Embed Size (px)
Citation preview

Current Challenges in Pertussis Prevention: A Review
Dr Gaurav Gupta. 23 Sept 2016

Conflict of Interest
• Received grants from various vaccine manufacturers including – Sanofi Pasteur– GSK– Abbott– Novartis

Noel Preston (1988)‘There must be a few medical subjects that have generated so much controversy & even outright
contradiction, as pertussis’

Leila Denmark. Pearl Kendrick. Grace Eldering. Loney Clinton Gordon.
Women Power !

Scope of Discussion
• Is pertussis increasing? • Is aP responsible?• Pertussis immunity?• Why not just use wP vaccine?• Office practice suggestions?


Whooping Cough bounces back

Possible Reasons for Increasing Pertussis
• Cyclical outbreaks every 3 to 5 years• Changing epidemiology, waning immunity• Inadequate vaccination schedules and/or compliance • Increased awareness, Improved surveillance and diagnostic
methods (PCR etc.)• Changes in case definitions• Lower than desired vaccine efficacy• Potential mutation & antigenic drift
Cherry JD. Epidemic pertussis in 2012--the resurgence of a vaccine-preventable disease. N Engl J Med 2012;367:785-7.Clark TA, Messonnier NE, Hadler SC. Pertussis control: time for something new? Trends Microbiol 2012;20:211-3

Overview of Past Outbreaks
• Several large pertussis outbreaks have been reported in the past 20 years– Chicago, USA, 1993– Cincinati, USA, 1993– Nova Scotia, Canada, 1994– Vermont, USA, 1996– Netherlands, 1996– Sindh, Pakistan 2011– California, USA 2010-11– Washington, USA 2012
USA between 1980-89 had outbreaks almost every year!
Vaccines 5 ed. Plotkin; Emerging infectious diseases. Vol. 6, No. 4, July–August 2000; CMAJ February 14, 2006 • 174(4)
Whole cell vaccines

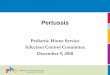
Global trends of pertussis incidence Substantial Heterogeneity in annual rates of change of pertussis incidence...
• Pink area Countries with significantly positive trends in incidence• White area Countries for which trends were not significant• Blue area Countries with significantly decreasing trendsSource: 1. Jackson D. W. & Rohani P. Review article - Perplexities of pertussis : recent global epidemiological trends & their potential causes. Epidemiol. Infect. (2014), 142, 672–684.
Inclusion criteria: mean DTP3 vaccine uptake of>80%, populations of>5 million & >80% complete case count records for this period
10

Knowledge is the process of piling up facts,wisdom lies in their simplification

Before generalized
use of pertussis vaccine in children
After generalized use of pertussis
vaccine in children
Hewlett EL, Edwards KM. Pertussis — Not Just for Kids. N Engl J Med 2005; 352: 1215-22.
Evolution of pertussis epidemiology

SAGE working group – 2014• Between country variance on multiple factors
– Vaccines – Population– Surveillance systems and diagnostic methods
• No evidence of global resurgence of pertussis• Both wP and aP Pertussis vaccines provide effective disease protection
– But evidence of earlier waning of immunity with aP vaccines• Resurgence seen in 5 of 19 countries
– Australia, Portugal, USA, UK (aP)– Chile (wP)
| 13
http://www.who.int/immunization/sage/meetings/2014/april/2_SAGE_April_Pertussis_Miller_Resurgence.pdf?ua=1

Colombia
Algeria
Brazil
Poland

Exclusive Use of Acellular Vaccines in Sweden Since 1996 Associated with Excellent Pertussis Control
Adapted from Nilsson L, von Segebaden K., Klink A-M, Grünewald M. Pertussis surveillance in Sweden: fourteen year report. Smittskyddsinstitutets (SMI).

More examples of aP using countries with no resurgences
• Norway: changed to aP in 1998 using 3/5/10 month schedule • Sweden: no vaccination prior to 1996 aP at 3,5 12 months • Finland: changed to aP in 2005 using 3,5,12 month schedule • Denmark: changed to aP in 1997 using 3,5 12 month schedule
| 16http://www.who.int/immunization/sage/meetings/2014/april/1_Pertussis_background_FINAL4_web.pdf?ua=1

DTaP Efficacy


Comparative efficacy of DTwP & DTaP vaccines
19
Source: 1. Edwards & Decker. In: Vaccines, 4th Edition, 2004. 2. Plotkin & Cadoz. PIDJ, 1997; 16 (5).

Components – Do they matter

COMPONENT COMPANY EFFICACY
1C Amvax, JNIH 71 TO 78%2C SKB 59%2C Pasteur Merieux 85%3C SKB (GSK) 84 %4C LEDERLE - an european vacc .
not marketed79 %
5C Connaught (Pasteur) 85 %DTwP VARIOUS countries 36 TO 96 %
Summary of vaccine efficacy: Cochrane 2012 (and 14)
Conclusion

Once adjusted for this aberration, the authors have conceded that their reviews would have
found no efficacy difference between the different licensed DTaP vaccines.

Antibody Response to aP Antigens (PT & FHA): High rates of seroconversion for anti-PT (82.9 to 100%) and anti-FHA titers (83.9 to 95.9%) after
the 3 dose primary vaccination with Pentaxim regardless of study population and primary vaccination schedule
Pentaxim licensed for use in over 100 countries, in NIP of 23 countries, over 100 million doses used

How long does immunity last?

Number of subjects: 263496 subjects (8-20 years of age)
Clin Infect Dis 2013;56:1248-54

The comparison of pertussis cases in wcP- vs acP vaccinated subjects
is really a comparison of pertussis in adolescents vaccinated with wcP
vs young children vaccinated with acp and since pertussis is much
more common in younger children they suggested that this finding
may have been confounded by age

Misegades LK, Winter K, Harriman K, et al. Association of childhood pertussis with receipt of 5 doses of pertussis vaccine by time since last vaccine dose, California, 2010. JAMA 2012;308:2126-32.

Overall DTaP-induced vaccine effectives (VE) and duration of protection estimates, California 2010
Case Control study in California (2010: 15 counties) to determine the vaccine effectiveness (VE) at different intervals after 5th dose of DTaP vaccine
Cases (n) Controls (n) VE, % 95% CI
Overall0 doses 53 19 Reference --
5 doses 629 1,997 88.7 79.4 – 93.8
Time since5th dose in months
0 doses 53 19 Reference --
< 12 m 19 354 98.1 96.1 – 99.1
12 – 23 m 51 391 95.3 91.2 – 97.5
24 – 35 m 79 366 92.3 86.6 – 95.5
36 – 47 m 108 304 87.3 76.2 – 93.2
48 – 59 m 141 294 82.8 68.7 – 90.6
60+ m 231 288 71.2 45.8 – 84.8
Adapted from Misegades LK et al. Association of childhood pertussis with receipt of 5 doses of pertussis vaccine by time since last vaccine dose, California, 2010. JAMA 2012;308:2126-32.
60+ : 61-83 months

Approximate duration of immunity after natural infection and after vaccination

• Both WHO and the CDC found that the acellular pertussis vaccines were effective at prevention of the disease,
• but had a limited impact on infection and transmission, meaning that vaccinated people could act as asymptomatic reservoirs of infection.

Why not use wP for everyone?

Frequency of Common Side Effects with Pertussis Vaccines
Event Whole cellpertussis vaccine
Acellularpertussis vaccine
Average Average Range
Fever < 38.3°C 44.5% 20.8% 16-29.2%
Fever > 38.3°C 15.9% 3.7% 1.6-5.9%
Erythema 56.3% 31.4% 15-44%
> 2.0 cm 16.4% 3.3% 1.4-5.9%
Swelling 38.5% 20.1% 7.5-24.2%
Drowsiness 62.0% 42.7% 29.4-52.2%
There is a very wide range among various aP with varying frequencies for individual side effects. Impossible to identify an aP with the most (or least) favourable adverse event profile.
Mathew JL. Acellular Pertussis Vaccines: Pertinent Issues, Indian Pediatrics 2008; 45:727-729

Meta-analysis of Serious Adverse Events with Pertussis vaccines
Event Frequencywith aP
Frequencywith wP
Pooled RR(95% CI)
Interpretation
High fever(>40°C)
227/99323 (0.23%)
996/96879(1.03%)
0.18(0.08-0.44)
RR is about 80% less with aP thanwith wP, but the absolutedifference is 2%.
Seizures(within 48 h)
58/106204 (0.05%)
224/103474(0.22%)
0.28(0.13-0.61)
RR is about 72% less with aP than with wP, but the absolutedifference is negligible.
Hypotensive-hyporesponsiveepisode
20/106204(0.02%)
491/103474(0.47%)
0.04(0.01-0.19)
RR is about 96% less with aP thanwith wP, but the absolutedifference is negligible.
Mathew JL. Acellular Pertussis Vaccines: Pertinent Issues, Indian Pediatrics 2008; 45:727-729
Relative risk for some events is less with aP, the absolute risk difference is comparable to wP because such events are very rare with both.

• The NIH-Multi Acellular Pertussis Trial
aP backboned vaccines are always better tolerated than wP vaccines
Decker & al. Pediatrics 1995
Fever Swelling Pain
Introduction of acP vaccine lead to a reduction of the emergency room admissions and hospital visits
• Approximately 90 emergency visits and 9 admissions per month are avoided by switching to the acP vaccine, mainly because of febrile and afebrile convulsions compared to the wcP vaccine period.
The NIH-Multi Acellular Pertussis Trial The Journal of Inf Dis (1996), pp. S270-S275

Role of aP vaccines
Basic purpose of Pertussis vaccination – prevent morbidity and mortality – max in infants and neonatesStrategies to reduce them• Adolescent vaccination• Maternal vaccination• Cocooning strategy• Vaccination of health care workers

Role of aP vaccines
Basic purpose of Pertussis vaccination – prevent morbidity and mortality – max in infants and neonatesStrategies to reduce them• Adolescent vaccination• Maternal vaccination• Cocooning strategy• Vaccination of health care workers

Office practice suggestions?

FAQs
• What to do with children having received all aP?
• How to counsel parents regarding wP & aP vaccines?

Summary
• Pertussis not yet conquered, though there is no global resurgence
• Outbreaks are not completely understood, and many studies have important methodological limitations
• Pertussis has been controlled in many countries using either aP or wP vaccines.
• Health-care providers need to choose pertussis vaccines that will best serve their patients while supporting public health goals














![[PPT]PowerPoint Presentation - IIT Kanpur · Web viewImage Processing Lecture 1 Introduction and Application Gaurav Gupta Shobhit Niranjan Instructors Gaurav Gupta Can catch at :](https://img.pdfslide.us/doc/110x75/5adff7017f8b9af05b8d14a3/pptpowerpoint-presentation-iit-viewimage-processing-lecture-1-introduction-and.jpg)