Embed Size (px)
Citation preview

Radiosurgery in urological malignancies
Debnarayan Dutta, MDConsultant Radiation Oncologist
Apollo Speciality Hospital, Chennai
INDIA

Apollo Speciality Hospital, Chennai
Cancer management Facilities- Medical, surgical & radiation oncology unit
- 320 slice CT scan
- MRI scan with ‘time of flight’ technology
- Bone marrow transplant unit
- Two LA with 3DCRT, IMRT & IGRT
- HDR brachytherapy
- BrainLAB system
- CyberKnife
- Tumour board
- Multi-disiplinary support system
- 17 yrs experience in radiation therapy
- 8 yrs experience in IMRT
- 10 yrs experience in BrainLAB
‘The Week’ magazine ranking 2010
3rd rank in oncology
(after TMH & AIIMS)

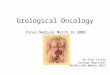
Cyberknife

Accuray Confidential
Linear
Accelerator
Manipulator
Image
Detectors
X-ray Sources
IMAGING
SYSTEM
ROBOTIC
DELIVERY
SYSTEM
TARGETING SOFTWARE

Robotic Radiosurgery
Highly precise RT delivery system
- Respiratory tracking
- Fiducial based tracking system
- Intra-fraction motion correction
- Uncomparable dose distribution
- X-ray based image verification
Hypofractionated RT
- High dose short course RT
- Higher BED delivered to target
Ideal for moving targets

Unique features of Cyberknife:
‘Frameless’ treatment of intra & extra cranial disease
Both intra & extra-ceanial
tumours can be treated

Unique features of Cyberknife:
– Relies on intra-fraction imaging to continually assess target movement
– Stated total clinical accuracy of .50mm
Chang et al.Neurosurgery, 2003
Murphy MJ et al. Int J Radiat Oncol Biol Phys. 2003
Sub-millimeter accuracy

CyberKnifeNovalis / Trilogy
Unique features of Cyberknife:
Unmatched dose distribution
Higher low dose spillage with Novalis.
Better dose conformity with Cyberknife

DRR
LIVE
Unique features of Cyberknife:
‘6-D tracking system’

Unique features of Cyberknife:
‘Fiducial tracking’
Fiducial tracking is the most effective method of tumour tracking

Unique features of Cyberknife:
Non-coplanar field arrangement

Unique features of Cyberknife:
‘Dose painting’ technique
– Highly conformal dose delivery
– Both isocentrically and non-isocentrically
– Non-coplanar beam arrangement
– Flexible fractionation schedule
– Flexible treatment delivery

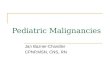
Synchrony respiratory tracking system: Cyberknife

Synchrony respiratory tracking system• Continuously tracks tumor motion during treatment
– Synchrony RespiratoryTracking System
• Continual tracking of motion throughout treatment
• Continuously adapts to variations in breathing patterns in 3D
– Model updated throughout treatment based on both internal & external motion
• Beam automatically corrects for target movement
0.75mm targeting accuracy

Unique features of Cyberknife:
Shorter overall treatment time
Site Schedule Days
Lung cancer 60 Gy/3# 3 days
45 Gy/3# 3 days
Prostate 36.25 Gy/5# 5 days
Brain tumours 20-30 Gy/3-5 # 3-5 days
AVMs 12-25 Gy/1# 1 day
Single fraction Rx 12-25 Gy/1# 1 day
Cyberknife IMRT
36.25 Gy/5# 70 Gy/35#
~3 hours ~10 hours
Daily treatment
Cyberknife: 45 min
IMRT: 15 min
With Cyberknife both total duration (min) &
treatment days are short
Total treatment duration in hrs

• Highest level of comfort
• Pain-free / No anesthesia
• No invasive head or body frame
• No breath-holding during treatment
• Significantly reduces treatment time
• Treats only affected areas
• Minimizes acute side effects
• Treats tumors anywhere in the body
• Sub-millimeter accuracy
• Dynamic (Inter-fraction) motion tracking
Cyberknife : Advantages

Radiosurgery in urological malignancies
- Prostate cancer
- Renal cell cancer
- Urinary bladder cancer

• Most prevalent malignancy in males in western community
• 2nd MC cause of mortality in the west
• Uncommon in Asians, probably shorter lifespan
• In TMH, constitutes 2.4% of all registered pts in 2000
• In recent years, more early prostate cancer patients are diagnosed
with prostate cancer
• Prostate cancer is slow growing tumour, risk of bone metastasis is
high in ‘high risk’ group patient
Prostate cancer

Risk stratification
RISK STRATIFICATION
LOW RISK INTERMEDIATE HIGH
T1,2a, PSA < 10 ng/ml,
GS</=6
T2b,
GS=7
T3,4,PSA>20ng/ml,
GS>7
Wait & watch
Surgery
Radiation therapy
HT
Radiosurgery
Combination
Surgery
Radiation therapy
HT
Radiosurgery
Combination
Surgery
Radiation therapy
HT
Radiosurgery
Combination

Radiotherapy
Radiation techniques:
2D Planning
Conformal Radiation therapy
- 3D-CRT
- IMRT
- SBRT
Target volume:
CTV – prostate with capsule + SV
T1 & small T2 with less PSA less GS only prostate is sufficient.
PTV – 1 cm margin.
Inclusion of pelvic lymph nodes still controversial.

Ca prostate Incidence of pelvic LN metastasis at diagnosis
Study T1a,b T1c T2a T2b,c T3
Pisansky 12/457
(2.6%)
15/456
(3.3%)
130/1206
(10.8%)
81/320
(25%)
-
Petros &
Catalona
2/61
(3.3%)
33/425
(7.8%)
0
Sands 6/127 (5%) 41/243
(16.9%)
95/199
(47.7%)
Van
Poppel
2/40(5%) 18/199
(9%)
25/46
(54%)
Hanks 1/21(5%) 38/135(28%) 48/95(50%)

Radiotherapy Radiation therapy schedules
Conventional fractionation:
- 70Gy/ 35# / 7 wk
- 2Gy/#
- Acute rectal & bladder toxicity
Hypofractionation schedule:
- High dose per fraction, short course treatment
- Equivalent loco-regional control
Ultra-hypofractionation schedule:
- Very short course, high dose per fraction
- Usual treatment duration 5 to 7 days

Conformal Radiation therapy
reduces toxicity
• RCT
• Royal Marsden Tait et al.Gr 2 or more 5 Vs 15%.
• Rotterdam trial Koper et al.
Grade 2 GI toxicity (32% vs. 19%, p = 0.02).
• M.D. Anderson Storey et al.
No dif but Dose 78 vs 70.
• Nonrandomized trials
• 15/27 improvement
• Most pronounced when dose escalation was not used.
• When dose escalation was used, no increased toxicity was demonstrated, except when the dose to the rectum >75 Gy.
• No article suggested increased toxicity with 3D-CRT for similar doses delivered compared with
conventional RT.

WPRT VS PORT:RTOG trial 9413
1323 patients with localized disease andrisk of LN involvement >15% & PSA <100
WP RT+ NCHT
PFS 60%
PO RT+ NCHT
44%
WP RT+ AHT
49%
PO RT+ AHT
50%
• WP RT NCHT improves PFS compared with PO RT and NCHT or PO RT and AHT, and
compared with WPRT + AHT in patients with a risk of LN involvement of 15%.
•Median follow-up : 59.5 mnths
• No OS advantage JCO 2003

Subset analysis of RTOG 9413
Subset of 694 patients studied
325 patients WP RT N&CHT
Median PFS 5.2yrs
324 patients PO RT N&CHT.
FS ≥10 × 11 but <11 × 11
cm)
MP FS<10x11cm
•Median PFS was 5.2, 3.7, and 2.9 years ( p 0.02).
•7-year PFS was 40%, 35%, and 27%
•RT field size has a major impact on PFS, and it is advised that
nodal treatment should be done in patients with a risk of LN inv >15% .
Roach IJROBP 2006

Dose escalation: improve LC


Author Study type Patient criteria Study details Results
Kurban et al Prospective
multi-
institutional
N= 4839
1986-95
T1-2 low risk
prostate cancer
No neo-adj HT
RT dose 60-78 Gy
3DCRT planming
Median FU 6.3 yrs
8-year PSA control rates were 72
to 93%. Dose >72 Gy had lower
PSA relapse rate.
Zietman MDACC
Randomized
N= 393
T1-2 disease
PSA < 105ng/dl
Arm 1: Conv RT 70.2 Gy
Arm 2: Conv RT 79.2 Gy
Median FU: 5.5 yrs
5-yr PSA rFS higher with dose
escalation (61% vs 80%). 49%
risk reduction in biochemical
failure.
Pollack et al MDACC
Randomized
N=301
Low risk prostate
cancer
Arm 1 (n=150): Conv RT 70
Gy
Arm 2 (151): 3DCRT 78 Gy
PSA rFS higher with dose
escalation (70% versus 64%;
p=0.03)
Peeters et al Randomized
Netherland
N=669
T1-4
Arm 1 (n=150): Conv RT 68
Gy
Arm 2 (151): Conv RT 78 Gy
Median FU: 51 months
5-yr PSA relapse-free survival
superior with high dose (64% vs.
54%; p = .02).
Zelefsky et al Randomized
MSKCC
N=1100
1988-98
RT dose systematically
increased from 64.8 to 86.4
Gy by increments of 5.4 Gy
in consecutive groups of pts.
5-yr PSA rFS was higher with
dose escalation in favorable,
intermediate and unfavourable
groups.
Zelefsky et al Single arm N=561
1996-2000
RT dose: 81 Gy to PTV 8-yr PSA rFS for favorable-,
intermediate-, and unfavorable-
risk groups were 85%, 76%, 72%
Prostate Cancer: Dose escalation studies

Intensity modulated radiation therapy
76- 81 Gy at 2 Gy/# dose delivered
Dose to target higher
Rectal & Bladder dose is high
High acute reactions
Dose escalation methods
IMRT/ 3DCRT

Dose escalation methods
Brachytherapy

Dose escalation methods
Brachytherapy seed implant

Dose escalation methods
HDR Brachytherapy implant
HDR brachytherapy implant
High dose rate
Invasive procedure
Skill dependent

Toxicities after Radiation therapy
Rectal toxicity
- Telengectasia
- Bleeding
- Bladder toxicity
- Incontinence
- Bleeding
- Thimble bladder
- Urethral stricture
-Erectile dysfunction
- Quality of life

Toxicity depends upon dose

Motion during treatment is a problem in Prostate Cancer
Cyberknife is the only technology which corrects movement between each field treatment

Author Study Patient criteria Study details Results
Martin Prospect
ive
PMH
N= 92
June 2001- Mar
2004
60 Gy /20 fr/ 4 wks
IMRT, FU: 38 mo
3 yr PSA relapse free was 76%.
RTOG Gr ≥3 GI toxicity in 1 patient
Kupelian Clevelan
d Clinic
N= 770
1998-2005
70 Gy; 2.5-Gy/fr/ 5
wks.
FU: 45 mo
5 yr PSA relapse free of low,
intermediate and high-risk disease was
95%, 85%, and 68%, respectively.
Livsey Retrosp
ective
Manche
ster
N= 705 men
T1-T4 disease
1995 -1998
Conformal RT (50
Gy/16fr/ 22 days)
Median FU: 48
months
Favourable, intermediate, poor
prognostic groups biochemical control
was 82%, 56%, and 39%. RTOG Gr ≥2
GI and bowel toxicity was 5% and 9%.
Lukka Randomi
zed
NCI
Canada
N= 936
Mar 1995-
Dec1998
Long arm: 66 Gy/33
fr 45 days
Short arm: 52.5
Gy/20 fr 28 days
5 yrs, PSA relapse free survival was
52.95% in long and 59.95% in short arm.
GI toxicity higher with short arm (11% vs
7%)
Tsuji Chiba
Japan
N=201
June 1995-Feb
2004
Three clinical trials RTOG Gr ≥2 GI toxicity. 5-yr PSA
relapse-free survival 83.2% without any
local recurrence.
Prostate Cancer: Hypofractionation studies


Author Study Patient criteria Study details Results
King Prospective N=41
Stanford
SBRT (CyberKnife)
36.25 Gy/ 5 fr/ 1 week
Median FU: 33 months
Biochemical control 100%
At 12 months, 78% achieved PSA nadir
RTOG Gr ≥3 rectal toxicity 4.8%
Friedland Prospective N=112
Naples
Feb2005-Dec
2006
SBRT (CyberKnife)
RT dose: 35-36 Gy/5 fr
Median FU: 24 months
3 patients had failure (two local and one
distant failure). 82% no erectile
dysfunction
Brachytherapy
Galalae Three centre
data
N=611
Localized
prostate cancer
HDR brachytherapy
combined with EBRT
5-yr PSA relapse-free survival were 96%,
88%, and 69% for favorable-,
intermediate-, and unfavorable-risk
patients
Prostate Cancer: Ultra-hypofractionation studies



Fullar et al, IJROBP 2008
Radiosurgery mimicking brachytherapy

Fullar et al, IJROBP 2008
Radiosurgery mimicking brachytherapy

Fullar et al, IJROBP 2008
Radiosurgery vs brachytherapy: Dosimetry

Radiosurgery vs brachytherapy: Dosimetry
Fullar et al, IJROBP 2008


Hossain et al, IJROBP 2010
SBRT vs IMRT : Dosimetry

Hossain et al, IJROBP 2010
SBRT vs IMRT : Dose distribution

Hossain et al, IJROBP 2010

Hossain et al, IJROBP 2010

Hossain et al, IJROBP 2010

SBRT: Early outcome of Ph II study (n=45)

SBRT: Early outcome of Ph II study (n=45)

SBRT: Clinical outcome (n=112)
Frieland et al, IJROBP 2009

Probability of maintaining erectile function
Robinson et al IJROBP 2002

King et al. IJROBP 2010
QOL: Sexual function domains
5 yr FU data with biochemical control & QOL function

QOL: Sexual function domains
King et al. IJROBP 2010


Aluwin J of Endourology 2010
Experiences from new centres

Aluwin J of Endourology 2010
Experiences from new centres




Stage Grade Treatment Treatment of recurrence
/ residual disease
Ta G1 TURBT + Immediate single
chemotherapy instillation with in
24 hrs of TURBT
Repeat TURBT
If sign of muscle
invasion consider
cystectomyG2-3
TURBT + Intravesicle therapyTcis G1-3
T1 G1-3
Superficial urinary Bladder

Author Study type Study details Results Remarks
van der
Werf-
Messing
Randomized
( n= 174)
Arm1: pre-OP RT
(30 Gy/15 fr) +
Nephrectomy
Arm 2:
Nephrectomy only
5 yr Survival:
50%
No difference between
Surgery alone and Pre-
OP RT + Surgery arm;
Increased resectability
in T3 disease
Juusela Randomized
(n=88)
Arm 1:
Nephrectomy alone
Arm 2: Pre OP RT
(33Gy; 2.2 Gy/Fr) +
Nephrectomy
5 yr Survival:
Arm 1: 63%
Arm 2: 47%
(p-value= NS)
No difference in
survival
Renal cell cancer: Pre-OP RT

Renal cell cancer: Post-OP RTAuthor Study type Study details Results Remarks
Kao GD Retrospective
(n=12)
Loco-regionally
advanced RCC
RT dose: 41.4- 63 Gy;
1.8-2 Gy/Fr
5 yr local control
rate 100%
High precision RT was used.
Acceptable toxicity profile.
Rabinovitch RA Prospective
Non-randomized
n=172;
year1978-88
Early (T1-2) localized
RCC
Treated with surgery
alone
7 yr actuarial loco-
regional failure 5%
30 pts had distant
metastasis
Adjuvant treatment may not
be useful in early RCCs
without nodal involvement.
Fugitt RB Randomized New Castle, United
Kingdom,
RT dose 55 Gy in 2.04
Gy/Fr
No survival
advantage with
PORT
4 patients died due to RT
induced hepatotoxicity
Kjaer M Randomized Copenhagen Renal
Cancer Study Group
Stage II/III RCC
RT dose 50Gy/20
fractions
No Survival
advantage with
PORT
44% had significant GI
complication
19% died due to RT induced
complications.
Sub-optimal radiation
therapy delivered

Author Study type Study details Results
Walsh L Prospective
n=12
Nude mice were injected
subcutaneously with A498 human
RCC cells.
RT dose: 48 Gy/3 fr(one per
week)
At 7 wks post-RT,
30% reduction in
volume
Beitler JJ Prospective
n=9
Medically inoperable RCC
SBRT
40 Gy/5 fr/1 week
Median FU 26.7 months
OS: 46% (4/9)
Loco-regional failure:
11% (1/9)
Wersall PJ Prospective
n=8
Medically inoperable RCC
SBRT
40 Gy/5 fr/1 week
Median FU 26.7 months
median OS: 58
months
loco-regional control
87%
Renal cell cancer: SBRT





Urological malignancies: Role of SBRT
Conclusion
- Hypofractionated RT / SBRT is an option in low risk carcinoma prostate
- Short course RT is equally effective compared with conv RT
- Short course RT is well tolerated and have similar gr 3/4 toxicities.
- Biochemical control is impressive in short term follow up data
-Need long term follow up data
- Radiosurgery is an interesting option in RCC & metastatic disease.

Indications of Cyberknife: Intracranial lesions
• Benign intracranial tumours
- Acustic neuromas
- Schwannomas
- Small meningiomas
- Chordomas
- Residual low grade gliomas
- Atriovenous malformation (AVMs)
• High grade gliomas after recurrence / post RT residual disease.

Indications of Cyberknife:
Extra-cranial lesions
• Small (T1) primary lung cancer
• Localized prostate cancer.
• Inoperable pancreatic cancer.
• Localized gall bladder cancer.
• Recurrent head and neck cancer in primary site or node.
• Residual disease/ boost treatment in nasopharynx/PNS region.

Indications of Cyberknife: Metastatic disease
• Solitary (or Oligo) brain metastasis.
• Solitary (or Oligo) lung metastasis.
• Solitary (or Oligo) liver metastasis.
• Isolated bone metastasis.