Embed Size (px)
DESCRIPTION
A review of fundamental critical care concepts Edward Omron MD, MPH, FCCP Pulmonary, Critical Care Medicine Morgan Hill, CA 95037
Citation preview

Critical Care Concepts
Edward Omron MD, MPH, FCCP
Pulmonary and Critical Care

INDICATIONSINDICATIONS
• ABG– Oxygenation– Ventilation– Acid-Base Status
• VBG– Ventilation and Acid-Base Status
– Cardiac Output (venous arterial PCO2 difference)
– Endpoint of resuscitation (ScvO2 and PCO2)

Blood Gas Report(Blood Gas Report(ArterialArterial))
• pH (No Units) 7.35-7.45
• PaCO2 (mm Hg) 35-45
• PaO2 (mm Hg) 110 - 0.5(age)
• HCO3- (mmol/L): calc. 22-26
• B.E. (mmol/L) -2 to 2
• O2 saturation: calc. >90%

Blood Gas ReportBlood Gas Report(mixed/central venous)(mixed/central venous)
• pH = 7.32-7.42
• PvCO2 = 40 - 50 (mm Hg)
• PvO2 = 36 - 42 (mm Hg)
• Oxygen Saturation > 70%
• Base Excess = -2 to +2


ANALYSIS OF VENTILATONANALYSIS OF VENTILATON
• PaCO2 = VCO2 x K
VA
Hypercapnea > 45 mm Hg (Hypoventilation)
Respiratory Acidosis
Hypocapnea < 35 mm Hg (Hyperventilation)
Respiratory Alkalosis

Respiratory Acid-Base Status
• Respiratory Disturbances– CO2+H20 H2CO3 H+ + HCO3
– Acute changes:• Delta 10 mm Hg PaCO2, pH changes by 0.08• Chronic change: 40 + B.E
– Alveolar Ventilation• VA CO2 pH
• Respiratory Acidosis pCO2 > 45• Respiratory Alkalosis pCO2 < 35

BASE EXCESS(B.E.)BASE EXCESS(B.E.)
• Positive value, excess base, metabolic alkalosis
• Negative value, excess acid, metabolic acidosis
• Metabolic component of acid-base status
• PCO2 independent
• Estimated by BE = (Total CO2 – 24)

Problem Solving
1. LOOK AT THE pH– Whatever side of pH 7.4 is the primary disorder
2. Look at pH, PCO2 direction
– Both decrease or increase, then metabolic– If move in opposite directions, respiratory
3. Respiration: acute or chronic?– Acute: 10 mm Hg / 0.08 change in pH– Chronic: 40+Base Excess

• Calculate the Adjusted Anion Gap– High vs normal ANG differential– Adjusted ANG = ANG + 2.8(4.4 -Albumin)

Arterial Draw:• pH = 7.28, PaCO2 = 34, HCO3 = 16
• Na = 153 Cl = 106 Total CO2 = 17
• Alb = 3 g/dL, Saturation = 84%
• Primary Acid-Base Disturbance?
• Adjusted ANG
• Metabolic Acid-Base Status
74 yo male found unresponsive and pulseless

• Primary Disorder– Acidosis and acidemia (pH < 7.4)
• pH and PCO2 direction– Both down: Metabolic Acidosis
• Base Excess– 16 – 24 = -8 mmols/L
• Adjusted Anion Gap– ANG + 2.8*(4.4 - 3) or 30 + 4 = 34 – Anion Gap Acidosis
• Compensation? – 40 + BE or 32 mm Hg

Venous Draw
• pH = 7.08, pCO2 = 75, HCO3 = 21
• Na = 145, Cl = 103, Total CO2 =22
• Alb = 3 g/dL, Saturation = 20%
• Primary Acid-Base Disorder?
• Adjusted ANG?
• Metabolic Acid-Base Status?

• Primary Disorder– pH < 7.4, acidosis and acidemia
• pH and PCO2 direction– Opposite therefore RESPIRATORY acidosis
• Base Excess
– 22 – 24 = -2 mmol/L
• Adjusted Anion Gap– ANG + 2.8(4.4 -3) = 20+4 =24– Anion Gap Acidosis
• 40 + BE rule Comp in VBG

74 yo male found unresponsive and pulseless
• Why a metabolic acidosis in arterial bed and respiratory acidosis in venous bed?– Venous arterial PCO2 difference?– PvCO2 (75) - PaCO2 (34) = 41– PvCO2 – PaCO2 1 / cardiac index– Normal ≤ 6 mm Hg
• Venous vs Arterial saturation difference?– PaO2 = 50 mm Hg, saturation = 84%– PvO2 =18, Venous Saturation = 20%– Increased oxygen extraction from circulatory
failure

PaO2 vs PvO2 in Cardiogenic Shock
Arterial Venous Saturation Difference
SHOCK

Effects of Cardiac Output on Arterio-venous Difference
• VO2 = 1.34*Hgn*10*C.O.*(SaO2 –SvO2)
• VO2 = 1.34*Hgn*10* C.O.* (SaO2 –SvO2)
– A decrement in C.O. must be accompanied by an increase in the arteriovenous difference at constant oxygen consumption

A fall in venous saturation from 70% to 50% represents A fall in cardiac index of 42%

Paradoxical Respiratory Acidosis of Cardiopulmonary Arrest
Venous Arterial CO2 Difference

Central Venous-Arterial PCO2 Gradient

Fick Equation for CO2 production
• VCO2 =Carbon dioxide production (200 mL/min)
• VCO2 = 10*C.O.*(PvCO2 – PaCO2)
• If cardiac output decreases and VCO2 remains constant, what must happen to venous-arterial CO2 difference?
• VCO2 = 10* C.O.* (PvCO2 – PaCO2)
• Respiratory Quotient VCO2/VO2 = 200/250 = 0.8

Venous Arterial CO2 Difference
• Circulatory Failure– Associated with Tissue Hypercarbic Acidosis– Hypovolemia, sepsis, shock …
• Cardiac Index = e (1.787 – 0.151(v-a CO2))
– Endpoint of Resuscitation
• PvO2 or SvO2 from VBG– Enpoint of Resuscitation

Cardinal Rules of Critical Care– GOLDEN HOUR GOLDEN HOUR
• Time dependent functionTime dependent function
– Maximize Oxygen Delivery• Improve Cardiac Performance
– Maintain MAP > 65 mm Hg (arbitrary)
» Preload Augmentation (crystalloid/colloid)
» Inotropes (norepinephrine)
» Peripheral vasoconstrictor (vasopressin)
• Transfuse Packed Red Blood Cells
• Assume control of ventilation/oxygenation– FIO2 factors

Cardinal Rules of Critical Care
– Minimize oxygen consumption• Sedation, analgesia, rarely neuromuscular
blockade
• Work of breathing
• Fever
• Rigors
• Pain
• Anxiety

Endpoint of Resuscitation
• Conventional Endpoints are lagging indicators of inadequate oxygen delivery– Blood Pressure– Heart Rate– Urine Output– Mental Status Changes– Central Venous Pressure (poor surrogate of
filling pressures)

• More effective endpoints of resuscitation
• Continuous Cardiac Index– Pulse pressure variation
– Systolic pressure variation
• SvO2 or ScvO2
• Serum lactate (Tissue hypoxia
• Venous – arterial PCO2– Directly correlates with cardiac index
• Metabolic acid-base status (SBE)

Resuscitation Endpoints
• A single set of data points is useless– C.I., SvO2, PaCO2-PvCO2, SBE, Lactate
• Construct multiple data points to assess trends and response to interventions!
• REAL time bedside interventions

Pulse Pressure Variation

Systolic Pressure Variation

Preload Augmentation
RVEDV or LVEDV
Stroke Volume
Normal
Abnormal (Cardiogenic or septic shock)
50 mL 100 mL 150 mL

Preload Augmentations/p fluid bolus
RVEDV or LVEDV
Stroke Volume
Normal
Abnormal (Cardiogenic or septic shock)
50 mL 100 mL 150 mL 200 mL

Stroke Volume
Ventricular preload
preload-dependencepreload-dependence
preload-independencepreload-independence
The lower the ventricular preload, The lower the ventricular preload, the more likely the preload-dependency the more likely the preload-dependency

.
Stroke volume
Ventricular preload
normal heart normal heart
failing heart failing heart
preload-dependencepreload-dependence
preload-independencepreload-independence

Preload Augmentation
• DO2 (oxygen delivery in mL O2/min)
• DO2 = CO x CaO2 x 10
• DO2 = HR x SV x CaO2 x 10
• DO2 = HR x SV x Hb x SaO2 x 13.8

Central Venous Oxygen Saturation ScvO2
• Allows separation of early and late shock
• Easily measured with venous blood gas
• Surrogate measurement of mixed venous oxygen sat.– 5-18% higher– A low ScvO2 always means a low SvO2!
• Normal ScvO2 68-76%
– 25% extraction coefficient of normal physiology


Fick Equation for Oxygen Consumption
• VO2= Oxygen Consumption (250 mL/min)
• VO2 = 10*C.O.*(CaO2 –CvO2)
• VO2 = 10 * C.O. * (1.34*Hgn*SaO2 -1.34*Hgn*SvO2)
• VO2 = 1.34*Hgn*10*C.O.*(SaO2 –SvO2)
• Solve for SvO2?

Four Determinants of Central Venous Oximetry
ScvOScvO22 SvO SvO22 = SaO = SaO2 2 - (VO - (VO22 / C.O. x Hgb x 1.34) / C.O. x Hgb x 1.34)
ScvO2 = Central venous saturation (%)
SvO2 = Mixed venous saturation (%)
SaO2 = Arterial oxygen saturation (%)
VO2 = Oxygen consumption mL (O2/min)
Hgb = Hemoglobin concentration (g/dL)Cardiac Output (C.O.) = dL/min

Master EquationMaster Equation
ScvO2ScvO2 SvO2 = SaO2 - (VO2 / C.O. x Hgb x SvO2 = SaO2 - (VO2 / C.O. x Hgb x 1.34)1.34)
• Acute Illness or Post-op Surgery– SaO2, VO2, Cardiac Output, and Hgb are
dynamically changing concurrently
– Optimize each parameter then recheck ScvO2 to assess response to intervention

Effect of changes in PaO2 on SvO2
600200
10080
60
40
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 100 200 300 400 500 600 700
PaO2 (mm Hg)
SvO
2
SvO2

Effect of changes in Hgn on SvO2
13
10
7.5
5
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0 2 4 6 8 10 12 14
Hemoglobin (g/dL)
Sv
O2
SvO2

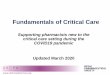
The Effects of Cardiac Output on SvO2
0.870.83
0.73
0.66
0.55
0.31
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 2 4 6 8 10 12
Cardiac Output (L/min)
Sv
O2
SvO2

Effect of Oxygen Consumption (VO2) on SvO2
0.850.79
0.74
0.68
0.57
0.46
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0 100 200 300 400 500 600
Oxygen Consumption (VO2)
Sv
O2
SvO2

REFERENCES
• Current Opinion Critical Care 2001; 7: 204-211• NEJM 2001; 345: 1368-1377• Critical Care Medicine 2002; 30: 1686-1692• Circulation 1969; 40: 165• Thorax 2002; 57: 170-177• Academic Emer Med 1999; 6: 421