Embed Size (px)
Citation preview
What's the relationship?
Case A 25 YRS old male presented with central abdominal pain associated with low grade fever And intermittent attacks of diarrhrea that come and go in a weekly pattern . The pt. was anorexic and metioned a gradual weight loss over the past few months . also the pt. is smoker since
he was 17 .

Case discussed
A 25 YRS old male presented with central abdominal pain associated with low grade fever And intermittent attacks of diarrhrea that come and go in a weekly pattern . The pt. was anorexic and metioned a gradual weight loss over the past few months . also the pt. is smoker since
he was 17 .
! Lets go DDX
Bacterial enteritis Viral enteritis Ulcerative colitis Tumor Crohn's disease
So what's the approach?? Full history : the pain questions , diarrhea , stool
characteristics , family Hx of similar condition, social habits including smoking .
Clinical examination Lab investigations : complete blood picture showed ( megaloblastic anemia?) elevated ESR and CRP , folic acid and Cu defeciency GSE for presence of bacteria . Stool occult blood test
Approach
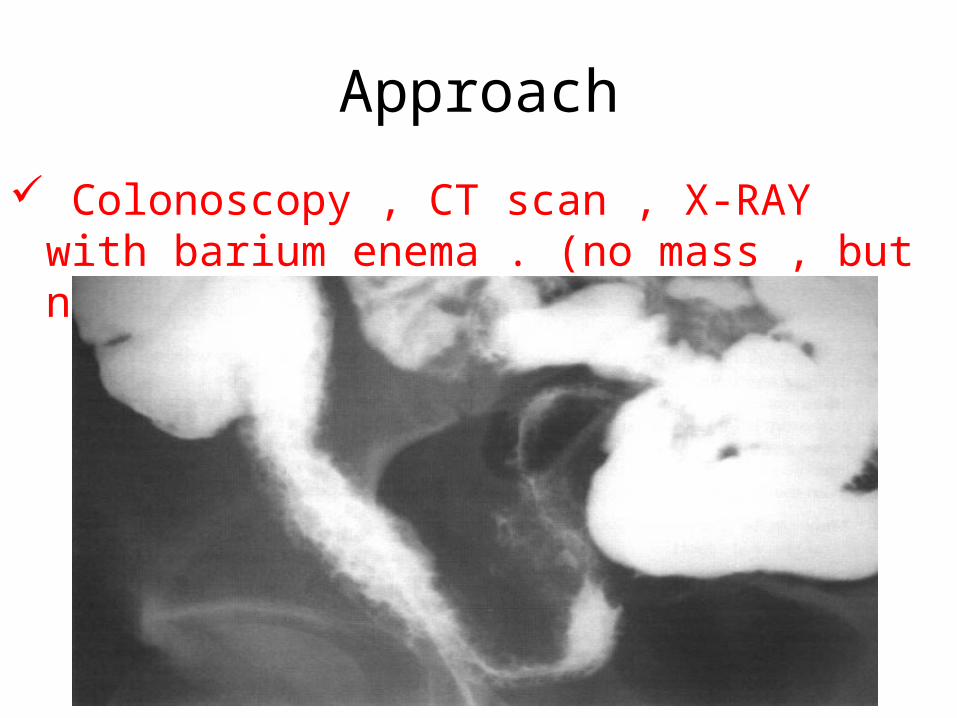
Colonoscopy , CT scan , X-RAY with barium enema . (no mass , but narrowing of bowel lumen)
inflammation
Edema and
fibrosis
Narrowed lumen
Of the wall of intestine
ATENDOSCOPY
(if possible)
What to see ?? • Mucosa : small ulcers coalesce to
form long serpentine linear ulcers . The mucosa between the ulcers is inflamed and edematous , having a cobble-stone appearance .
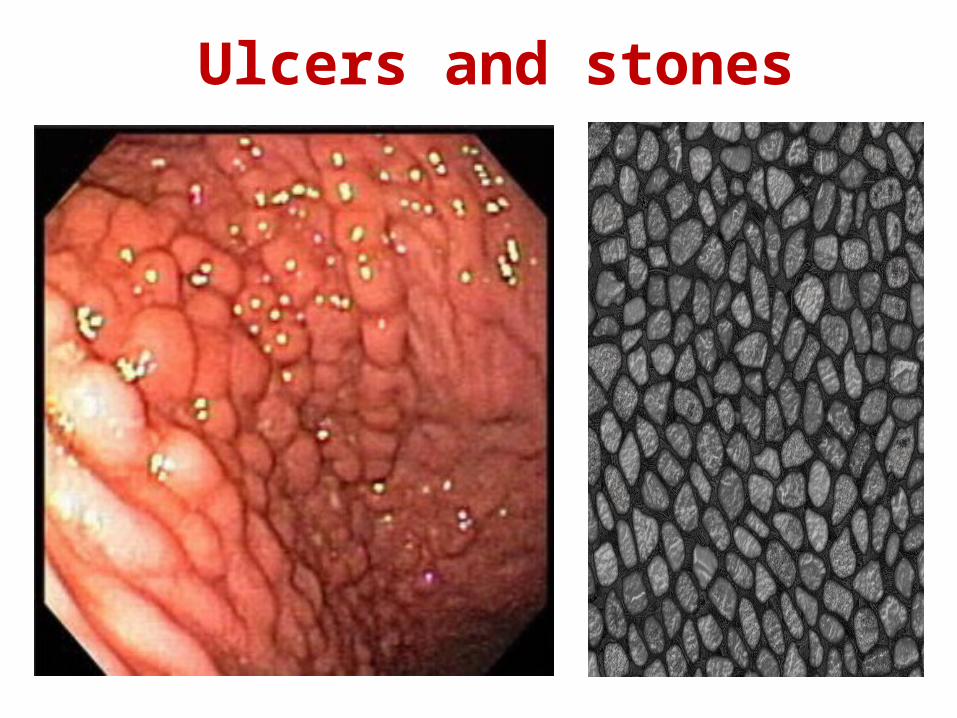
Ulcers and stones
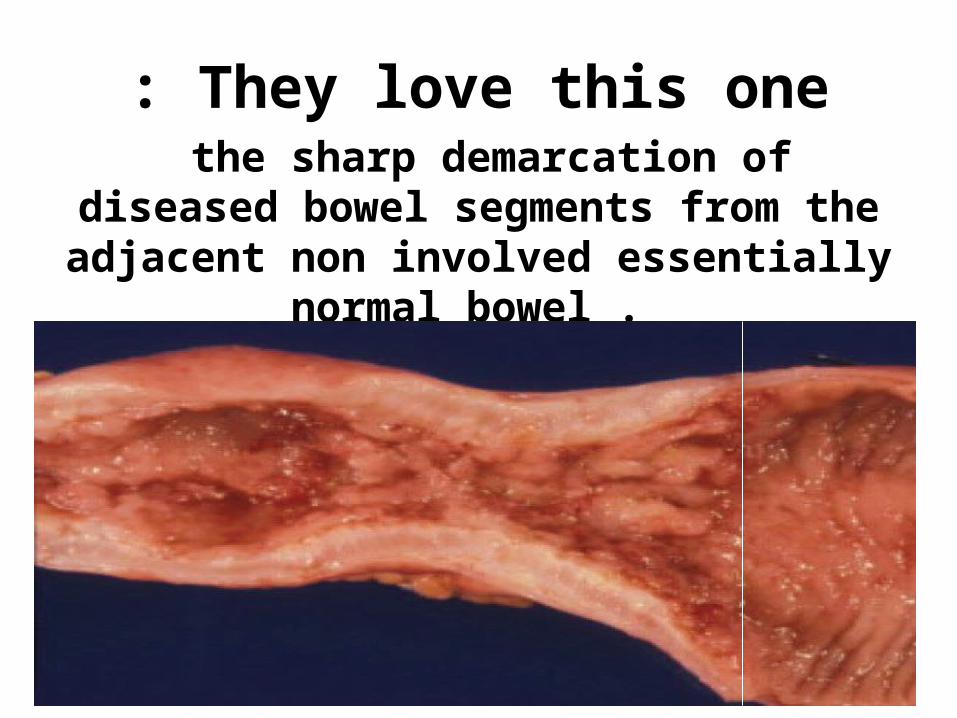
They love this one: the sharp demarcation of diseased bowel segments from the adjacent non involved
essentially normal bowel .
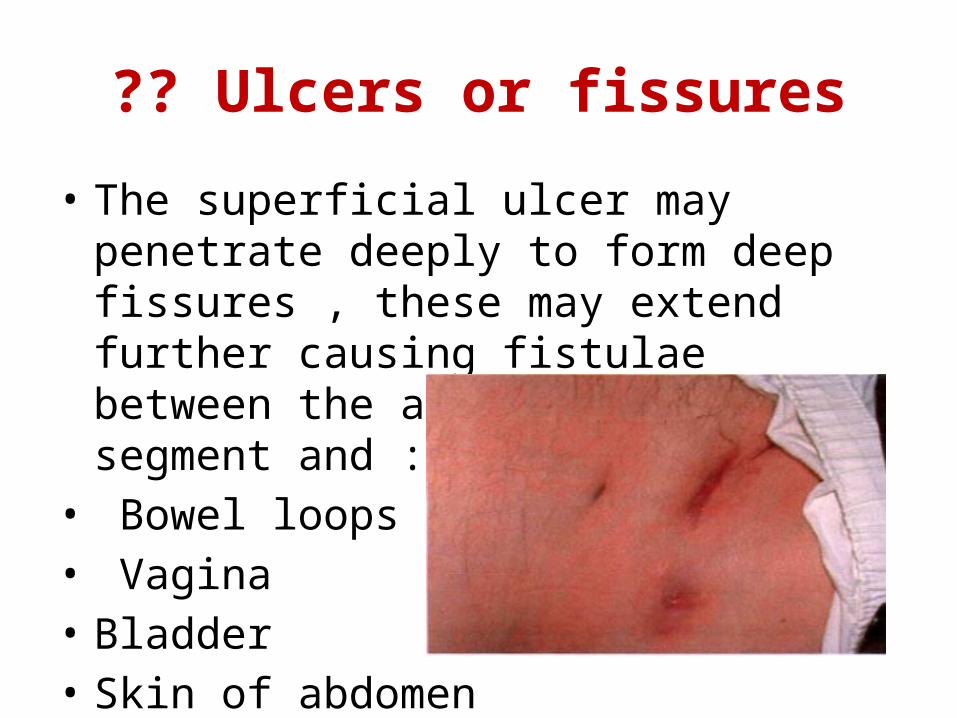
Ulcers or fissures?? • The superficial ulcer may penetrate deeply to
form deep fissures , these may extend further causing fistulae between the affected intestinal segment and :
• Bowel loops• Vagina • Bladder • Skin of abdomen
Biopsy taken for
bacteriologic and
pathologic studies
The Bx results
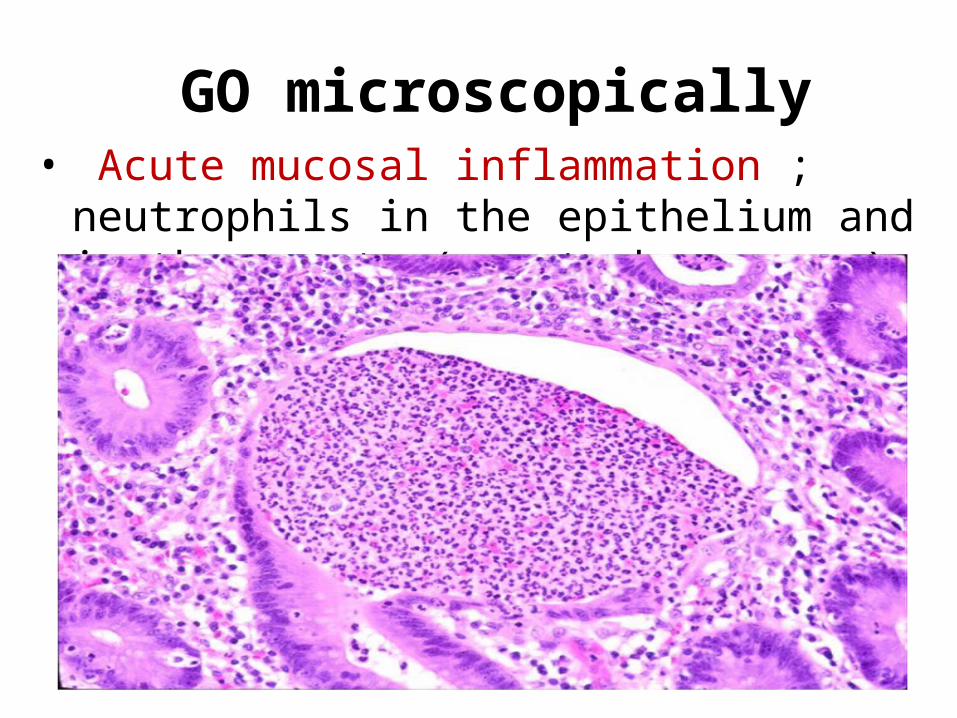
GO microscopically • Acute mucosal inflammation ; neutrophils in the
epithelium and in the crypts (crypt abscesses )
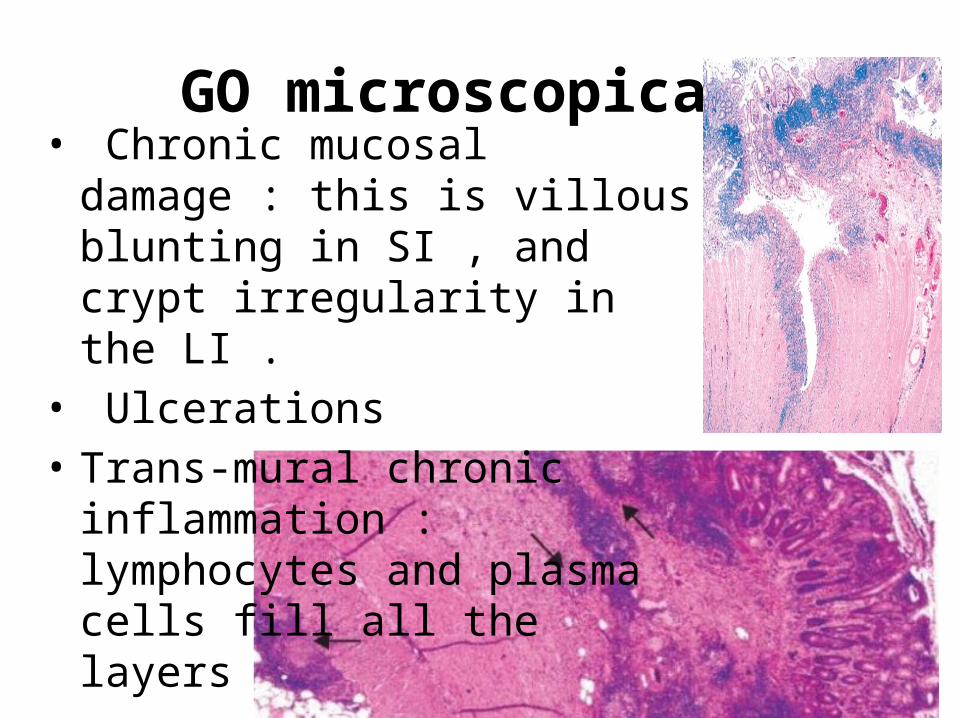
GO microscopically • Chronic mucosal damage : this is
villous blunting in SI , and crypt irregularity in the LI .
• Ulcerations• Trans-mural chronic inflammation :
lymphocytes and plasma cells fill all the layers
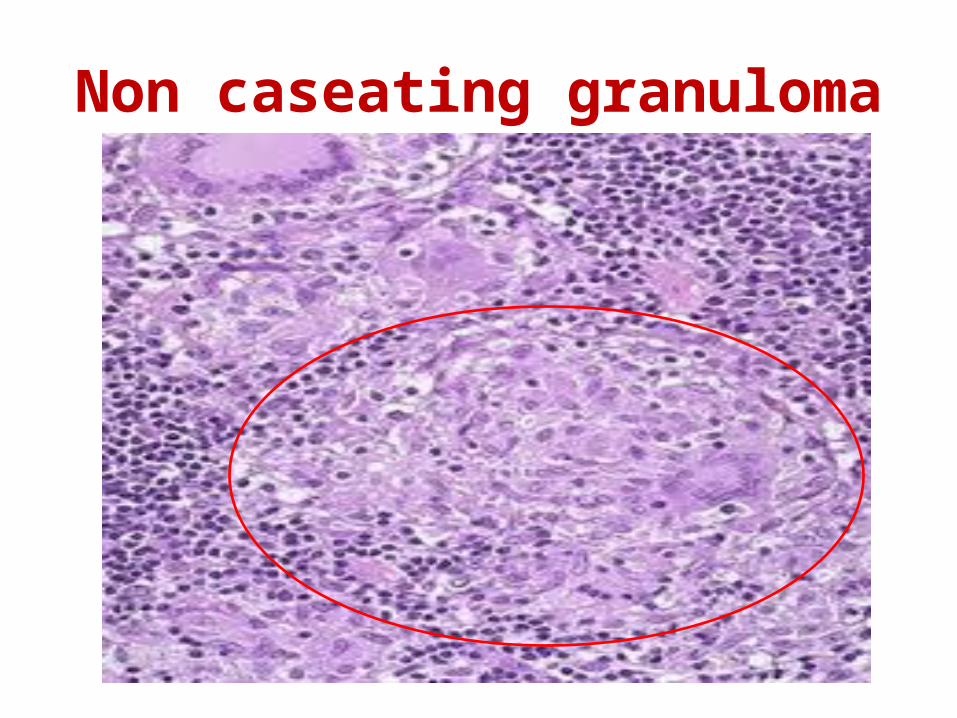
Non caseating granuloma
GO microscopically
• Other changes ; duplication and thickening of musc. mucosae. And also fibrosis of submucosa , musc. Propria and serosa .
• Dysplastic changes in the mucosal epithelial cells : this is imp. In long standing disease , may be focal or widesprad , increase with time
this increases the risk of CA . Esp. that of colon

C / F• Colicky abdominal pain • Intermittent attacks of diarrhea • Fever lasting weeks or months • Anorexia , Wt loss • Anemia in colon involvement
Complications of Crohn's • Fibrosing strictures : causing intestinal
obstruction ( symptoms ?)• Fistulae to ; normal bowel , vagina , bladder• Extensive involvement of small intestine :
causing protein losing enteropathy , pernicious anemia (?) , steatorrhea (?) and generalized malabsorption .
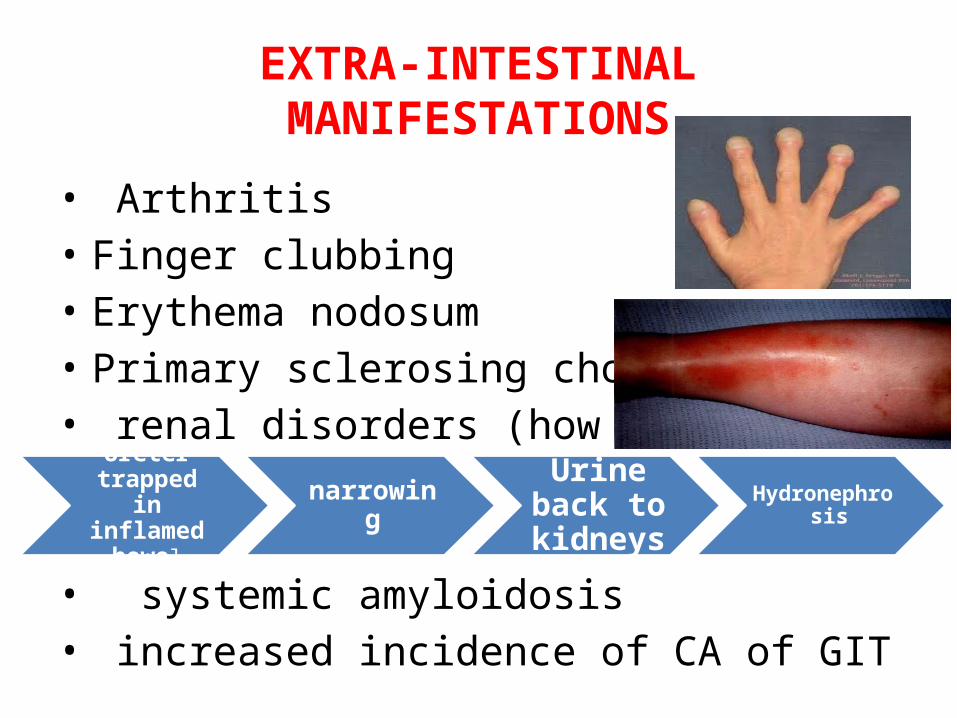
EXTRA-INTESTINAL MANIFESTATIONS
• Arthritis • Finger clubbing• Erythema nodosum• Primary sclerosing cholangitis• renal disorders (how ?)
• systemic amyloidosis • increased incidence of CA of GIT
Ureter trapped in inflamed
bowel
narrowingUrine
back to kidneys
Hydronephrosis

Cigarette smoking is a risk factor for Crohns DR, Bernard Crohn
Clubbing is an extra intestinal manifestation
for CrohnsCobble stone pavements

THANK YOU