Embed Size (px)
DESCRIPTION
Citation preview

CYANOTIC CYANOTIC HEART DEFECTSHEART DEFECTS
Ma. Tosca Cybil A. Torres, RN

CYANOTIC HEART DEFECTS● Permit unoxygenated or desaturated blood to enter the systemic
circulation. ● Infants with complex or mixing cyanotic heart lesions who are
dependent on having a PDA for all or the majority of their pulmonary or systemic blood flow can become severely symptomatic within the first few days of life as the ductus arteriosus begins to close. They often need emergency management with medical or surgical intervention to survive the neonatal period.
● PGE1 is a potent vasodilating drug that is administered to prevent closure of the ductus or to reopen the ductus arteriosus and restore pulmonary or systemic blood flow. Continuous infusion of the drug may improve arterial oxygen saturation and tissue perfusion, allowing the infant to be stabilized in anticipation of further diagnostic and treatment interventions. It is rapidly metabolized through the pulmonary circulation and excreted through the renal system. It must be infused by continuous IV administration. The major side effect is apnea and infants frequently require intubation.

CYANOTIC HEART DEFECTS● Cyanosis – bluish discoloration of the skin and nail beds and mucus membranes appears
when tissues are deprived of adequate amount of O2.● It becomes visible when hemoglobin, approximately 5 gms/dl blood circulates unbound
to O2 and the measured O2 saturation drops below 85%.● Cardiac lesions produce cyanosis when desaturated blood from the venous system
enters the saturated arterial system without passing through the lungs.● Cyanosis can occur when:
1. blood flow to the lungs is decreased or insufficient.2. deoxygenated or desaturated blood is pumped to the body and a decreased, normal, or increased amount of deoxygenated and oxygenated blood is pumped to the lungs.
These are due to:1. right to left shunting lesions when blood flow to the lungs is decreased and there is a
communication between the intracardiac chambers or great vessels (ex. TOF).2. Mixing lesions where blood flow to the lungs is increased or normal and there is a
connection between the great arteries (ex. Single ventricle without pulmonary stenosis or tricuspid atresia)
3. Pulmonary hypertension or pulmonary vascular disease and a communication between the intracardiac chambers or great vessels (Eisenmerger’s complex)

CYANOTIC HEART DEFECTSClinical consequences of cyanosis:
1. Polycythemia2. Anemia3. Clotting abnormalities4. Hypercyanotic episodes or tet spells ( rapid and deep respirations, irritability and crying, peripheral vasodilation, increased systemic venous return, increasing cyanosis that can be very severe and decreased systolic murmur reflecting decreased pulmonary blood flow.5. CNS injury caused by abscess or embolic events.6. Pulmonary hypertension7. Endocarditis

CYANOTIC HEART DEFECTS Hypercyanotic episode:● As the child becomes more cyanotic, the child experiences
increased tachypnea and hyperpnia and this increase the degree of right to left shunting.
● treatment of the episodes includes:1. Calming the infant, placing the infant in the knee-chest position, and administering O2.2. Morphine SO4 is administered to suppress the respiratory center and decrease the degree of hyperpnea.3. Potent medication that causes vasoconstriction (ex. Phenylephrine) may be needed to increase systemic vascular resistance, decrease the degree of right to left shunting, and force blood into the pulmonary system.

Tetralogy of Fallot (TOF)• Incidence and Pathophysiology:● TOF accounts for 8%-10% of all CHDs, and is the most common
cyanotic lesion seen in the 1st year of life.● Misalignment of ventricular septum during fetal development results
in the constellation of three of the four characteristics of this lesion.a. VSDb. Pulmonary stenosis (infundibular/ subpulmonic, valvular, and
supravalvular)c. Overriding of the aorta (into the right ventricular side instead of
the over the left ventricle)d. RVH develops secondary to the pulmonary stenosis (also known
as right ventricular outflow tract obstruction)

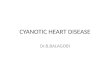
Tetralogy of Fallot

Altered Hemodynamics:
● The degree of pulmonary stenosis (infundibular, valvular, supravalvular) determines the resistance to blood flow out to the lungs through the pulmonary artery.
● The VSD is usually large and the pressures in both ventricles are equal. So the saturated blood enters the RV from the RA, it can flow into the coronary artery or shunt right to left into the aorta (causing desaturated blood to enter the systemic circulation),depending on the relative resistance of the pulmonary versus the aortic circulation.

Tetralogy of Fallot (TOF)Manifestations:1. The degree of pulmonary stenosis governs the onset and severity of the
symptoms. The more severe the pulmonary stenosis (primarily infundibular stenosis), the less pulmonary blood flow, the greater the right to left shunting, and the more cyanotic and desaturated the patient.
2. If pulmonary stenosis is mild, there is little or no right to left shunting. The saturation can be normal or low normal. This is known as “pink tet”.
3. Some infants present as cyanotic newborns. When antegrade (forward) pulmonary blood flow is severely impeded because of pulmonary stenosis, blood flow to the lungs depends on a PDA. As the mixed saturated blood enters the aorta, certain amount will shunt through the ductus arteriosus into the pulmonary arteries, allowing it to be oxygenated. As this structure closes, the NB becomes profoundly cyanotic.
4. Other infants become cyanotic over the 1st few months of life. Initially, they may tire easily, especially with exertion, and may have difficulty feeding and gaining weight before cyanosis develops. In time these infants may have hypercyanotic episodes, as well as other clinical signs of chronic hypoxemia.
5. Auscultation reveals a harsh systolic murmur, often accompanied by a palpable thrill.
6. The heart is “boot shaped” on chest x-ray because of poor development of the pulmonary artery.

Tetralogy of Fallot (TOF)Therapeutic Management:a. Medical Management:1. Continuous PGE1 infusion to maintain ductal patency for
symptomatic NB (severe desaturation related to decreased pulmonary blood flow or frequent tet spells).
2. Close monitoring for signs and symptoms of worsening hypoxemia for older infants.
3. Illnesses that put them at risk for dehydration must be treated promptly.
4. Hemoglobin and hematocrit levels must be evaluated to assess for anemia.
5. Close monitoring for hypercyanortic episodes may detect some very subtle and often self limiting episodes lasting 10-15 minutes.

Tetralogy of Fallot (TOF)b. Surgical Management:1. Primary repair during infancy has become the
treatment of choice of many centers with surgery scheduled at 2-4 months of age for asymptomatic infants. This is to normalize the physiology sooner and promote normal growth of the pulmonary arteries. It requires CP bypass.
● Postop complications include: rhythm disturbances (ex. Narrow complex tachycardia, varying degrees of heart block), residual VSD, low CO related to RV dysfunction, residual RV outflow obstruction and branch pulmonary artery stenosis.
● Mortality rate is 2%-5%.● Decisions and considerations regarding palliative or
definitive repairs include institutional approach, associated anatomic issues such as abnormal coronary arteries, branch pulmonary artery size or stenosis, infant size and whether pulmonary atresia is also present.
● Earlier surgical intervention is indicated for increasing or severe cyanosis, significant polycythemia, or hypercyanotic episodes.

2. Modified Blalock – Taussig Procedure – the most commonly performed in some symptomatic NBs that are poor candidates for primary repair. This is a lower risk surgical procedure by creating a systemic – pulmonary artery shunt to increase the pulmonary blood flow. This is usually not done with the child in CP bypass.
● Complications are the same as for thoracotomy incision, including pneumothorax, stridor (harsh vibrating sound heard during respiration obstructing air passage) from recurrent laryngeal nerve injury, diaphragm paresis from phrenic nerve injury, and chylothorax from injury to the thoracic duct. In addition, shunt failure because of thrombosis or clot remains a potential major problem.

Tricuspid AtresiaIncidence and Pathophysiology:● It represents approximately 2%-3% of all CHDs. It is the 3rd most
common cyanotic cardiac condition. ● It is a complex lesion with many variations. In this lesion, the
tricuspid valve does not develop. An ASD or patent foramen ovale must be present for the fetus or infant to survive.
● The RV is hypoplastic (underdeveloped).The VSD can be of varying size. The pulmonary artery may be in the normal position or transpose with the aorta.
● There may be pulmonary stenosis of varying degrees. The NB may depend on the ductus arteriosus for pulmonary blood flow. The degree of cyanosis and symptoms are related to these multiple factors.

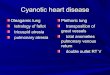
Tricuspid Atresia

Altered Hemodynamics:
● The desaturated blood enters the RA and is shunted right to left through the patent foramen ovale/ASD into the LA, since it cannot flow into the RV because the tricuspid valve is atretic or absent. In the LA, the desaturated blood mixes with the saturated blood (returning from the lungs) and from the LA, it flows through the mitral valve into the LV
● Some of the mixed saturated blood flows out of the aorta and to systemic circulation. Some will flow through the VSD and into the right ventricular chamber into the pulmonary artery into the lungs to become oxygenated.
● For children with severe pulmonary stenosis and no VSD or other complex anatomy, the PDA is critical to ensure pulmonary blood flow.

Tricuspid AtresiaManifestations:1. Profound cyanosis maybe present in the
neonate and is usually visible within the 1st few hours of life in neonates with decreased pulmonary blood flow. Infants with increased pulmonary blood flow present with milder cyanosis and increasing signs of CHF.
2. Single heart sound is present because there is no closure of the tricuspid valve.
3. A systolic murmur of the VSD or a PDA murmur may be heard (if patent)

Therapeutic Management:
a. Medical Management1. PGE1 infusion is initiated for infants who depend on the
PDA for pulmonary blood flow; and the infant is stabilized and readied for surgery.
b. Interventional Cardiac catheterization1. Balloon atrial septostomy during cardiac catheterization to
allow blood to flow from the RA to the LA.● A catheter is inserted into the femoral vein and advanced
into the RA and across the foramen ovale/intraatrial septum. A balloon in this catheter is then inflated, and this balloon is pulled back through the foramen ovale, tearing the septum. If the balloon procedure is not effective, and can happen in infants beyond NB age, a catheter blade septostomy can be performed to cut the septum.

Tricuspid Atresiac. Surgical Management:● The goal of this staged palliative repair is to
separate the desaturated and saturated blood, thereby eliminating cyanosis. The equally important role is to optimize ventricular function, by decreasing the workload (volume overload) on the heart.
Norwood Procedure -is a series of three open-heart surgeries that gradually improve certain life-threatening forms of congenital heart disease
1. Systemic to pulmonary artery shunt (Blalock Taussig Shunt)– to provide adequate pulmonary blood flow if significant pulmonary stenosis is present. This is the 1st procedure in a three-stage effort to palliate this defect.

2. Hemi-Fontan (Bi-directional Glenn procedure) – is performed at 4-6 months of age, once the pulmonary vascular resistance has decreased to normal pressures. In this procedure, the SVC is connected directly to the pulmonary arteries, thereby reducing left ventricular volume load by 1/3. This part of the blood flow to the lungs is now by passive flow, since it is not pumped by the RV to the lungs.

• Pulmonary hypertension must be prevented and managed aggressively postop to ensure adequate pulmonary blood flow. Position the child with the head of the bed up to encourage blood flow to the lungs will help decrease the degree of venous congestion in the upper body.
● Pleural effusions can develop as the body adjusts to the flow and pressure changes. Occasionally, atrial dysrythmias are seen. SVC syndrome may be present, this is a condition in which SVC pressures are elevated and the patients have upper body edema or plethora. It can occur when there is an obstruction at the SVC to branch pulmonary artery anastomosis, abnormal pulmonary artery anatomy, or elevated pulmonary vascular resistance

Tricuspid Atresia3. Fontan Operation – the 3rd procedure, is usually performed
between ages 18 months and 6 years period. Desaturated blood is directly channeled from the IVC to the pulmonary arteries.

The goals of the Fontan procedure are:a. separation of the desaturated venous and saturated
arterial blood.b. Volume unloading of the single ventricle. ● Sometimes, a small connection between the venous and
the arterial circulations is maintained called fenestration. This is placed in case the pressures are slightly higher than normal in the pulmonary arteries is that some desaturated blood can shunt right to left to the systemic circulation until the pulmonary arteries adjust to the new flow and pressures. At a later time, the fenestration may be closed. This can be done in the cardiac catheterization laboratory if an adjustable tie has been placed at the time of the fontan procedure.
● Surgical mortality declined and is now reported to be 4%-8%.

Pulmonary Atresia with intact ventricular septumIncidence and
Pathophysiology:
● it accounts for approximately 3% of all CHDs. The causes of this lesion are the failure of the pulmonary valve to develop, accompanied by hypoplastic development of the pulmonary artery and RV. The tricuspid valve may also be underdeveloped. The RV pressures maybe extremely high, and the coronary arteries may also be abnormal.

Altered hemodynamics:● As the blood enters the RV, it cannot flow directly to the
pulmonary arteries because of atresia of the pulmonary valve. The blood entering the RV is propelled back through the tricuspid valve into the RA and shunted right to left through the foramen ovale to the LA. The desaturated blood and saturated blood mix in the LA and flow through the mitral valve and into the LV, where the mix blood is pumped to the aorta. From the aorta, this mixed saturated blood flows to the body and brain. Oxygenation of the blood occurs through persistent PDA into the pulmonary arteries and to the lungs.
Manifestations:1. Profound cyanosis is seen during the early neonatal period.
Survival depends on the presence of PDA.2. S2 single.3. Soft or continuous systolic murmur if PDA is present.

Pulmonary Atresia with intact ventricular septum Therapeutic management:a. Medical Management;1. Continuous PGE1 infusion for NB to maintain ductal patency. b. Surgical management:● The primary treatment for this lesion.1. Pulmonary Valvotomy or Transannular patch as the early surgical interventions and/or the
creation of a systemic to pulmonary artery shunt (Blalock-Taussig shunt).● Valvotomy may encourage growth of the RV. Over time, right to left shunting of the atrial level may decrease as the RV increases the amount of blood it pumps to the pulmonary system.

2. Bidirectional Glenn Procedure or staging to the modified fontan procedure is performed if the RV remains very small and cannot pump an adequate amount of blood to the lungs.● Surgical mortality ranges from 19% after the 1st procedure to 36% after both procedures.
Contraindications for pulmonary valvotomy:1. Very high RV pressures and associated coronary artery
abnormalities because there would be inadequate coronary blood flow, MI and ventricular muscle dysfunction.
● These children are given a systemic to pulmonary artery shunt and then staged as for a single ventricle. Sometimes, cardiac transplantation may be indicated for this subgroup of children with pulmonary atresia and intact ventricular septum.

Truncus arteriosusIncidence and Pathophysiology:● It accounts for 1%-4% of all CHDs.● It is marked by incomplete division of the common great vessels. The truncus arteriosus,
which normally divides into the pulmonary artery and pulmonary valve and the aorta and aortic valve. This failure in division results in a single large vessel and single valve, which gives rise to the pulmonary, systemic and coronary circulations.
● The ventricular septum fails to develop at the same time, therefore VSD is present. The common truncal arteriosus vessel overrides the VSD and receives both right and left ventricles.

Altered Hemodynamics:● Desaturated blood enters the RA and flows through the
tricuspid valve into the RV. Saturated blood from the LA flows through the mitral valve and into the LV. The desaturated and saturated blood mixes in the ventricles at the level of the VSD and common ventricular outflow tract. The common great vessel sends this mixed blood to the systemic, pulmonary, and coronary circulations. O2 saturation depends on the volume of pulmonary blood flow related to the pulmonary vascular resistance; the greater this flow the more symptoms of CHF, decreased CO, and potential for coronary artery ischemia. The ventricles are under pressure and volume overload.

Truncus ArteriosusManifestations:1. The infant presents (often in the neonatal period),
with CHF and some degree of cyanosis. The volume of pulmonary blood flow determines the severity of symptoms. Unrestricted flow to the pulmonary artery results in pulmonary congestion and severe CHF. If pulmonic stenosis is present, pulmonary blood flow is limited and cyanosis increases.
2. A harsh systolic murmur is heard and may be accompanied by thrill. A diastolic murmur of truncal valve insufficiency may be heard. The opening of the single truncal valve may produce a click.
3. Bounding pulses and a widened pulse pressure because of truncal insufficiency.

Therapeutic Management:
a.Medical Management: aimed at reducing the effects of CHF and preventing polycythemia
1.CHF is treated with digoxin and diuretics.
b. Surgical Management:1. Pulmonary artery
banding for NBs who do not respond to early medical management.

2. Rastelli repair- Total corrective repair includes closing the VSD and placement of a conduit from the RV to the pulmonary artery.

3. Valvuloplasty of the truncal valve which is the new aortic valve may be performed to improve valvular competence. Blood flow postop is normal.● Surgical mortality is about 5% - 10% in children who do not have associated malformations.
4.Conduit replacement is necessary as the child grows and a future truncal valve repair or replacement may be needed.

Hypoplastic Left Heart SyndromeIncidence and pathophysiology:● Accounts for 1% of all CHDs. It is seen more frequently in
males than in females. Approximately 95% of all affected infants who are untreated will die within the 1st months of life.
● Inadequate development of the left side of the heart results in only one effective ventricle. The syndrome may include aortic valve atresia, hypoplasia of the LV, atresia or hypoplasia of the ascending aorta, and mitral valve stenosis or atresia. Most infants have intact ventricular septum.

Hypoplastic Left Heart Syndrome

Altered Hemodynamics:● Saturated pulmonary venous blood return is
unable to flow from the LA through the rest of the left side of the heart. It is shunted left to right through a patent foramen ovale into the RA, where it mixes with desaturated blood. Mixed blood travels through the RV to the main pulmonary artery. A portion of blood flows to the branch pulmonary artery through the PDA to the descending aorta. From the aorta this mixed saturated blood provides systemic and coronary blood supply. The coronary blood supply is from retrograde flow in the ascending aorta.

Hypoplastic Left Heart SyndromeManifestations:1. Most infants present (within the first few days of life) with tachypnea and
early CHF from increased pulmonary blood flow and as the ductus arteriosus begins to close, systemic hypoperfusion and shock. The infant appears grayish blue in color with dyspnea and hypotension.
Therapeutic Management:● Nearly all neonates with hypoplastic left heart syndrome will die within the
first month of life without surgical intervention. a. Medical Management:
1. Emergency management addresses correction of the acid-base and electrolyte imbalances and reestablishment of ductal patency with PGE1.
b. Surgical Management1. Cardiac transplantation as a single, definitive correction has been successful
with 85% operative survival rate and 81% 5-year survival rate. ● The scarcity of neonatal donor heart, however, greatly limits the number of
infants who may receive transplant.

2. Norwood Procedure – a three-step palliative repair.a. The stage 1 procedure provides unobstructed blood flow from the RV to the main pulmonary artery, which is anastomosed to the ascending aorta to make a “neoaorta” (often with patch enlargement of the native aorta). The RV acts as the systemic ventricle. Pulmonary blood flow is supplied through a systemic-to-pulmonary artery surgical shunt.b. the 2nd stage, a bidirectional Glenn procedure, is performed at approximately 6 months of age. c. The palliation is completed usually by 6 yrs of age by a modified Fontan procedure. The 4-year survival after staged repair is greater than 50%; a 5-year survival 50%-70% depending on the associated factors.
● Postop and long term complications include hypoxemia, CHF, RV dysfunction, pulmonary artery anomalies, systemic venous hypertension, dysrythmia, endocarditis, and developmental delays.

Transposition of the Great Arteries
Transposition of the great arteries is a birth defect causing a fatal condition in which there is a reversal, or switch, in the truncal connections of the two main (great) blood vessels to the heart, the aorta and pulmonary artery.

Transposition of the Great Arteries

Manifestations: • Blueness of the skin • Shortness of breath • Poor feeding • Clubbing of the fingers or toes
Tests often include the following:• Chest x-ray • Cardiac catheterization • ECG • Echocardiogram (if done before birth, it is called a fetal
echocardiogram) • Pulse oximetry (to check blood oxygen level)

Surgical Management1. Mustard procedure or
the Senning procedure- creates a tunnel (a baffle) between the atria. This redirects the oxygen-rich blood to the right ventricle and aorta and the oxygen-poor blood to the left ventricle and the pulmonary artery. This operation is called an atrial or venous switch.

2. arterial switch operation- The aorta and pulmonary artery are switched back to their normal positions. The aorta is connected to the left ventricle, and the pulmonary artery is connected to the right ventricle. The coronary arteries, which carry the oxygen-rich blood that nourishes the heart muscle, also need to be re-attached to the new aorta.

NURSING CARE Assessment
1. Obtain thorough nursing history.2. Measure and record the height and weight and record.3. Record vital signs.4. Assess and record:
a. Skin color: pink, cyanotic, mottledb. Mucous membrane; dry, cyanoticc. Extremities; peripheral pulses for quality and symmetry, capillary refill, cool
5. Assess clubbing6. Assess chest wall for deformities.7. Assess respiratory pattern. (technique)8. Assess heart sounds.
a. Rate (brady,tachy or normal) and rhythmb. Identify murmurs.
9. Assess fluid statusa. Daily weight.b. Strict I & O
10. Assess and record the child’s level of activity.a. Observe the child at play, while feeding.

NURSING DIAGNOSESImpaired Gas exchange related to altered
pulmonary blood flow or pulmonary congestion.Decreased cardiac output related to decreased
myocardial function.Activity intolerance related to hypoxia or
decreased myocardial function.Altered Nutrition; Less than body requirements
related to excessive energy demands required by increased cardiac workload
Risk for infection related to chronic illness.Fear and anxiety related to life-threatening
illness.

NURSING INTERVENTIONS:1. Relieving respiratory distress.
a. Positioning.b. Suction oral and nasal secretionsc. Administer oxygen as prescribed.d. Administer prescribed meds and document response.
Diuretics Bronchodilators
e. May need to change oral feeding to NGT feeding.2. Improving Cardiac Output
a. Organize nsg care and meds schedule to provide periods of uninterrupted rest.
b. Provide play or educational activities that can be done in bed.c. Maintain normothermia.d. Administer prescribed meds
Diuretics (Furosemide, spirinolactone) Digoxin Afterload reducing meds (Captopril, enalapril)

NURSING INTERVENTIONS:3. Improving oxygenation and Activity tolerance
a. Continuous monitoring of VS (pulse oximeter)b. Administer oxygen as needed; assess response
4. Providing adequate nutritiona. Infants
Small frequent feedings Fortified formula or breast milk (up to 30 cal/oz) Limit oral feeding time to 15-20 mins Supplement oral feeds with NGT feeds as needed.
b. Report feeding intolerance: nausea, vomiting, diarrheac. Document daily weight (same time, scale, day)d. Record accurate I&O
5. Preventing infectiona. Maintain routine childhood immunization.b. Administer yearly influenza vaccine.c. Prevent exposure to communicable disease.d. Good hand washinge. Report feversf. Report signs of URTI
6. Reduce fear and anxietya. Educate patient and family.b. Provide the family with contact phone numbers of a cardiologist.c. Provide teachings on initial action in case of emergency situations.

EVALUATIONImproved oxygenation as evidenced by easy,
comfortable respirationImproved cardiac output as evidenced by
stable v/s and adequate peripheral perfusionIncreased activity levelMaximal nutritional status demonstrated by
weight gain and increase in growth curve percentile.
No signs of infection.Parents discuss diagnosis and treatment
together and with child.

End of Discussion