- 1.Types of dementia, Pathphysiology of Alzheimers disease, New
diagnostic criteria and guidelines for Alzheimersdisease, Current
and future psychopharmacological interventions in Alzheimers
disease.
2. Dementia a growing epidemic In 2012 -5.4 million Americans
have dementia of allcauses. In 2050- it is estimated that 15
million Americans willlive with dementia. Every 68 seconds someone
in America developsdementia. It is estimated that nearly 500,000
new cases will bediagnosed this year alone. Worldwide 36 million
people are believed to live withdementia. By 2050, if breakthroughs
are notdiscovered, the rates could exceed 115 million. 3.
DefinitionDementia consists of: memory impairment (amnesia),
deficits in either language (aphasia), or motor function (apraxia),
recognition (agnosia), or executive function, such as working
memory andproblem solving. personality changes can also be present
(sometimeseven before the memory impairment) 4. Not Every Memory
Disturbance IsDementia Age-related memory-impairment (ARMI) Self
perceived memory loss Over age 65 prevalence around 40% = 16
million in US About 1% of which eventually develop dementia Minor
Cognitive Impairment (MCI) More severe memory loss, little/no
functional impairment Around 10% over 65 does not necessarily
develop to AD Alzheimers Disease (AD) Around 15% of those with MCI
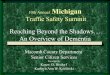
convert 5. Not All Dementias are AlzheimersDisease 6. Mixed
Dementias It is possible to have more than one dementia, and in
fact many patients haveboth Alzheimers disease and either dementia
with Lewy bodies or vasculardementia. 7. Pathology of Alzheimers
DementiaIn order for a dementia to be called Alzhheimers diseaseit
has to present with both: AMYLOID PATHOLOGY - Beta amyloid plaques
(extracellular) TAU PROTEIN PATHOLOGY - Neurofibrillary tangles
(abnormal phosphorylation of tau proteins) (intracellular) 8.
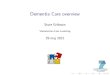
Amyloid Plaques 9. NORMAL PATHWAY: Processing of AmyloidPrecursor
Protein into Soluble Peptides 10. ABNORMAL PATHWAY: Processing
ofAmyloid Precursor Protein into A betaPeptides 11. Beta Secretase
Inhibitors Merck: MK-8931 Lilly: LY450139 12. Gamma Secretase
Inhibitors Merck: MK-8931 Eisai: E 2609 Lilly: LY2886721 13.
Monoclonal Antibodies againstAbeta 42 *Solanezumab (Lilly)
*Bepaneuzumaub (Pfizer) 14. AMYVID (Flobetapir)Visualizing Amyloid
Indicated for PET imaging of the brain to estimate the density of
beta amyloid plaques in adult patients with cognitive impairment
who are being evaluated for Alzheimers disease and other causes of
cognitive impairment. 15. Amyloid Cascade Hypothesis, Part One:
increasedproduction of Abeta42 16. Amyloid Cascade Hypothesis, Part
Two: A beta 42Oligomers Form and Interfere with SynapticFunction
17. Amyloid Cascade Hypothesis, Part Three: formation ofamyloid
plaques causing inflammation 18. Amyloid Cascade Hypothesis, Part
Four: amyloid plaqueinduces formation of tangles 19. The Role of
Tau Protein 20. Tau Pathology 21. Amyloid cascade Hypothesis, Part
Five: neuronaldysfunction and loss 22. DIAGNOSIS: 2011 Diagnostic
Criteria for AD(emphasis on prevention) 23. Two kinds of AD:
Familial andIncidental Autosomal dominant, early onset (5-10%)
(mutations in the APP or gamma secretase) CHROMOSOMEGENE1Presenilin
2 14Presenilin 121 Amyloid PPIncidental is non-genetic it does not
run infamilies. 24. Pre-symptomatic Entities1. Pre clinical AD (
recommendations are intended for research purposes).2. MCI (Minor
Cognitive Impairment). 25. More Sensitive Screening 26. Core
clinical criteriaNeuropsychiatric symptoms that: 1.Interfere with
the ability to function 2. Represent a decline from the previous
level of functioning 3. Are not explained by delirium 4. Cognitive
impairment is detected by history taking and objective cognitive
assessment 5. Impairment involves a minimum of two of the following
domains: Impaired ability to acquire and remember new information
Impaired reasoning and handling of complex tasks, poor judgment
Impaired visuospatial abilities Impaired language functioning
Changes in personality or behavior 27. Diagnostic Overview1.
Possible AD dementia2. Probable AD dementia3. Probable or possible
AD dementia withevidence of the AD pathophysiological process. 28.
Incorporation of Biomarkers intoAD Dementia CriteriaBiomarkers may
be useful in three circumstances:1. Investigational studies2.
Clinical trials3. And as optional clinical tools for use where
available and when deemed appropriate by the clinician. 29. CSF:
Decreased A42Amyloid Pathology PET : Amyloid imaging with
AmyvidBiomarkersCSF: Increased total or phosphorylated tauPET:
hypoperfusion Tau Pathology temporoparietal, precuneus MRI: Medial
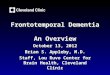
temporal lobeatrophy, Hippocampal atrophy, 30. William Utermohlen
1933-2007 Diagnosed with Alzheimers disease in 1995. 1967 (self
portrait) 31. 1995 32. 1997 33. 1998 34. 1999 35. 2000 36.
Cholinesterase inhibitors offermodest results The usual response to
cholinesterase inhibitor therapy in Alzheimers disease is initial
improvement that is statistically detectable on cognitive testing
and perhaps noticeable to the caregiver but not necessarily to the
patient. Such a response usually lasts about 6 months, at which
point cognitive functioning as measured on cognitive testing is
back to where it was before beginning the drug. 37. Donepezil
(Aricept) Selective inhibitor of AChE, allowing more ACh
toaccumulate Once daily dosing Severe AD Benefits for all outcomes
at 6 months Some indication of positive changes on ADL and severe
impairment battery(SIB) scores More selective for brain than
periphery GI side-effects usually moderate and transient - nausea,
vomiting, diarrhea No liver toxicity Hallucinations twice as common
as placebo . 38. Rivastigmine (Exelon) Inhibits both AChE and the
peripheralbutylcholinesterase (BuChE) May be more selective for
hippocampal AChE May be more useful for late stage AD, when
gliosisincreases BuChE Might interfere with plaque formation
Increased incidence of GI side-effects, especiallyduring dose
optimization/increase 39. Galantamine (Razadyne, previouslyReminyl)
Natural product isolated from daffodils and snowdrops Inhibits
AChE; allosteric modulator of nicotinic receptors;synergistic at
cholinergic synapses Nicotinic action may boost attention and
behaviors causedby deficiencies of other neurotransmitters.
Studies: 16 or 24mg/day, 24 wks, benefits in cognitive and global
function Moderate AD gained more advantage than mild AD BUT may be
higher mortality than with the other AChEs 40. Memantine
(Artificial Magnesium) Voltage-dependent NMDA antagonist that
targetsglutamatergic system Mild side effect profile Dizziness,
confusion, headache, constipation Dosing schedule: Week 1 - 5
mg/day, Week 2 - 5 mg twice a day, Week 3 - 10 mg twice a day, Week
4 - 15 mg twice a day Administered with or without food No PK/PD
interactions with donepezil or other renally-excreted drugs