Embed Size (px)
Citation preview

FIRST TRIMESTER SONOGRAPHY
BY DR DEB KUMAR BISWAS
1ST YEAR RESIDENTDEPT OF
RADIODIAGNOSISMEDICAL
COLLEGE,KOLKATA

BASIC PHYSICS OF SONOGRAPHY

Obstetrical Ultrasound
Introduced in the late 1950’s ultrasonography is a safe, non-invasive, accurate and cost-effective means to investigate the fetus
Computer generated system that uses sound waves integrated through real time scanners placed in contact with a gel medium to the maternal abdomen
The information from different reflections are reconstructed to provide a continuous picture of the moving fetus on the monitor screen

Obstetrical Ultrasound Indications: Unsure last menstrual period Vaginal bleeding during pregnancy Uterine size not equal to expected for dates Use of ovulation-inducing drugs confirm early pregnancy Obstetric complications in a prior pregnancy: ectopic, preterm
delivery Screen for fetal anomaly: abnormal serum screens, certain drug
exposure in early pregnancy, maternal diabetes. Rh isoimmunization
Postdate fetus Twins Intrauterine growth restriction (IUGR)
RADIUS study (1993) did not support routine US screening

PCPNDT RULES IN OBSTERIC SCANNIMG



FIRST TRIMESTER OF PREGNANCY(1 TO 13WKS)GERMINALSTAGE:FROM FERTILIZATION TO 2 WEEKS EMBRYONICSTAGE:FERTILIZATION TO 10 WKS OF GESTATION
FOETAL STAGE:FROM 10 WKS TO DELIVERY

PUPOSE OF FIRST TRIMESTER
SONOGRAPHY>TO VISUALISE IUT GSAC –ITS NUMBER AND IMPLANT SITE
>TO VISUALISE EMBRYO AND FOETUS-NUMBER AND CARDIAC ACTIVITY
>TO ESTIMATE GA-BY MSD CRL BPD>TO EVALUATE THE MORPHOLOGY OF UTERUS AND ADNEXA>TO PROVIDE AND EARLY DIAGNOSIS OF FOETAL ANOMALY
>TO SCREEN FOR ANEUPLOIEDY

TVS VS TAS
TVS TASGSAC 4 WKS 5 DAY 5 WKSYOLK SAC 5 WKS 6 WKSFOETAL POLE 6 WKS 7 WKSFOETAL CARDIAC ACTIVITY
6WKS 7 WKS
BETA HCG 1000 1800

Early Pregnancy Ultrasound report
NORMAL
ABNORMAL
Location Structure Viability Dating Number
• Assessment of other pelvic masses ????• Screening for fetal abnormalities ????• Assisting CVS and amniocentesis????

SONOGRAPHIC APPEARANCE OF
NORMAL IUP

GESTATIONAL SAC 1ST RELIABLE EVIDENCE OF IUP IS VISUALISATION
OF GSAC WITHIN THE THICKENED DECIDUA(INTRADECIDUAL SIGN)
A SMALL ROUND FLUID COLLECTION COMPLETELY SURROUNDED BY A ECHO RICH RIM
i.e. ECENTRIC ECHOGENIC RING WITH ANECHOIC CENTRE
LOCATED IN LATARAL POSITION OF UTERINE FUNDUS
THRESHOLD LEVEL :4WK 3 DAYS DISCRIMINATORY LEVEL:5 WKS 2 DAYS DOUBLE DECIDUAL SIGN:OUTER RING IS FORMED
BY ECHOGENIC ENDOMETRIAL LINING.USED TO DIF B/W IUP & PSEUDOSAC OF ECTOPIC PREG
A WELL DEFINED DOUBLE DECIDUAL SIGN IS MORE ACCURATE PREDICTOR OF IUP
A VAGUE /ABSENT DOUBLE DECIDUAL SIGN-PSEUDOSAC OF ECTOPIC
NOT 100% SPECIFIC FOR IUP

Confirming intrauterine gestation
1) Double decidual sac sign
3) Double bleb sign2) Intradecidual sign

GSAC CONTD
IT GROWS @ 1MM/DAY DISCRIMINATORY ZONE: SERUM HCG LEVEL @
WHICH GSAC IS VISUALISED BY TVS: >2000 Miu/mi TAS:>6000 Miu/ml

YOLK SAC
>1ST STRACTURE TO BE SEEN WITHIN GSAC
• IT APPEARS AS A BRIGHT RING WITH ANECHOIC CENTRE LOCATED WITHIN GSAC
>DIAGNOSTIC OF IUP
>BY TVS:EARLY VISUALISATION POSSIBLE@5WKS & SHOULD ALWAYS BE VISUALISED WITH MSD OF 8MM
>NO OF YOLK SAC DETERMINE THE AMNIOCITY IN MFP

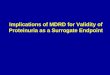
AMNION: double bleb sign
The earliest demonstration of the amnion To bleb :amnion & chorion visualised@ 5.5wks (CRL:2MM)

DOUBLE BLEB SIGN A Double Bleb Sign is a
sonographic feature where there is visualization of a gestational sac containing a yolk sac and amniotic sac giving an appearance of two small bubbles.
The embryonic disc is located between the two bubbles.
It is an important feature of an intrauterine pregnancy and thus distinguishes a pregnancy form a pseudogestational sac or decidual cast cyst.
It should not be confused with the double decidual sac sign.
Yolk sac
Embryonc Disc
Amniotic sac

EMBRYO
>CAN BE VISUALISED IN GSAC AS SMALL AS 10m>GROSS FOETAL ANOMALIES DETECTED:IN LATE 1ST TRIMESTER MAINLY BY TVSDISCRIMINATORY SIZETAS TVS17 TO 30 mm 9 TO 18 mm

CARDIAC ACTIVITY
BEGINS @ 37 DAYS FROM LMP UPTO 10 WKS :B MODE & M MODE USED FOR SAFETY PUISE/COLOUR DOPPLER SHOLD BE
USED AFTER 10 WKS
TVS TAS>HR DETECT 6WKS 7WKS>MSD 13 TO 18 mm 25 mm>length EL 4 TO 5 mm CRL 8 TO 10
mmNORMAL HR: @ 6 WK:90 TO 110 @9 WK:140 TO 170>@ 5 TO 8 WKS FOETAL BRADYCARDIA(<90):a/w HIGH RISK OF MISCARRIAGE

PLACENTA Determining its upper and lower edges r/o
placenta previa With increasing gestational age, the
placenta increases in echogenicity because of increased fibrosis and calcium content.
This feature of placental maturation has led to a grading of placentas from immature (grade 0) to mature (grade 3).
Placentolmegaly Diabetes, fetal hydrops, Rh
isoimmunization
Small placenta: Severe IUGR (symmetrical/asymmetrical)
Grade 0
Grade 1
Grade 3

ABNORMAL PLACENTAPlacenta Previa found in approximately 5%
of second-trimester scans If detected at 15–19 weeks,
it persists in 12% of patients.
If it is detected at 24–27 weeks, it may persist in up to 50%.
Vasa Previa: membranous insertion of cord where exposed vessels cross internal os

05/03/202323
Early dating of pregnancy
5 – 9 weeks : use of mean GS diameter
6 – 12 weeks : use of CRL (most accurate dating of early pregnancy)
After 12 weeks : use of BPD

MEAN SAC DIAMETER CAN BE MEASURED FROM 5-6 TO 11 WKS SHOULD NOT BE USED IF EMBRAYO CAN BE
ASSESSED PROCEDURE:AVG OF 3 ORTHOGONAL INTERNAL
DIAM. MEASURED >AP >LONGITUDINAL >TRANSVERSE GA(IN DAYS)=MSD(MM)+30

CROWN RUMP LENGTH
TVS:EMBRYO REACHES 2 TO 5 mm(5 to 6 wks of MA)
TAS:EMBRYO LENGTH 5 TO 10 mm (6 to 7 wks of MA)
MAX STRAIGHT LINE LENGTH OF EMBRYO/FETUS OBTAINED ALONG ITS LONGITUDINAL AXIS
ACCURACY:+/- 3TO 4 DAYS INACCURATE: TOWARDS THE END OF 1ST TRIMES DUE TO RAPID FOETAL DEVELOPMENT FLEXION EXTENSION POSITIONAL CHANGE

MEASUREMENT OF CRL

BIPARIETAL DIAMETER MEASURED AT THE END OF 1ST TRIMES MEASURED IN A TRANSVERSE SECTION OF FOETAL
HEAD WITH BOTH THE THALAMUS AND CAVUM SEPTUM PELLUCIDUM IN MIDLINE
TVS: OUTER TO OUTER TABLE TAS:OUTER TO INNER TABLE ACCURECY:+/- 3 TO 4 DAYS(B/W 12 TO 16 WKS)

TWIN PREGNANCY ZYGOSITY: GENETIC MAKE UP:DNA ANALYSISD CHORIONICITY:NO OF PLACENTA AMNIOCITY:NO OF YOLK SAC
TWIN
MONOZYGOTIC
<4 DAYS DC DA 4 TO 8 DAYS :MC DA
8 TO 12 DAYS:MC MA
>13 DAYS:CONJOINE
D TWIN
POLYZYGOTIC
DC DA


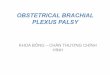
SONOGRAPHY IN TWIN PREGNANCY
DICHORIONIC: THICK INTERTWIN MEMBRANE.TWO LAYER OF AMNION WITH CHORIONIC TISSUE IN BETWEEN.
THICK SEPTUM IS PRESENT B/W TWO GSAC WHICH APPEARS AT THE BASE AS A TRI ANGULAR TISSUE PROJECTION (LAMDA SIGN) LAMDA SIGN READILY VISIBLE IN LATE 1ST
TRIMESTER BUT BECOMES PROGRESIVELY DIFFICULT TO VISUALISE AS GESTATION PROGRESS

MONOCHORIONIC TWIN
ONLY AMNION NO CHORIONIC TISSUE IN INTERTWIN MEMBRANE WHICH IS THIN
T SIGN SEEN

Twin peak (or Lambda sign) pathognomonic for dichorionic placentation
T-sign pathognomonic for monochorionic placentation

Other roles of US Confirm fetal number . Confirm viability. Diagnosis of vanishing twin syndrome. Exclude any malformation or conjoined twins
(especially at age > 35y = genetic amniocentesis)
Needed with other procedures CVS fetal reduction

Abnormal early (first trimester) pregnancy
Failed early pregnancy. Pregnancy of uncertain viability (i.e. IU pregnancy in a situation with no
enough criteria (usually on ultrasound grounds) to confidently categorize a pregnancy
as a miscarriage). Pregnancy of unknown location. Ectopic pregnancy Trophoblastic disease Subchrionic hemorrhage Incomplete abortion (retained products of conception)

Failed early pregnancy
(FEP(
Pregnancy of uncertain viability
(PUV(
No cardiac activity with CRL
≥7mm < 6mm
No fetal pole with MSD
> 25 mm (Anembryonic
Pregnancy)
< 20mm
Others Absence or inadequate growth on serial scans at least 7-10 days
Mean GSD < 25mm and containing yolk sac only
Management Termination Follow up US in 7-14 days with serial beta HCG correlation…viable or nonviable.
TVUS criteria of :

SONOGRPHIC DIAGNOSIS OF
EMBRYONIC DEMISE

EMBRYONIC CARDIAC ACTIVITY
MOST IMPORTANT CRITERIA EMBRYOLOGY:HEART STARTS BEATING @36/37
DSAYS WHEN CRL 1.5 TO 3mm SO WE MAY FIND DIFFICULT TO IDENTIFY CARDIAC
ACTIVITY IN NORMAL EMBRYO WITH CRL<2MM CARDIAC MOTION IS SEEN IN ALL PREGNANCIES
WITH CRL>5mm IN OUR PRACTICE FOLLOW UP SONOGRAPHY IS
PERFORMED IN PT WITH EMBRYO <5mm CRL WITH NO CARDIAC ACTIVITY UNLESS YOLK SAC IS ABSENT

GESTATIONAL SAC FEATURES USED WHEN DIAGNOSIS OF PREGNANCY FAILURE CANT
BE MADE ON THE BASIS OF ABNORMAL CARDIAC ACTIVITY
MOST IMPORTANT OF ALL THIS IS SAC SIZE FOR EARLY PREGNANCY FAILURE ABNORMAL SAC SIZE
DEFINED AS BY TAS:MSD OF 20mm or MORE WITHOUT A YOLK SAC MSD OF 25 mm OR MORE WITHOUT A EMBRYO BY TVS:MSD OF 8 mm OR MORE WITHOUT A YOLK SAC MSD OF 16mm OR MORE WITHOUT A EMBRYO GROWTH RATE:GROW @ 1.1 mm/DAY GROWTH RATE <0.7 MM/DAY MAY INDICATE EARLY PREGNANCY FAILURE IN PRACTICE GSAC OF 16 mm OR MORE WITHOUT A
EMBRYO IS A STRONG EARLY SIGN OF PREGNANCY FAILURE

AMNION &YOLK SAC CRITERIA
VISUALISATION OF AMNION IN THE ABSENCE OF EMBRYO IN SONGRAPHY AFTER 7 WKS OF GA IS ABNORMAL AND DIAGNOSTIC OF NON VIABLE PREGNANCY

SONOGRAPHIC PREDICTOR OF ABNORMAL
OUTCOME

EMBRYONIC BRADYCARDIA
IN A STUDY IT WAS FOUND THAT A HEART RATE <80 BEATS PER MIN IN EMBRYO WITH CRL LESS THAN 5mm IS UNIVERSALLY A/W SUBSEQUENT EMBRYONIC DEMISE
ARRYTHMIA IS ALSO A INDICATOR OF FIRST TRIMESTER LOSS

MSD-CRL
MSD LESS THAN 5mm GREATER THAN CRL i.e (MSD – CRL =< 5mm) (sometimes termed as EARLY OLIGOHYDRAMNIOS)
IS A/W 1ST TRIMESTER SPONTANEOUS ABORTION LOW POSITION OF G SAC & IRREGULAR GSAC
ALSO A/W ABNORMAL OUTCOME

YOLK SAC SIZE & SHAPE
YOLK SAC MALFORMATION NOTED IN DIABETIC MOTHERS BEFORE 9 WKS
B/W 8 TO 12 WEEKS OF GESTATION YOLK SAC LESS THAN 2 mm IN SIZE IS A/W POOR OUTCOME
A THIN YOLK SAC IS ALSO A/W ABNORMAL OUTCOME
ABNORMALLY LARGE YOLK SAC IS OFTEN THE SONOGRAPHIC INDICATOR OF PATHOLOGY & SUBSEQUENT EMBRYONIC DEMISE

DOPPLER USG ASSESMENT
UTERINE ARTERY RESISTANCE DECREASES PROGRESIVELY AFTER IMPLANTATION
IT INCREASES IN IUGR & ECLAMPSIA CAUSE OF INCREASE RESISTANCE:ABNORMAL
TROPHOBLASTIC INVASION ABNORMAL RI >0.55 MAY BE A/W EARLY
PREGNANCY FAILURE

ECTOPIC PREGNANCY
INCIDENCE:1% OF ALL PREGNANCY RISK FACTOR:• H/O ECOPIC• H/O PID • PREGNANT WOMEN WITH IUCD IN SITU• H/O LAP TUBAL LIGATION• H/O TUBAL MICROSURGERY• IVF

SYMPTOMS OF ECTOPIC PREGNANCY
CLASSIC TRIAD (SEEN IN JUST 50%)• PELVIC PAIN• ABNORMAL VAGINAL BLEEDING FOLLOWING 6 TO
8 WKS AMENORRHOEA• PALPABLE ADNEXAL MASS

SITE OF ECTOPIC PREGNANCY

SONOGRAPHIC EVALUATION OF ECTOPIC
TAS:BEGIN OUR EXAM WITH TAS LOOK FOR LARGE OR COMPLEX MASS THAT MAY
BE OUTSIDE THE RANGE OF TVS PROBE CAN IDENTIFY THE DEGREE OF I/P BLOOD LOSS FLUID SEEN IN HRPM IMPERT A GREATER SENSE
OF URGENCY TO THE SURGEON
TVS:MORE SPECIFIC

Endometrial cavity -A trilaminar endometial pattern seen -pseudogestational sac -decidual cyst may be seen PSEUDOSAC – All pregnancies induce an endometrial decidual
reaction, and sloughing of the decidua can create an intracavitary fluid collection called a pseudosac
Early gestational sac Pseudosac location below the midline echo along the burried into endometium cavity line b/w endometrial layers shape usually round may change,oviod borders double ring single layer color flow high avascular pattern peripheral flow

True vs. pseudo-gestational sac

DECIDUAL CYST It is identified as an anechoic area lying with in the
endometrium but remote from the canal and often at the endometrial-myometrial border.
Adenxa - 15-30% an extrauterine yolk sac or embryo seen
in fallopian tubes confirms tubal pregnancy. - A halo or tubal ring surrounded by a thin
hypoechoic area caused by subserosal edema can be seen.
Rectouterine cul-de-sac Free peritonial fluid with an adnexal mass suggestive of ectopic pregnancy

b) Color Doppler Sonography(TV-CDS):
- Improve the accuracy. -Identify the placental shape (ring- of-fire pattern) and blood flow outside the uterine cavity.
-PERITROPHOBLASTIC FLOW IS OF HIGH VELOCITY LOW RESISTANCE FLOW WITH VERY LOW RI & PI

USG SIGN
1.‘Bagel’ sign – Hyperechoic ring around gestational sac in adnexal region
2. ‘Blob’ sign – Seen as small inconglomerate mass next to ovary with no evidence of sac or embryo.
3. Adnexal sac with fetal pole and cardiac activity is most specific.
4. Corpus luteum is useful guide when looking for EP as present in 85% cases in Ipsilateral ovary.

Hyperechoic ring around gestational sac in adnexal region(BAGEL SIGN)

Ring sign — a hyperechoic ring around an extrauterine gestational sac.

2. β-HCG Assay-
a) Single β-HCG: little value b) Serial β-HCG: is required when result of initial USG is confusing.
- When hCG level < 2000 IU/L doubling time help to predict viable Vs nonviable pregnancy.
-Rise of β-HCG <66% in 48 hrs indicate ectopic pregnancy or nonviable intrauterine pregnancy .
Biochemical pregnancy is applied to those women who have two β-HCG values >10 IU/L

Other types of ectopic
pregnancy

Cervical ectopic pregnancy
GS within the cervix . Abnormally low sac position. Colour Doppler : hypervascular trophoblastic
ring in the cervical region .

Interstitial ectopic pregnancy Eccentric gestational sac: the diagnosis is suggested by
visualization of an intrauterine gestational sac or decidual reaction located high in the fundus, that is surrounded by less than 5 mm of myometrium in all planes.
Interstitial line sign : an echogenic line from the mass to the endometrial echo .

Sonographic features of Caesarean scar ectopic pregnancy (CSEP)
empty uterus
empty cervical canal
GS in the anterior part of
the lower uterine segment
absence of myometrium
between the bladder wall
and the GS

EVALUATION OF EMBRYO First Trimester Screening In 2007, the American College of Ob Gyn endorsed
offering aneuploidy screening to all gravidas Performed between 11 and 13 weeks 6 days (fetal
crown–rump length 42–79 mm). Fetal nuchal translucency and maternal blood, β-hCG
and pregnancy-associated plasma protein A (PAPP-A). This test can detect approximately 60-85% of fetuses
with Down syndrome, with a 5% false positive rate.2 Abnormal screen can increase the risk of genetic,
other aneuploidies and other cardiac anomalies

EVALUATION OF EMBRYO Nuchal translucency: Translucent space between the back of
the neck and the overlying skin The scan is obtained with the fetus in
sagittal section and a neutral position . The fetal head (neither hyperflexed nor
extended, either of which can influence the nuchal translucency thickness).
The fetal image is enlarged to fill 75% of the screen, and the maximum thickness is measured, from leading edge to leading edge. (inner to inner measurement)
It is important to distinguish the nuchal lucency from the underlying amnionic membrane.
> 6 mm considered abnormal

What is Abortion?
• Abortion is described as the expulsion of the products of conception before the embryo or fetus is viable. Any interruption of human pregnancy prior to the 28th week of gestation or the delivery of a fetus weighing less than 500 grams is known as abortion.

Categories of Abortions
These include: 1. Threatened 2. Inevitable 3. Incomplete 4. Complete 5. Septic

Threatened abortion(Features)
1. History Mild vaginal bleeding. No abdominal pain
or mild abdominal3. U/S which is essential for the
diagnosis Showed the presence of fetal heart activity

Inevitable and incomplete abortions(Features)2. Examinations
Poor general condition. The cervix is dilating and products of
conception may be passing trough the os
The uterus may be the correct size for date (inevitable abortion) or small for date (incomplete abortion)
3. U/S Fetal heart activity may or may not present in inevitable abortion or retained products of conception ( RPOC ) in incomplete abortion

RPOC
LARGE ECHOGENIC MASS OF TISSUE FILLING THE ENDOMETRIAL CANAL
SINGLE OR LAGE GROUP OF VESSELS EITHER SUPERFICIALLY ON MYOMETRIUM OR EXTENDING DEEP WITHIN IT
THE HIGH FLOW RATE ( APROX 160 CM/SEC) WITHIN THE VESSELS MAY R AISE HIGH CONCERN ABOUT PERFORMING D&C
SURPRISINGLY NO UNTOWORD BLEEDING SEEN DURING OR AGTER SURGERY

Retained products of conception (incomplete abortion)

Complete abortion(Features)1. History
Heavy vaginal bleeding which has been stopped.
lower abdominal pain which follows the bleeding which has been stopp
2.U/S showed empty uterine cavity or PROP

Missed abortion(Features)1. Most of missed abortions are
diagnosed accidentally during routine U/S in early pregnancy .
In some cases there may be a history of : Episodes of mild vaginal bleeding Regression of early symptoms of pregnancy

Missed abortion(Features)
3. U/S (which is essential for diagnosis ) diagnosed if two ultrasound ( T/V or T/A) at least 7days apart showed an embryo of > 7 weeks gestation ( CRL > 6mm in diameter and gestational sac > 20 mm in diameter ) with no evidence of heart activity .

It is due to an early death and resorption of the embryo with the persistence of the placental tissue
It is diagnosed if two ultrasound ( T/V or T/A) at least 7 days apart showed after 7 weeks of gestation i.e. gestational sac > 20mm , an empty gestational sac with no fetal echoes seen .
It is treated in a similar way to missed abortion .
Anembryonic pregnancy (Blighted ovum)

Anembryonic Pregnancy

MOLAR PREGNANCY
Defined as proliferation and degeneration of the chorion
A benign neoplasm of the chorion
The embryo fails to develop in most cases
Occurs in 1 of 2000 pregnanciesMore often in low socioeconomic
groups with low protein dietsMore often is the younger or
older mother

Symptoms of a Molar Pregnancy
Uterus expands faster and reaches landmarks earlier
More morning sicknessEarlier signs of PIHVaginal bleeding in the 4th monthDischarge with grape-like
vesicles

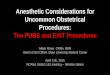
Molar pregnancy ( Snow storm+ Theca-lutein cysts )


Safety of ultrasound in pregnancy
General perception is that ultrasound is safe (It is not ionising radiation)
However, bioeffects can be either thermal or mechanical (i.e. cavitations) with high power ultrasound
One RCT of repeated routine ultrasound with Dopplers in the 3rd trimester found a small but significant decrease in birth weight in the exposed cohort

How to reduce biohazardsALARA
As Low As Reasonably Achievable
ALARA principle: Lowest acoustic power Shortest duration Least exposure to sensitive target tissues

Take home message Ultrasound is no substitute for a good history
ALWAYS do an abdominal scan with ( Full bladder)
before using the vaginal probe with ( Empty bladder)
Avoid premature conclusions

Take home message Systematic scan should be performed
US scans are useful to be combined with HCG tests
before decision.
With ultrasound , an early intervention or
conservative management in pregnancy can be
determined.