Embed Size (px)
Citation preview

1© Copyright L.Burchell, Gambro 2003
ContinuousRenalReplacementTherapy

2© Copyright L.Burchell, Gambro 2003
CRRT = CONTINUOUS RENAL REPLACEMENT THERAPY
Defined as
– “Any extracorporeal blood purification therapy intended to
substitute for impaired renal function over an extended period
of time and applied for
or aimed at being applied for 24 hours /day.” *
* Bellomo R., Ronco C., Mehta R, Nomenclature for Continuous Renal
Replacement Therapies, AJKD, Vol 28, No. 5, Suppl 3, November 1996

3© Copyright L.Burchell, Gambro 2003
Evolution of
CRRT
CAVHD
BSM - VPM
PRISMA
2nd Generation
extracorporeal
blood purification
system

4© Copyright L.Burchell, Gambro 2003
History of CRRT
1950’s - CRRT concept originated
1960’s - Scribner proposed CAVHD in context of ARF
1977 - Kramer introduces CAVH
1980 - Paganini introduces SCUF
1984 - Geronemus and Schneider propose CAVHD

5© Copyright L.Burchell, Gambro 2003
History of CRRT, cont’d.
1987 - Uldall introduces CVVHD
1990’s - Transition to VV therapies from AV therapies
1996 - R. Mehta, UCSD, hosts the first international conference on CRRT in San Diego

6© Copyright L.Burchell, Gambro 2003
REVIEW OF BASICS…

7© Copyright L.Burchell, Gambro 2003

8© Copyright L.Burchell, Gambro 2003

9© Copyright L.Burchell, Gambro 2003

10© Copyright L.Burchell, Gambro 2003

11© Copyright L.Burchell, Gambro 2003
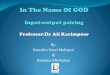
Molecular Weights
• Albumin (55,000 - 60,000)
• Beta 2 Microglobulin (11,800)
• Inulin (5,200)
• Vitamin B12 (1,355)
• Aluminum/Desferoxamine Complex (700)
• Glucose (180)• Uric Acid (168)• Creatinine (113)• Phosphate (80)
• Urea (60)
• Phosphorus (31)• Sodium (23)
• Potassium (35)
100,000
50,000
10,000
5,000
1,000
500
100
50
10
5
0
molecular weight,
daltons
}
}}
“small”
“middle”
“large”

12© Copyright L.Burchell, Gambro 2003
RIFLE Criteria

13© Copyright L.Burchell, Gambro 2003
INDICATIONS FOR CHOOSING Continuous Renal Replacement Therapy

14© Copyright L.Burchell, Gambro 2003
Clinical Indications for CRRT
Renal Indications
• Azotemia
• Fluid Overload
• Tumor lysis Syndrome
• Sepsis
• Cerebral edema
Non-renal Indications
• Metabolic Disorders
• Fluid Overload
• CPB, IABP, ECMO
• Sepsis
• ARDS
• Crush injuries
• CHF

15© Copyright L.Burchell, Gambro 2003
INDICATIONS FOR CHOOSING
Continuous Renal Replacement Therapy
Cardiovascular instability
Ongoing acidosis
Large obligatory fluid intake
Increased catabolism
Increased intracranial pressure
Sepsis ?

16© Copyright L.Burchell, Gambro 2003
Introduction to CRRT
• Continuous therapies closely mimic the native kidney in treating ARF and fluid overload
• Slow, gentle and well tolerated by hypotensive patients
• Remove large amounts of fluid and waste products over time
• Tolerated well by the hemodynamicallyunstable patient.
Why continuous therapies?

17© Copyright L.Burchell, Gambro 2003
What are we trying to achieve?
Waste removal
Electrolyte balance
Fluid balance
Acid-Base balance
Removal of septic mediators

18© Copyright L.Burchell, Gambro 2003
Advantages
Hemodynamic stability
Management of fluid overload
Control of Urea and creatinine
Nutritional support
Membrane absorption and removal of humoral mediators of sepsis

19© Copyright L.Burchell, Gambro 2003
Principles of CRRT clearance
CRRT clearance of solute is dependent on the following:
• The molecule size of the solute
• The pore size of the semi-permeable membrane
The higher the ultrafiltration rate (UFR), the greater the solute clearance.

20© Copyright L.Burchell, Gambro 2003
Replacement Fluids
Physician Rx and adjusted based on pt. clinical need.
Sterile replacement solutions may be:
• Bicarbonate-based or Lactate-based solutions
• Electrolyte solutions
• Must be sterile and labeled for IV Use
• Higher rates increase convective clearances
• You are what you replace

21© Copyright L.Burchell, Gambro 2003
Continuous Renal Replacement Therapy
SCUF Slow Continuous Ultra-Filtration
CVVH Continuous Veno-Venous Hemofiltration
CVVHD Continuous Veno-Venous Hemodialysis
CVVHDF Continuous Veno-Venous Hemodiafiltration

22© Copyright L.Burchell, Gambro 2003
Renal Recovery?
CRRT does affect resumption of function.

23© Copyright L.Burchell, Gambro 2003
By avoiding hypotensiveepisodes, the risk of further kidney damage is reduced and the chance for renal recovery is enhanced

24© Copyright L.Burchell, Gambro 2003
30610
0135
0
.2
.4
.6
.8
1
0 20 40 60 80 100
IRRT
CRRT
days
Recovery from Dialysis Dependence: BEST Kidney DataR
ecovery
fro
m d
ialy
sis
dependence
Manuscript under review
Leading the way…

25© Copyright L.Burchell, Gambro 2003
CRRT vs. IHD in Renal Recovery
Recent studies suggest that CRRT is superior to IHD with respect to recovery of renal function
Implications go far beyond just “hard” endpoint of renal recovery
• Need for chronic dialysis impairs quality of life
• If length of stay (LOS) in ICU can be reduced this will have a major impact on hospital budget
• Patients dependent on chronic dialysis will consume significant health care resources and have an impact on the community health care budget

26© Copyright L.Burchell, Gambro 2003
Access Location
Internal Jugular Vein
• Primary site of choice due to lower associated risk of complication and simplicity of catheter insertion.
Femoral Vein
• Patient immobilized, the femoral vein is optimal and constitutes the easiest site for insertion.
Subclavin Vein
• The least preferred site given its higher risk of pneumo/hemothorax and its association with central venous stenosis

27© Copyright L.Burchell, Gambro 2003
Advanced therapy
• Therrapeuticplasma exchang
TPE• HemoperfusionHP

28© Copyright L.Burchell, Gambro 2003
THANK YOU