Embed Size (px)
Citation preview
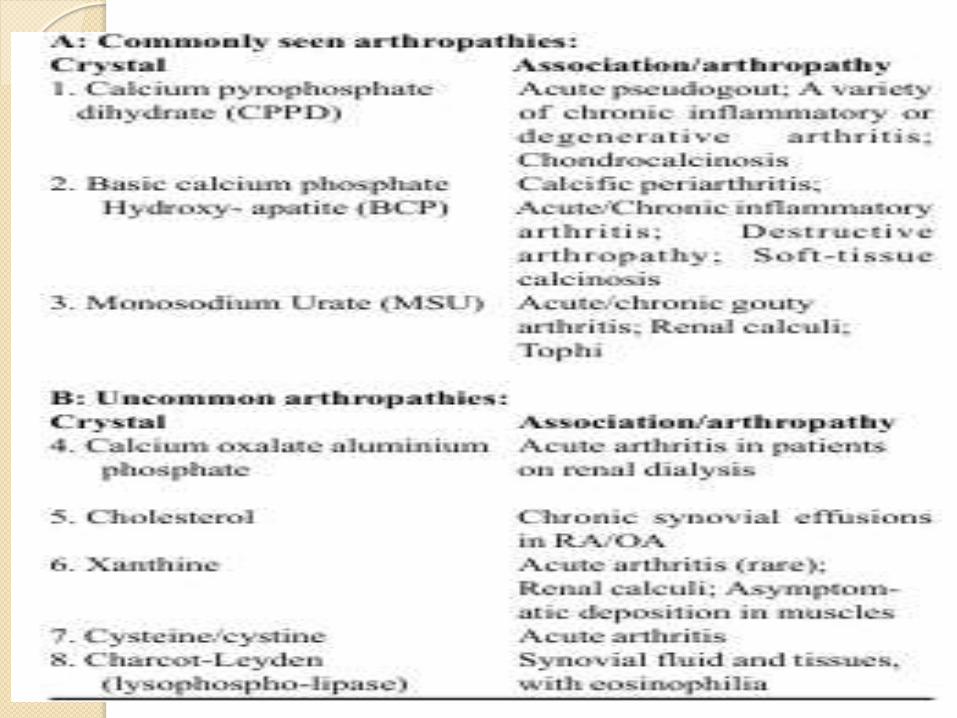
CRYSTAL ARTHRITIS
Dr. M Kasi Viswanadham
PG in Orthopaedics
GOUT
word Gout is derived from the latin
word ‘gutta’ means drop.
based on the ancient belief that the arthritis is due to
deposition of malevolent humor by evil spirits into the joint,
drop by drop
Gout is a disorder of purine metabolism
characterized by hyperuricaemia,
deposition of monosodium urate
monohydrate crystals in joints and peri-
articular tissues and recurrent attacks of
acute synovitis.
Late changes include cartilage
degeneration, renal dysfunction and uric
acid urolithiasis.
history
• 2640 BC: podagra first identified by the Egyptians
– 5th century BC: Hippocrates referred to gout as “unwalkable disease” and noted links between gout & lifestyle, demographics & other variables
Galen described the tophi.
Crystals in gouty tophi was first demonstrated
by Antony Van Leeuwenhoek in (1679 )
Sir Alfred Garrod demonstrated hyperuricemia as the basic cause of gout(1848)
McCarty and Hollander established the association between gouty arthritis and articular crystal deposition(1961)
Gout is much more common in men
than in women;
rare before menopause and more
common in old age
Male ,female ratio 2.7:1
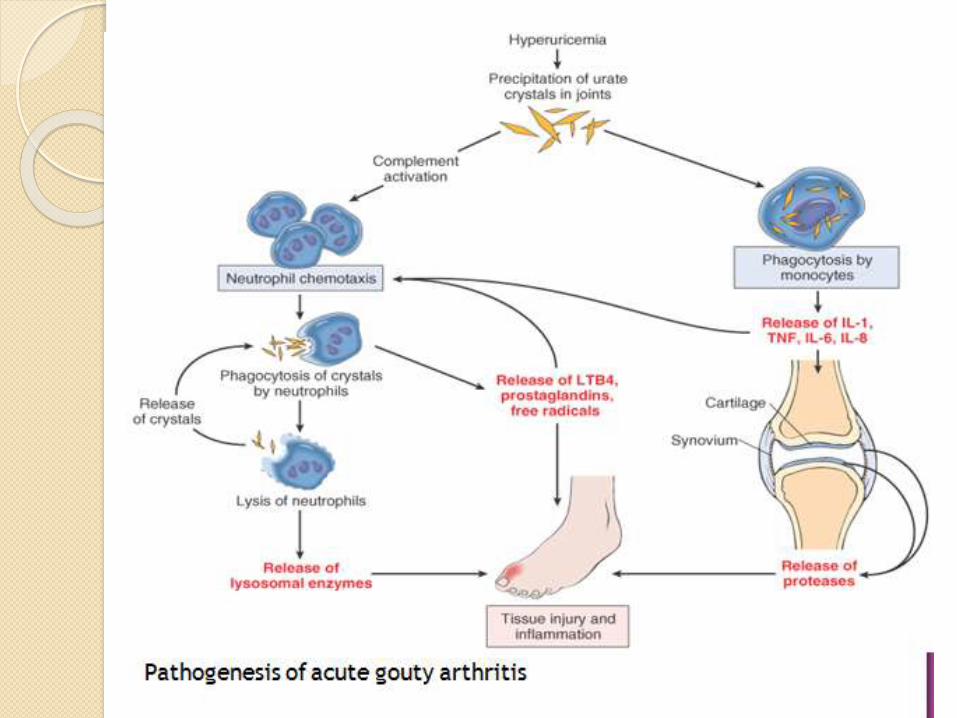
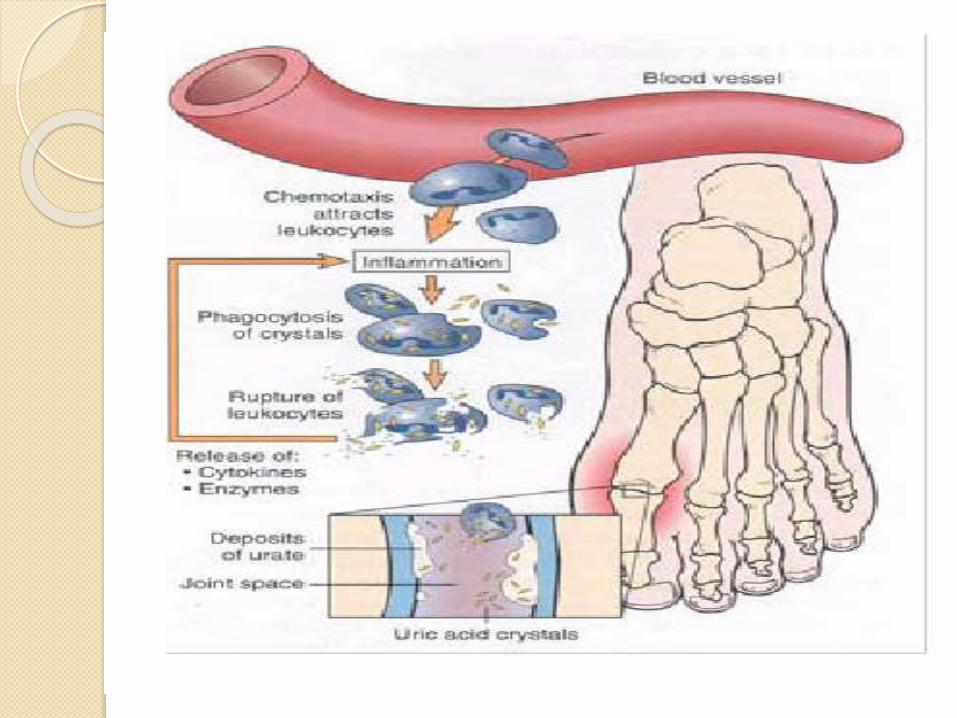
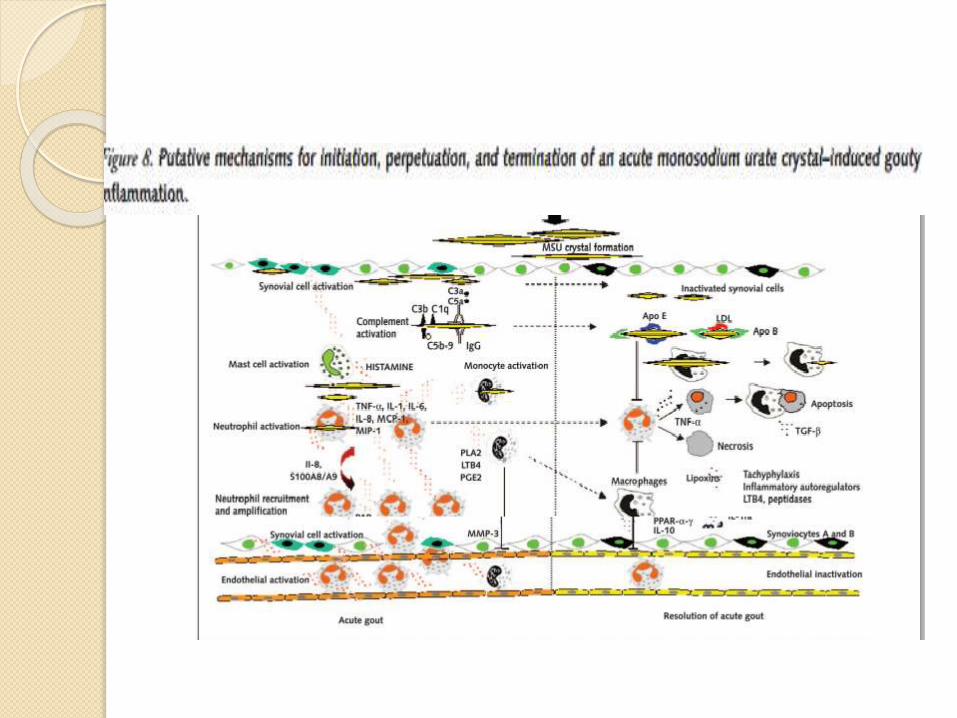
pathogenesis
The pathogenesis of gout depends on
three vital steps:
(1) the development of
hyperuricaemia;
(2) the formation of monosodium
urate monohydrate (urate) crystals;
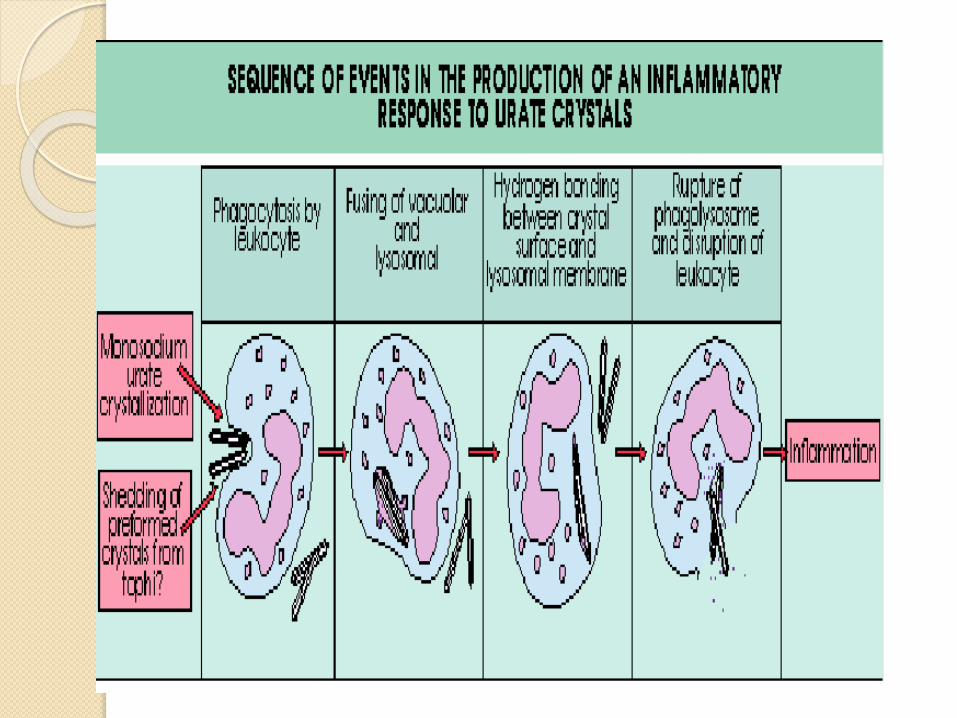
(3) the interaction between the urate
crystals and the inflammatory system.
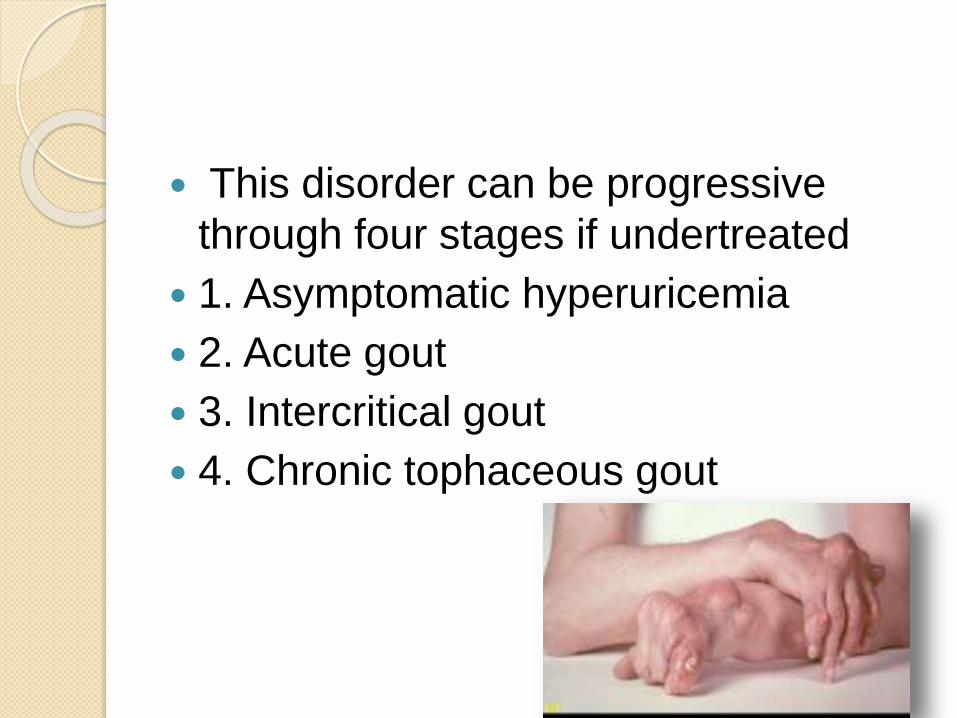
This disorder can be progressive
through four stages if undertreated
1. Asymptomatic hyperuricemia
2. Acute gout
3. Intercritical gout
4. Chronic tophaceous gout
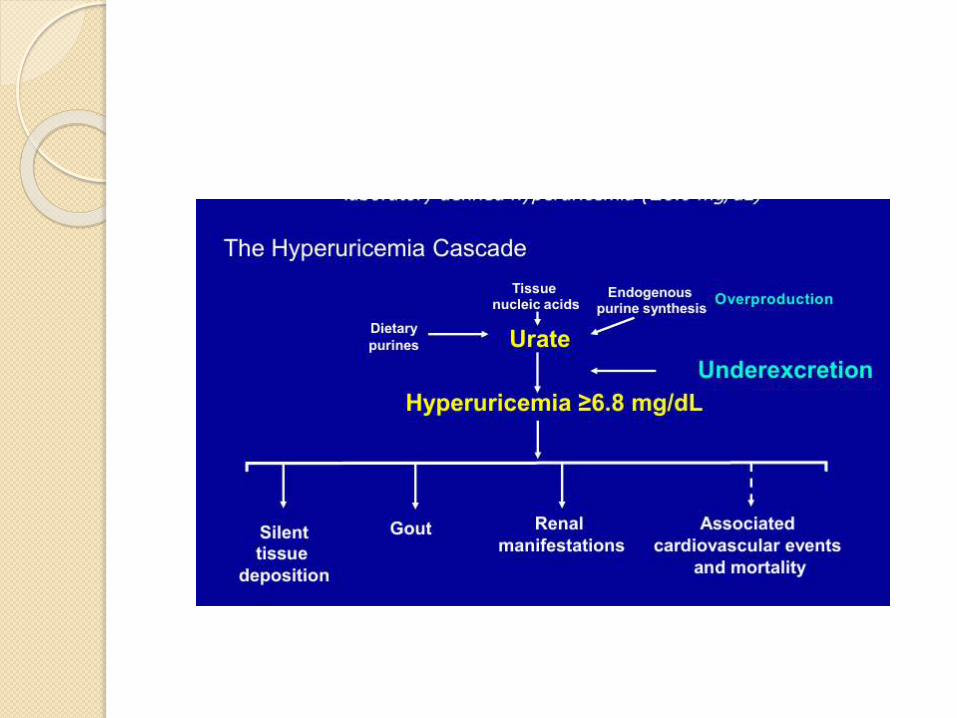
Asymptomatic hyperurecemia
Asymptomatic
Serum uric acid levels-more than
6mg/dl
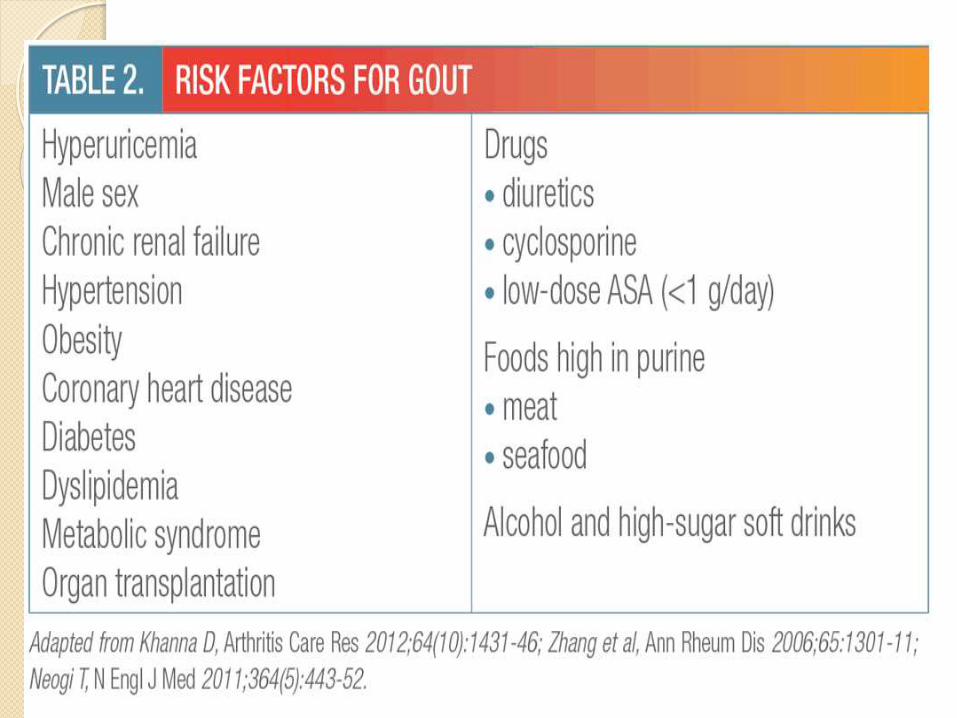
risk of gout increases with the degree
and
duration of hyperuricaemia.
Acute gout
most common early clinical
manifestation
Usually, only one joint is affected
initially, but polyarticular acute gout
can occur in subsequent episodes
Factors provking manifestations-.
alcohol,
obesity
abrupt change in serum uric acid
concentration
Diuretic use, hypertension, renal insufficiency, and
osteoarthritis
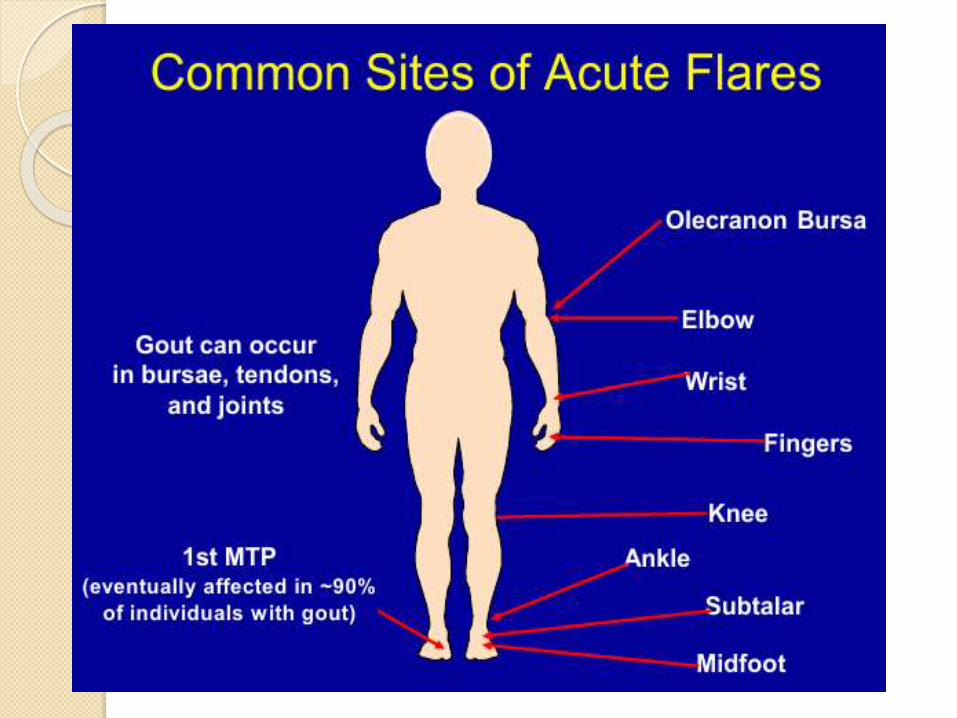
Most acute attacks of gout involve a
single joint in the lower limb,
most commonly the first metatarso
phalangeal joint also referred to as
podagra.
Others-ankle, heel, knee, wrist, fingers, and elbow joints
Symptoms-severe pain,
Swelling
Erythema
Warmth
Tenderness
Low grade fever
Starts during night peak 1-2 days.lastfor 7-10 days◦ Differential diagnosis-septic
arthritis,cellulitis
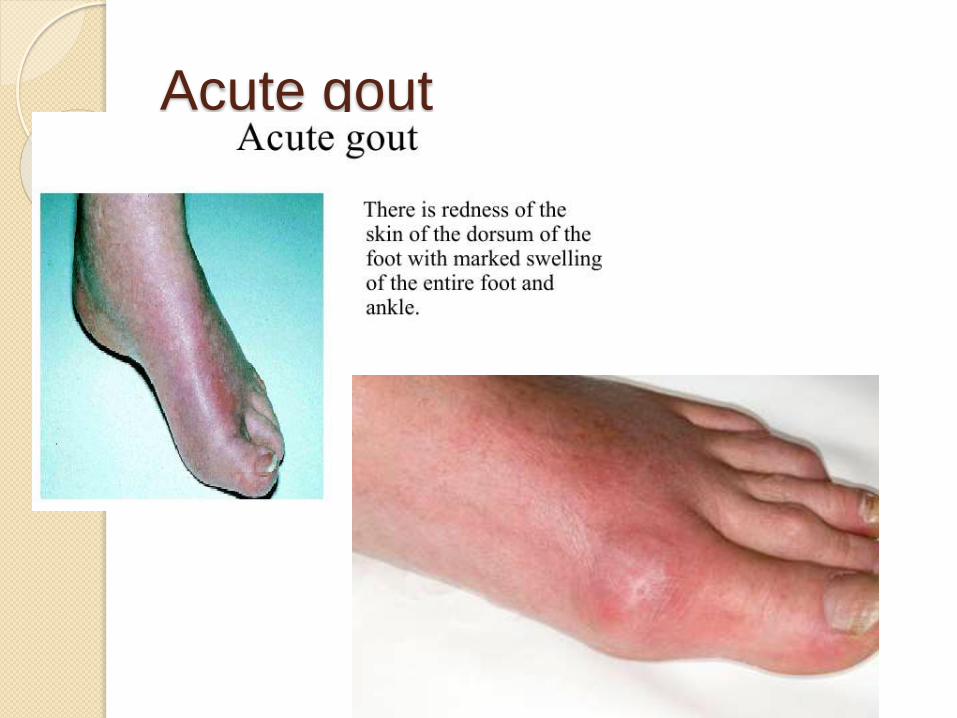
Acute gout
Intercritical gout
intercritical period is the time between
the acute attacks;
the term prophylactic period has been
preferred because its emphasizes the
value of medication which inhibits or
prevents recurring acute episodes.
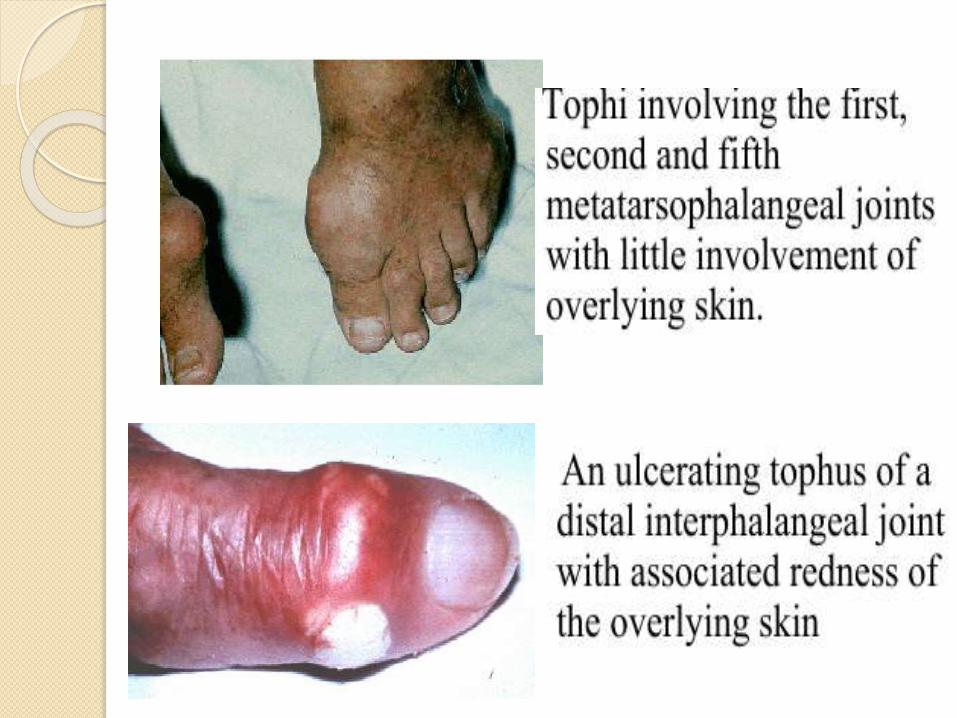
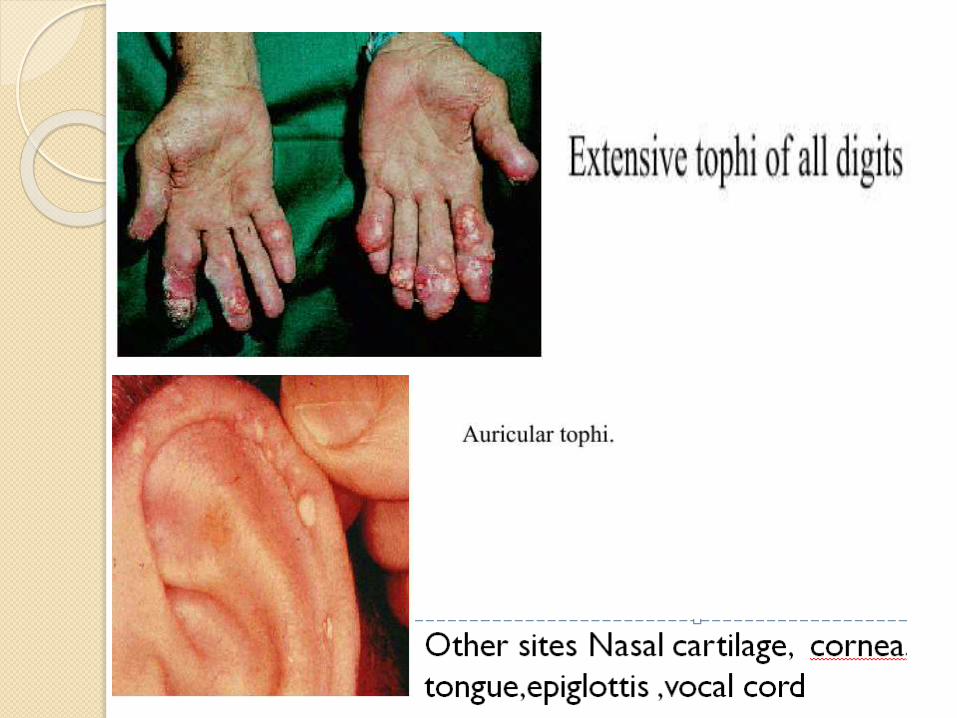
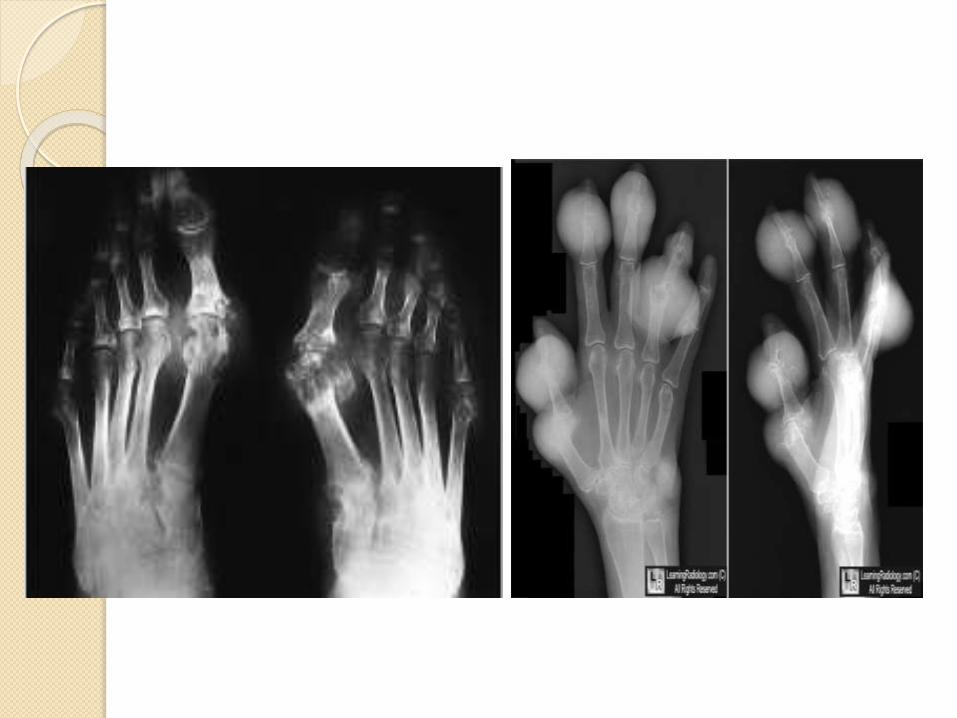
Chronic tophius gout
Massive deposition of monosodium
urate crystal(tophi) in the articular
cartilage, subchondral bone, synovial
membrane, capsular, periarticular
tissue and tendon sheaths.
Occurs late (an avg 12 yrs)after intial
attack
Chronic gout
Tophaceous nodule consist of
multicentric deposition of urate crystal
,inter cellular matrix and foreign body
grannulomatous reaction.
Tophi firm yellow in colour
occsionally discharge cheesy or
chalky white material.
+
o
Complications of tophi gout-pain,soft
tissue damage and deformity,joint
destruction, nerve compression
syndromes
Renal manifestation of gout
Nephrolithiasis
Acte gouty nephropathy
Chronic gouty nephropathy
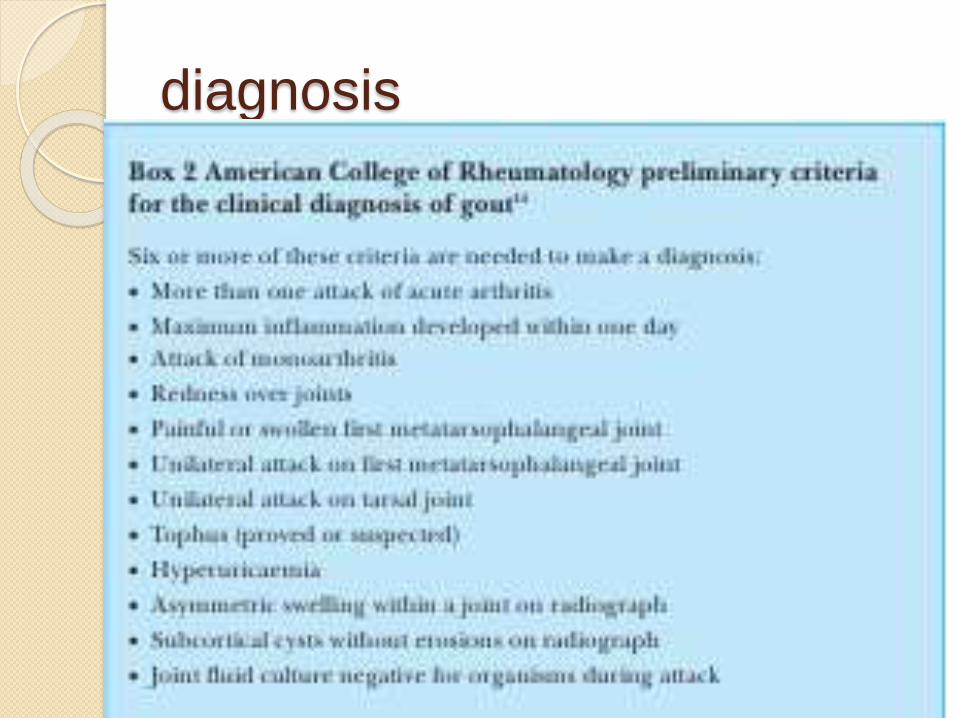
diagnosis
Base line lab tests-urine analysis
renal function tests
Serum urate- normal value is 6-7 mg/dl (6.8mg/dl)
an elevated serum uric acid level does not indicate or predict gout
hyperuricemia in the absence of symptoms is not diagnostic of gout.
diagnosed based on the discovery of uratecrystals in the synovial fluid or soft tissues.
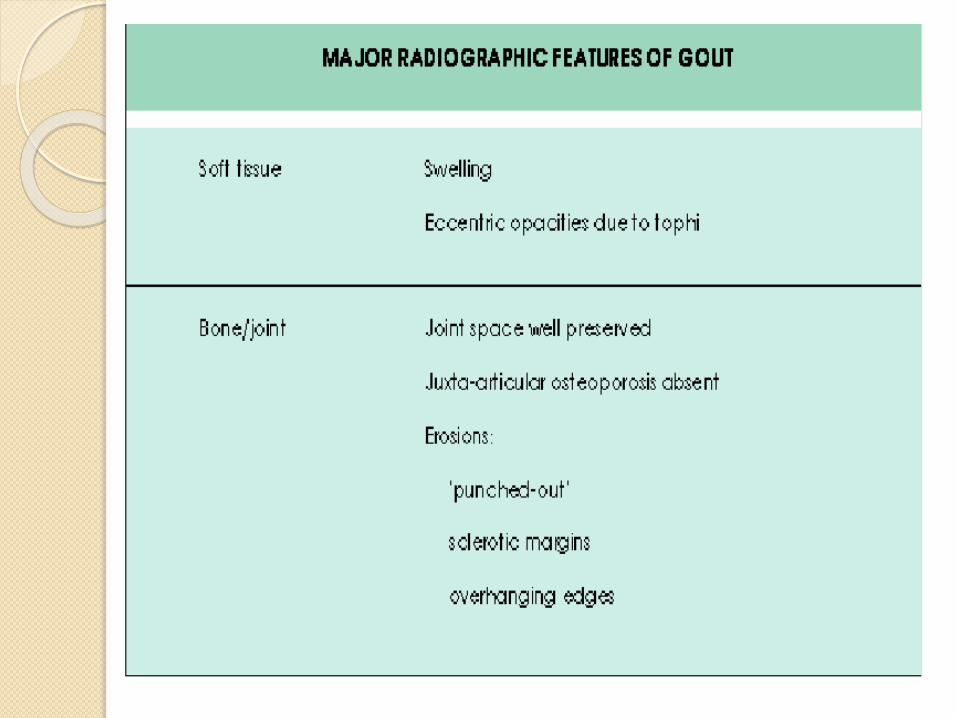
radiography
Early in the disease, radiographs are
often normal or show only soft-tissue
swelling
Radiographic findings characteristic of
gout, which generally do not appear
within the first year of disease onset
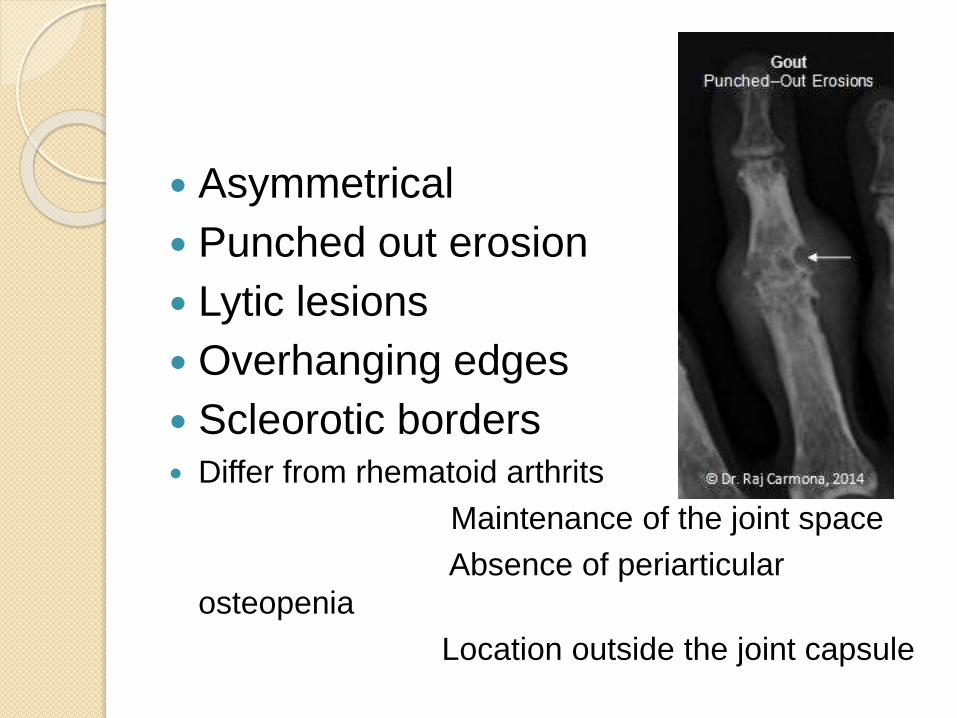
Asymmetrical
Punched out erosion
Lytic lesions
Overhanging edges
Scleorotic borders Differ from rhematoid arthrits
Maintenance of the joint space
Absence of periarticular
osteopenia
Location outside the joint capsule
identification of urate crystals the gold standard for conformation of the diagnosis
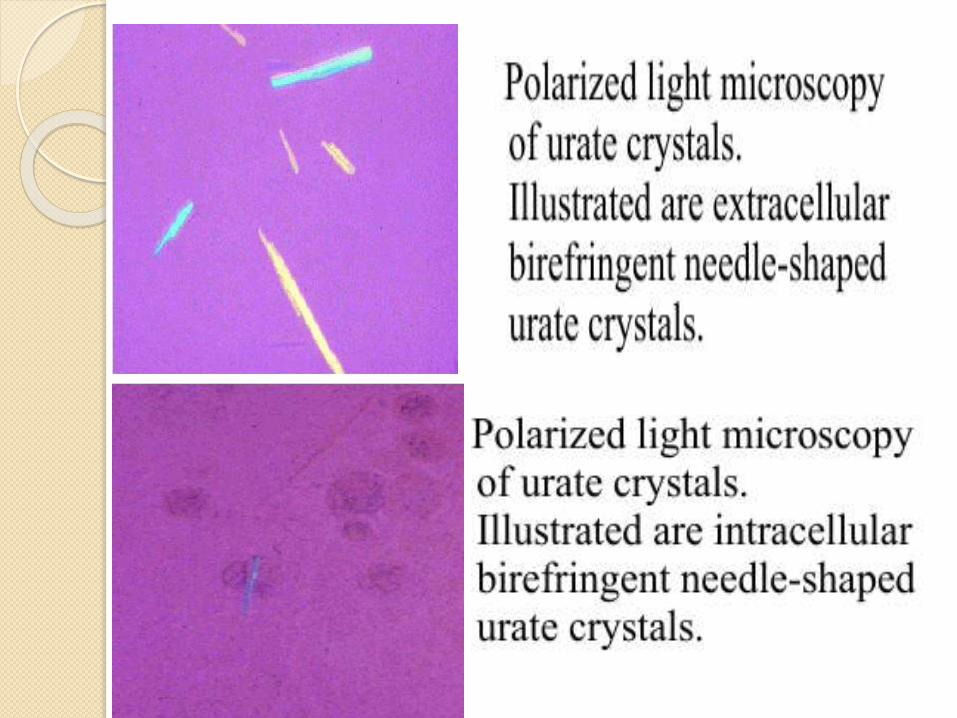
identification of urate crystals in synovial fuidusing polarized light microscopy is highly specific for gout
.
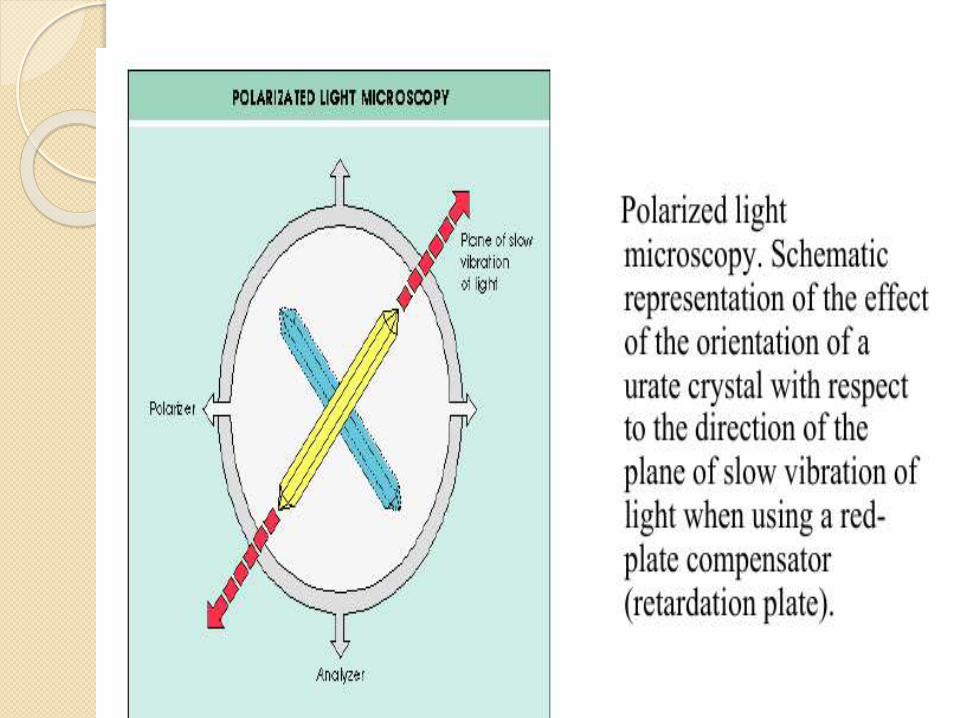
examined with a polarizing filter, they are yellow when aligned parallel to the slow axis of the red compensator, but they turn bluewhen aligned across the direction of polarization (ie, they exhibit negative birefringence).
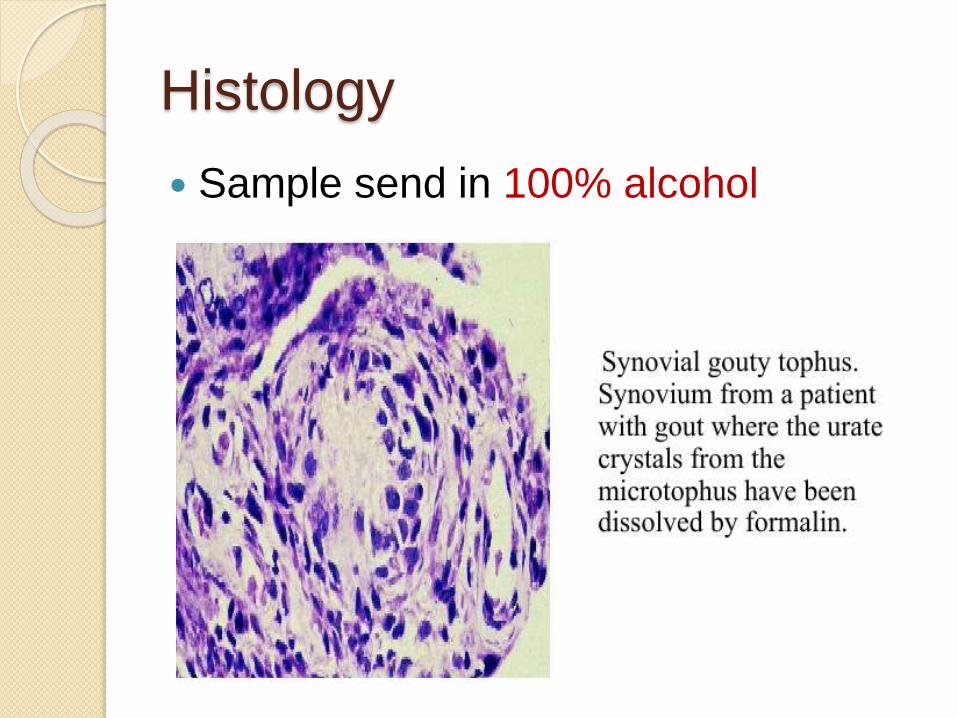
Histology
Sample send in 100% alcohol
ultrasound
A "double contour" sign, consisting of a hyperechoic, irregular line of monosodium urate crystals on the surface articular cartilage overlying an adjacent hyperechoic bony contour
"Wet clumps of sugar," representing tophaceous material, described as hyperechoic and hypoechoicheterogeneous material with an anechoic rim
Bony erosions adjacent to tophaceousdeposits
Differential diagnosis acute
gout= infective (septic) arthritis;
traumatic synovitis;
palindromic rheumatism
seronegativspond-arthritides
Rhematic fever
d Differential diagnosis of chronic
gout nodular rheumatoid arthritis;
osteoarthritis with Heberden’s /
Bouchard’snodes;
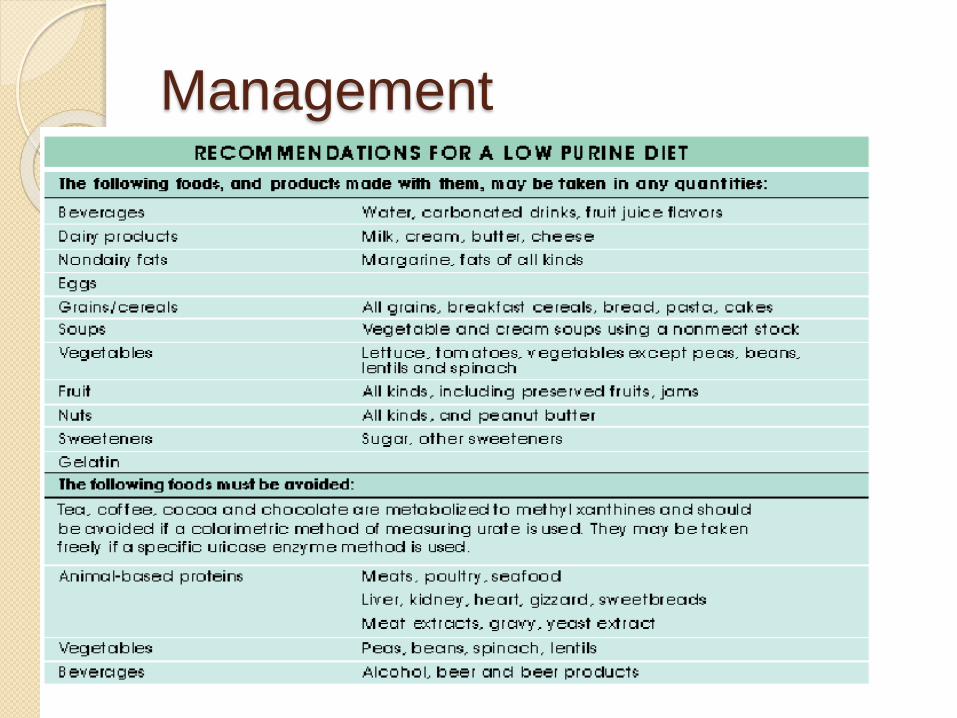
Management
Treatment The acute attack
Resting the joint
Applying ice packs if pain is severe,
NSAIDs
Colchicine (may cause diarrhoea, nausea and vomiting)
A tense joint effusion may require aspiration and intra-articular injection of corticosteroids.
Oral corticosteroids.
The sooner treatment is started the sooner is the attack likely to end.
Interval therapy
Between attacks, attention should be
given to simple measures such as
losing weight
cutting out alcohol and
Eliminating diuretics.
Chronic gout
Uricosuric drugs (probenecid or
sulfinpyrazone) can be used if renal
function is normal.
Allopurinol a xanthine oxidase inhibitor,
is usually preferred for patients with
renal complications or chronic
tophaceous gout allopurinol is definitely
the drug of choice
Urate-lowering drugs should never be
started before the acute attack has
completely subsided, and they should
always be covered by an anti-
inflammatory preparation or
colchicine, otherwise they may
actually prolong or precipitate an
acute attack.
Surgery
Ulcerating tophi that fail to heal with
conservative treatment can be
evacuated by curettage
the wound is left open and dressings
are applied until it heals.
Calcium pyrophosphate dihydrate
(CPPD) crystal associated
arthropathies
idiopathic
presents as sporadic episodes in the
majority of patient
rare familial forms
The autosomal dominant form of the disease has
been shown to be related to a mutation in the
ANKH gene, which encodes a transmembrane
inorganic pyrophosphate transport channel
association with some metabolic disorders-
hyperparathyroidism,
haemochromatosis,
hypophosphatasia,
Wilson’s disease,
ochronosis,
hypo-calciuric hypercalcaemia
diabetes mellitus
hypomagnasaemia
intra-articular injections of hyaluronic acid preparations (such as Hylan GF-20) may trigger acute attack of pseudogout
o Age is most important risk factor
Osteoarthritis (OA) - threefold increased risk if CPPD present
Previous joint trauma/injury
Joint surgery/lavage promotes crystal shedding
Incidence and prevalence uncertain
Strong association with age prevalence 3.7% in age 55-59 17% in age 80-84%
CPPD associated arthritis is third most common inflammatory arthritis
most common acute mono-articulararthritis in elderly; typically involves the knee
pathogenesis
Not known
Disorder of articular cartilage with
altered chondrocyte
cartilage matrix abnormalities,altered
activity of enzymes that produces
pyrophoshates which combines with
calcium ions to form CPPD crystals
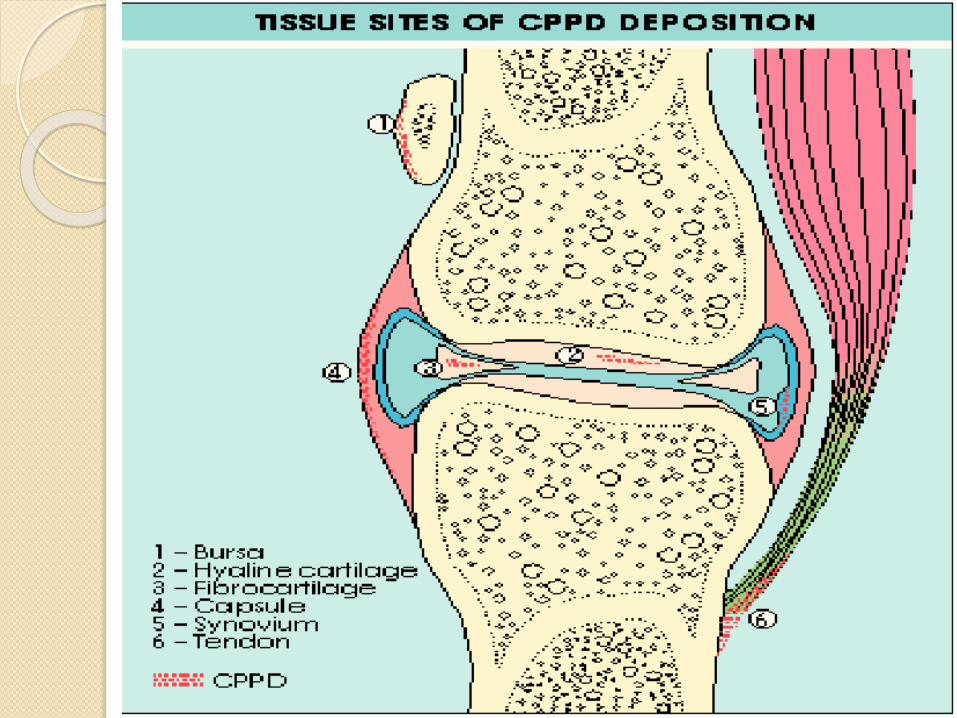
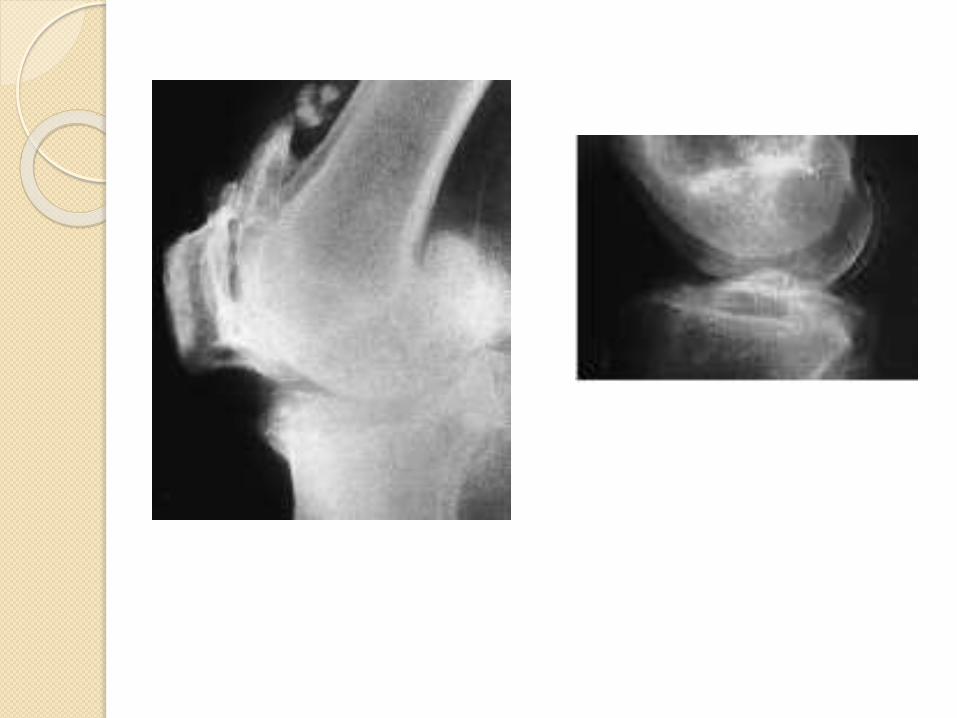
The deposits are often visible as a
fine layer of calcification overlying the
menisci and articular cartilage of the
knee- termed chondrocalcinosis
The crystals may provoke an acute attack of synovitis- referred to as pseudo-gout.
Pseudo gout Clinical syndrome of acutesynovitis with intraarticular (IA) Calcium pyrophosphate dehydrate (CPP) crystal deposition
o Most common joints knee and wrist
Chronic form referred to as calcium
pyrophosphate deposition (CPPD)
Arthropathy
Increases development of
osteoarthritis
Chondrocalcinosis
Asymptomatic
Incidental finding
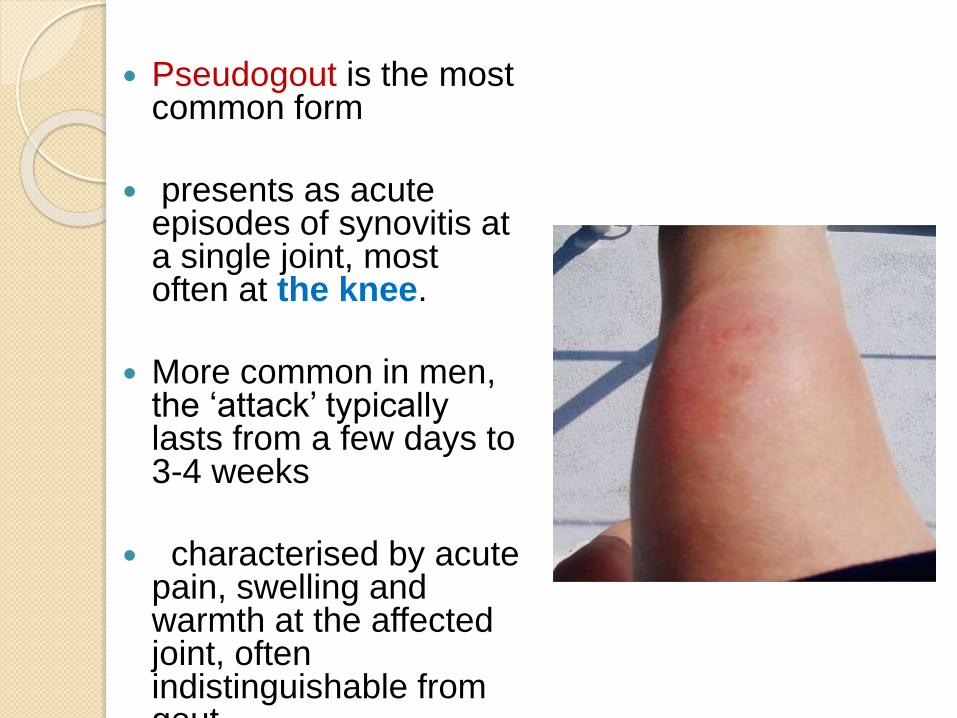
Pseudogout is the most common form
presents as acute episodes of synovitis at a single joint, most often at the knee.
More common in men, the ‘attack’ typically lasts from a few days to 3-4 weeks
characterised by acute pain, swelling and warmth at the affected joint, often indistinguishable from gout.
Chronic CPPD: predominately affects
women; it is a progressive, often
symmetric, polyarthritis.
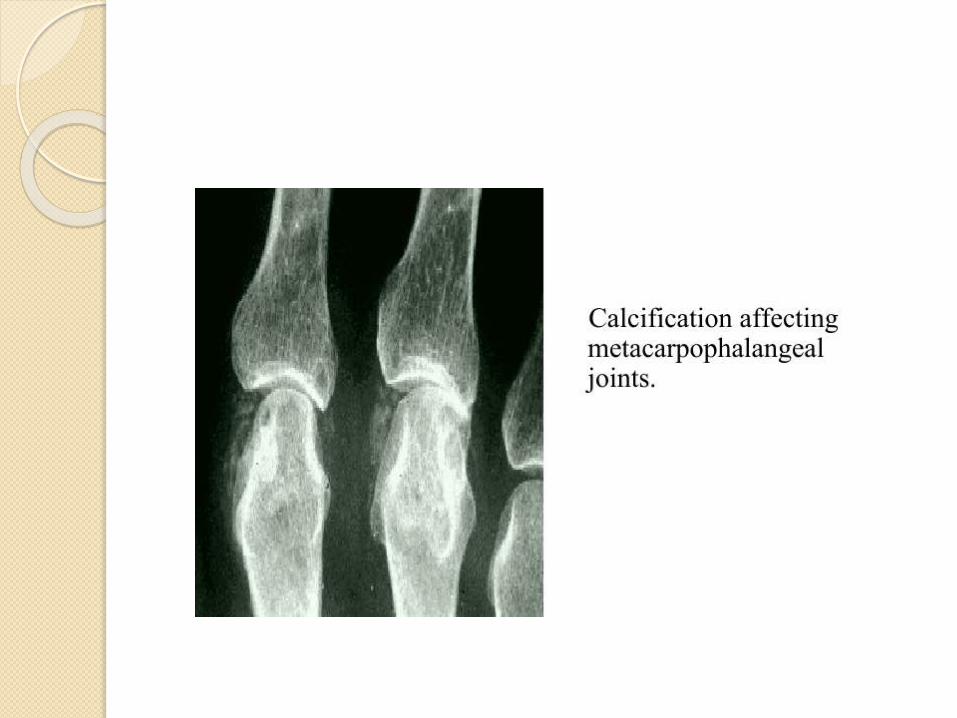
Usually affects the knees, wrists, 2nd
and 3rd MCP’s, hips, spine, shoulders,
elbows and ankles.
Chronic CPPD differs from pseudogout
in its chronicity, involvement of the
spine and MCP’s.
Radiograph of involved joint
Chondrocalcinosis (CC) = linear
densities in joints;
best seen on films of pelvis, hand and
knee
Only detects 40% articular CPPD
disease
Subchondral cysts
Aggressive joint degeneration;
osteophyte
Arthrocentesis
Inflammatory Synovial Aspirate: mean leukocyte count of 24,000 cells/μL with neutrophil predominance
Gram stain and culture necessary to rule out infectious arthritis
Screening for metabolic disorders
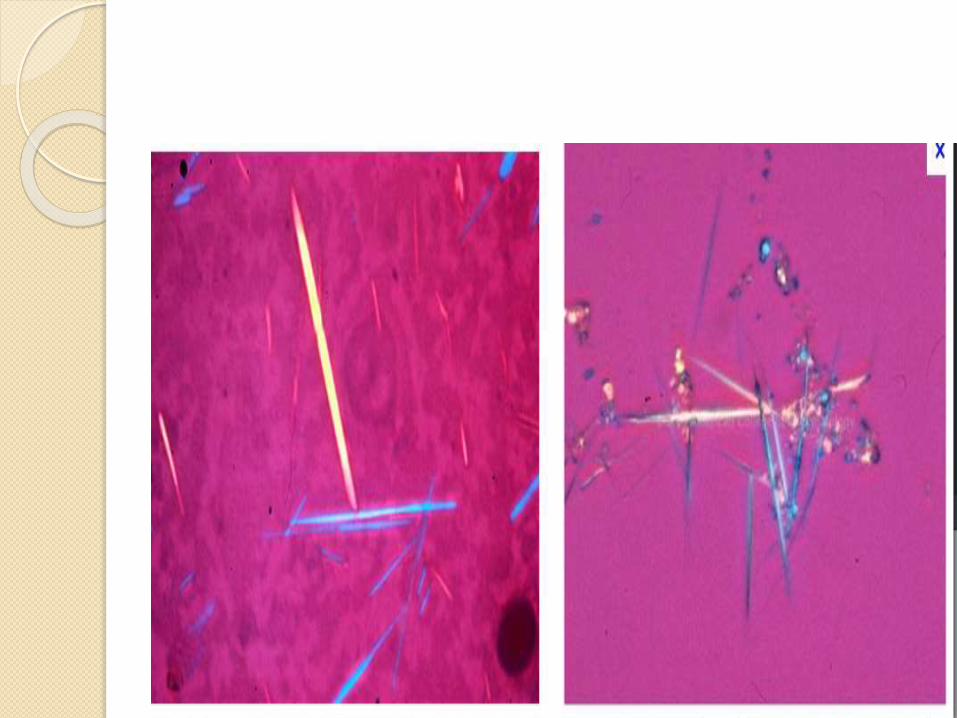
Gold standard: synovial fluid analysis under polarized light microscopy with rhomboid crystals, absent/weak positive birefringence polarizing filter
CPP crystals change color depending upon their alignment relative to the direction of the red compensator.
They are positively birefringent, appearing blue when aligned parallel with the slow axis of the compensator and yellow when perpendicular.
The sensitivity of a synovial fluid analysis for crystals is 84%, with a specificity of 100%.
Ultrasound –CPPD in peripheral joints appears as punctuate pattern with thin hyperechoic deposits
Specificity 86.7%, Sensitivity 96.4%;
Sensitivity varies with joint
Most accurate in mild cartilage degeneration
MRI - insensitive for articular CPPD
CT – sensitive for CPPD; however not specific
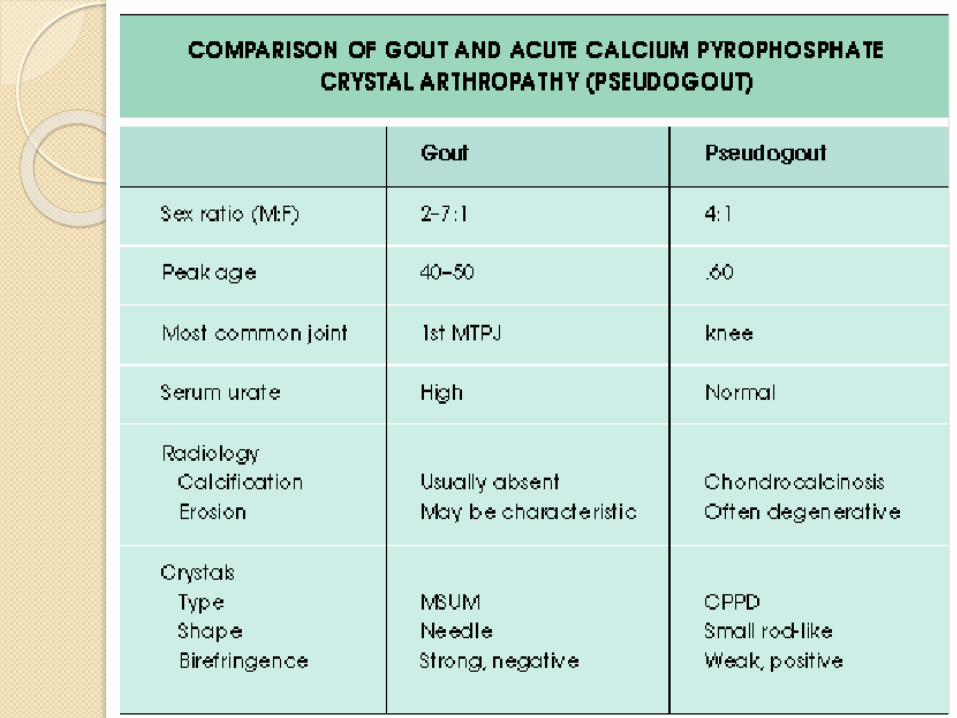
Differential diagnosis o Gout - negative birefringent monosodium urate crystals; elevated
uric
acid; first attack usually in foot
o OA: may be associated with CPPD; chronic symptoms
o RA : positive serology (Rheumatoid factor, Anti-citrullinatedpeptide
antibody) and elevated acute phase reactants;
morning stiffness;
polyarticular;
symmetric arthritis of wrist, hand or finger joints;
rheumatoid nodules; Symptoms >6 weeks
Septic Arthritis: SF analysis with turbidity, >10,000 PMNs
low glucose and elevated lactic acid;
positive Gram stain and culture
o Trauma
treatment-
o Ice
o Rest
o Joint aspiration
o Intraarticular glucocorticosteroids
o Oral Nsaids
o Cyclooxygenase-2 selective agents
o Colchicine
o Parenteral AdrenocorticotropicHormone
Prognosis
1. Acute attacks self-limited, resolve 7-10 days
2. Progressive joint damage; destructive arthropathy resembling neuropathic(Charcot’s) joints
3. Large joint arthropathy may require joint replacement
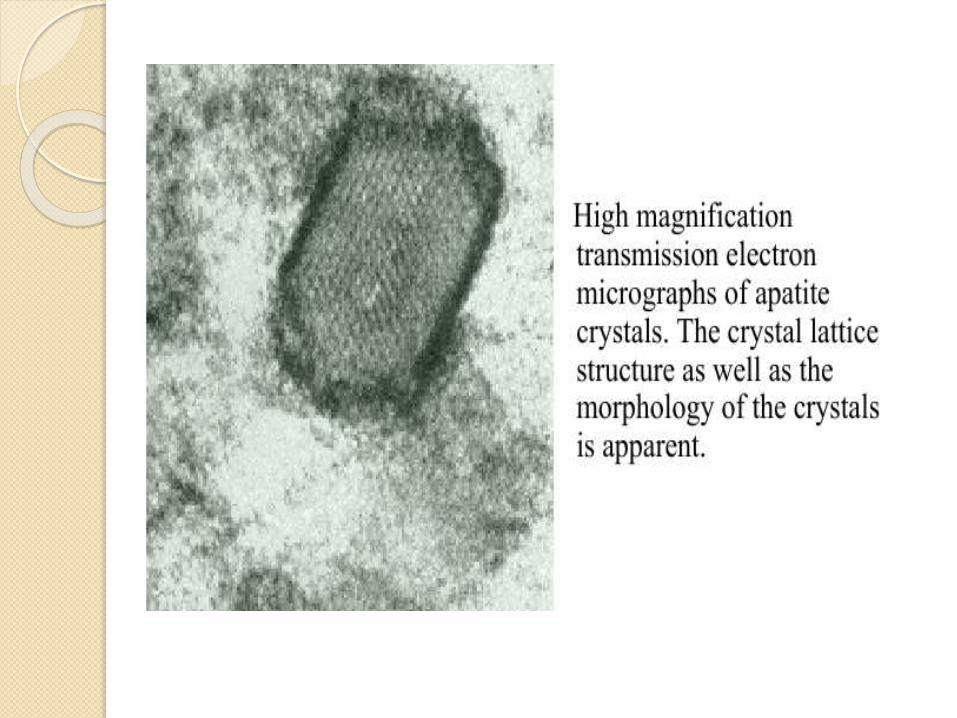
II. Basic calcium phosphate hydroxy-
apatite (BCP) crystal associated
arthropathies:
The BCP crystals includes-
hydroxy-apatite,
octacalcium
Phosphate and tricalcium phosphate
Manifestations-Periarthritis / tendonitis
Milwaukee shoulder syndrome (MSS)
Osteoarthritis
Erosive arthritis
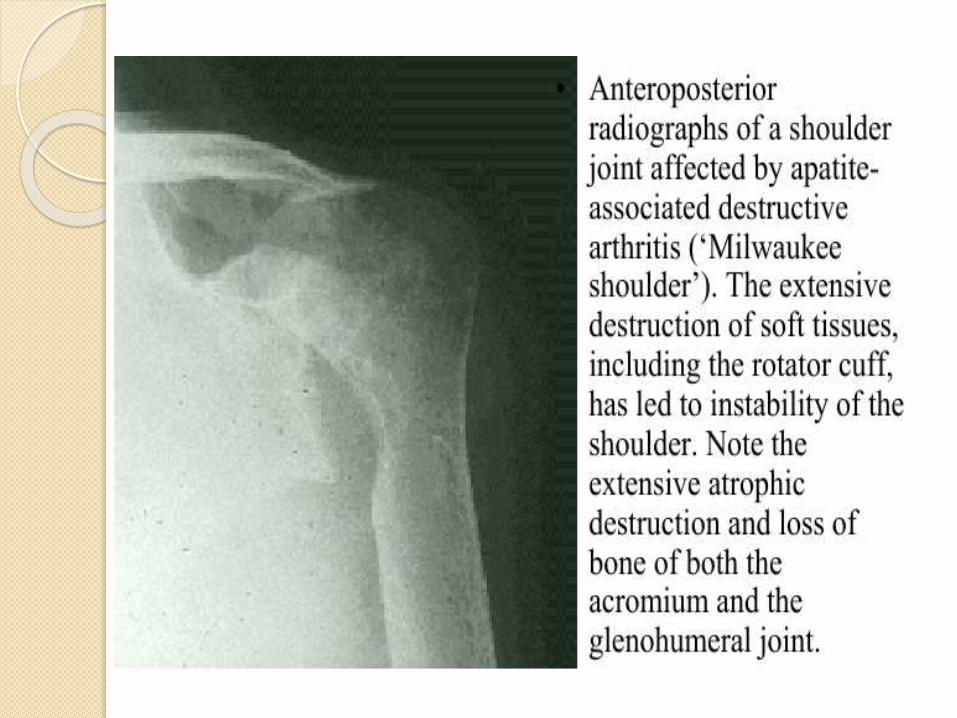
Milwaki shoulder syndrome
more common in women
affects a single joint- most often the shoulder, or the knee.
there may be a history of preceding trauma or overuse of the joint.
There are marked degenerative changes
on radiology, with the presence of loose bodies and calcification
BCP crystals is difficult and the diagnosis may
eventually depend upon excluding other causes such as gout or septic arthritis.
THANK YOU
The serum urate concentration may
reduce during an acute attack; a
normal urate concentration at this
point does not rule out a diagnosis of
gout
“Eunuchs do not take gout, nor
become
bald. A women does not take gout
unless her menses be stopped,An
young man does not take gout unless
he indulges in coitus. In gouty
affection, inflammation subsides in 40
days”
hippocrates



![MRI of Arthritisthritis [AS], enteropathic arthropathies, and psoriatic arthritis), septic arthritis, crystal-deposition and other deposition-induced arthropathies, and synovium-based](https://img.pdfslide.us/doc/110x75/5e46b77456173108910fd237/mri-of-arthritis-thritis-as-enteropathic-arthropathies-and-psoriatic-arthritis.jpg)