, GGT, or 5’ nucleotidase occurs with elevation of ALT, GGT, or 5’ nucleotidase level. level.
7373

Tests based on coagulation Tests based on coagulation ::
1.1. Clotting timeClotting time
2.2. Bleeding timeBleeding time
3.3. Fibrinogen in bloodFibrinogen in blood
The process of coagulation depends The process of coagulation depends upon many substances which are upon many substances which are synthesized in liver . In liver damage synthesized in liver . In liver damage therefore their synthesis is increased & therefore their synthesis is increased & there is hypofibrinogenemias.there is hypofibrinogenemias.
7474

Bromosulphophthalein retention Bromosulphophthalein retention testtest
The dye bromosulphophthalein after intravenous The dye bromosulphophthalein after intravenous injection is removed from blood by the liver parenchyma injection is removed from blood by the liver parenchyma cells & kupffer cells & is excreted in bile. The dye 5 cells & kupffer cells & is excreted in bile. The dye 5 mg/kg body weight is injected & blood samples are mg/kg body weight is injected & blood samples are withdrawn after 45 min. In about 80 % of cases of withdrawn after 45 min. In about 80 % of cases of infective hepatitis in preicteric phase with mild damage, infective hepatitis in preicteric phase with mild damage, the retention of dye is 50 – 80 % & with severe damage the retention of dye is 50 – 80 % & with severe damage the retention is above 80%.the retention is above 80%.
The limitation of the test is the difficulty of estimation of The limitation of the test is the difficulty of estimation of dye in jaundiced patients with elevated bilirubin.dye in jaundiced patients with elevated bilirubin.
7575

What are the causes of bilirubin abnormalities ?What are the causes of bilirubin abnormalities ?
Bilirubin is produced by the breakdown of Hb in Bilirubin is produced by the breakdown of Hb in the R.E. system. This newly formed bilirubin the R.E. system. This newly formed bilirubin circulates through the blood stream bound to circulates through the blood stream bound to albumin. Liver cells extract the bilirubin & albumin. Liver cells extract the bilirubin & conjugate it to a water soluble pigment that is conjugate it to a water soluble pigment that is excreted in bile. Elevations of the total bilirubin excreted in bile. Elevations of the total bilirubin in the blood cause jaundice ( yellowing of skin & in the blood cause jaundice ( yellowing of skin & sclera, & pruritis ) & may be due to bile sclera, & pruritis ) & may be due to bile obstruction or excessive hemolysis.Elevation of obstruction or excessive hemolysis.Elevation of indirect bilirubin occurs with obstruction & indirect bilirubin occurs with obstruction & hepatocellular disease, & hemolytic anemia & hepatocellular disease, & hemolytic anemia & physiological in newborns. The direct bilirubin physiological in newborns. The direct bilirubin increases primarily with obstruction to bile flow & increases primarily with obstruction to bile flow & is associated with an increase in ALP.is associated with an increase in ALP.
7676

Blood Groups:Antigen & antibody present in ABO group:

If agglutination occurs with antiserum A Blood group is A.
If agglutination occurs with antiserum B Blood group is B.
If agglutination occurs with both antisera A & B Blood group is AB.
If agglutination doesn’t occur with antiserum A or B
Blood group is O.
Results:

Cross matching:For blood typing, RBC of the individual
(recipient) & test sera are used.Cross matching is done by mixing the
serum of recipient & RBCs of donor. In clinics, Cross matching is always done before blood transfusion. If agglutination of RBCs from a donor occurs during Cross matching, the blood from that person is not used for Transfusion.

Inheritance of Rh antigen :

Sodium (Na)Sodium is primarily responsible for maintaining osmotic pressure. In other words, it maintains intracellular and extracellular fluid levels in the body. An increased serum sodium is present in states of dehydration as a result of diarrhea or vomiting. Low sodium levels usually are a result of too much water in the body.Normal values: 135 - 145 Meq/L
Blood investigations:
Serum Electrolytes:

Potassium (K)Potassium is a major component in cardiac function. Even small changes in Potassium can cause abnormal cardiac arrhythmias, affecting cardiac function. Too much potassium in the blood is usually caused by poor kidney function and can cause abnormal and sometimes fatal abnormalities in the heart rhythm. Low potassium levels are usually the result of potassium loss from excessive urination or from vomiting. A potassium level that is too low can cause abnormal heart rhythms.Normal values: 3.5 - 5.0 mEQ/L

Chloride (Cl)In combination with sodium, chloride maintains fluid levels by regulating osmotic pressure in the blood. An elevated chloride usually results from abnormal kidney function. A chloride level below normal usually results from excessive vomiting or diarrhea.Normal values: 100 - 106

Serum calciumAll cells require calcium to function.
Calcium is especially important in the structure of bones and in neuromuscular (nerves and muscles) activity. A deficiency of calcium in the body fluids causes hyperexcitable nerves and muscles. Excess calcium has the opposite effect.
Normal values range from 9 to 11 mg/dL.

Serum phosphorus
The serum phosphorus test measures the amount of phosphate in the blood.
Most of the body's phosphorus is combined with calcium in the bones, but about 15% exists -- as phosphate (PO4) ions -- in the blood and other soft tissues and body fluids. Dietary phosphorus is efficiently absorbed, so a low PO4 level caused by dietary deficiency is unlikely in those on a normal diet unless the person has a malabsorption syndrome (inadequate absorption of nutrients in the intestinal tract.

Thank youThank you
8686