Embed Size (px)
Citation preview

April 12, 2023 1
Cretinism & Hypothyroidism
in ChildrenDr.K.V.Giridhar
Associate Prof. of Pediatrics
GMC. Ananthapuramu, A.P.,India.

• cretinism: ’congenital disease’ due to absence or deficiency of normal thyroid secretion, characterized by physicaldeformity, dwarfism, and mental retardation, and often by goiter.
• Hypothyroidism: ‘acquired disease’ due to primary and other various causes of Thyraoid and hypothalamo, pitutory,thyraoid axis abnormaloties.

Etioliogy of CretinismCONGENITAL
Hypoplasia & mal-descent of thyraoid
Familial enzyme defectsIodine deficiency in pregnacy (endemic cretinism)
Intake of ‘goitrogens’ during pregnancy
Pituitary defectsIdiopathic

Etiology of Hypothyroidism
ACQUIREDIodine deficiencyAuto-immune thyroiditisThyroidectomy or RAI therapyTSH or TRH deficiencyMedications (iodide & Cobalt)Idiopathic

GOITROGENS
• DRUGSAnti-thyroidCough medicinesSulfonamidesLithiumPhenylbutazonePASOral hypoglycemic agents

GOITROGENS
FOODSoybeansMilletsCassavaCabbage

THYROID HORMONESIodine & tyrosine, together
form both, T3 & T4 under TSH stimulation, in thyroid gland.
When released into circulation T4 binds to:Globulin(TBG)-75%Prealbumin(TBPA)-20%Albumin(TBA)- 5%

THYROID HORMONES (c’d)Less than 1% of T4 & T3 is free in
plasma.T4 is deiodinated in the tissues to
either T3 (active)At birth T4 level approximates
maternal level, but increases rapidly during the first week of life.
High TSH in the first 5 days of life can give false positive neonatal screening for ‘hypothyroidism’.

Thyroid stimulating Hormone (TSH)
Is a Glyco-protein. Secreted by the anterior
pituitary under influence of TRH(TSRH)
It has trophic effect on thyroid gland
It also stimulates, iodine trapping, oxidation, organification, coupling and proteolysis of T4 & T3.

TSH (c’d) T4 & T3 are feed-back regulators
of TSH TSH is stimulated by a-adrenergic
agonists TSH secretion is inhibited by:
DopamineBromocreptineSomatostatinCorticosteroids

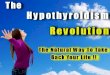
Hypothalamo, pituitary, thyraoid Axis
Pituitary gland
Thyroid gland
Hypothalamus
T3
T4
TRH
TSH

THYROID HORMONES (c’d)
Acute & chronic illnessesb-adrenergic receptor blockersStarvation & severe PEMCorticosteroidsPropylthiouracilHigh iodine intake (Wolff-Chaikoff
effect)
Conversion of T4 to T3 is decreased by:

THYROXINE (c’d)
Premature infantsHypo pituitarismNephrotic syndromeLiver cirrhosisPEMProtein losing enteropathy
Total T4 level is decreased in:

THYROXINE (c’d)
SteroidsPhenytoinSalicylatesSulfonamidesTestosteroneMaternal TBIgs.
Drugs, which decrease Total T4:

THYROXINE (c’d)
Acute thyroiditisAcute hepatitisEstrogen therapyClofibrateiodidesPregnancyMaternal TSH
Total T4 is increased with:

FUNCTIONS OF THYROXINE Thyroid hormones are essential for:
Linear growth & pubertal development
Normal brain development & function
Energy productionCalcium mobilization from boneIncreasing sensitivity of b-adrenergic receptors to catecholeamines

CLINICAL FEATURES
Birth weight > 4 kgOpen posterior fontanelNasal stuffiness & dischargeMacroglossiaConstipation & abdominal
distensionFeeding problems & vomiting

CLINICAL FEATURES (c’d)Non pitting edema of limbs Coarse featuresUmbilical herniaHoarseness of voiceAnemiaDecreased physical activityProlonged (>3 weeks)
neonatal jaundice

CLINICAL FEATURES (c’d)
Dry, pale & mottled skinLow hair line & dry, scanty
hairHypothermia & peripheral
cyanosisHypercarotenemiaGrowth failureRetarded bone ageStumpy fingers & broad hands

CLINICAL FEATURES (c’d)Skeletal abnormalities:
Infantile proportionsHip & knee flexionExaggerated lumbar lordosis
Delayed teeth eruptionUnder developed mandibleDelayed closure of anterior fontanel

OCCASIONAL FEATURESOvert obesityMyopathy & rheumatic painsSpeech disorderImpaired night visionSleep apnea (central &
obstructive)AnasarcaAchlorhydria & low intrinsic
factor


OCCASIONAL FEATURES (c’d)Decreased bone turnoverDecreased VIII, IX & platelets
adhesionDecreased GFR &
hyponatremiaHypertensionIncreased levels of CK,LDH &
AST Abnormal EEG & high CSF
proteinPsychiatric manifestations

CLINICAL FEATURES (c’d)
Neurological manifestationsHypotonia & later spasticityLethargyAtaxiaDeafness + MutismMental retardationSlow relaxation of deep tendon jerks

ASSOCIATIONS
Autoimmune diseases Diabetes MellitusCardiomyopathy & CHDGalactorrhoeaMuscular dystrophy + pseudo hypertrophy (Kocher-Debre-Semelaigne Syndrome)

DIAGNOSIS
Early detection by neonatal screening
High index of suspicion in all infants with increased risk
Overt clinical presentation
Confirm diagnosis by appropriate lab and radiological tests

LABROTARY TESTS
Low (T4& T3)High TSHHigh serum cholesterol & carotene
levelsAnaemia (normo, micro or macrocytic)High urinary
creatinine/hydroxyproline ratioCXR: cardiomegalyECG: low voltage & bradycardia

IMAGING TESTS X-ray films can show:
Delayed bone age or epiphyseal dysgenesis
Anterior beaking of vertebraeCoxavara & coxa plana
Thyroid radio-isotope scan Thyroid ultrasound CT or MRI


THYROID FUNCTION TESTS(c’d)
Specific Tests:Thyroglobulin levelThyroid Stimulating
ImmunoglobulinThyroid antibodiesThyroid radio-isotope scanThyroid ultrasoundCT & MRIThyroid biopsy

TREATMENT L-Thyroxin is the drug of
choice. Start with small dose.Dose is 10 mg/kg/day in infancy. In older children start with 25
mg/day and increase by 25 mg every 2
weeks till required dose.Monitor clinical progress &
hormones level

TREATMENT(c’d) Life-long replacement therapy 5 types of preparations are
available:L-thyroxin (T4)Triiodothyronine (T3)Synthetic mixture T4/T3 in 4:1 ratioDesiccated thyroid (38mg T4 & 9mg
T3/grain)Thyroglobulin (36mg T4 & 12mg
T3/grain)

PROGNOSIS
Depends on:Early diagnosis
Proper counselling
Strict diet control
Careful monitoring
Compliance

PROGNOSIS Is good for linear growth & physical
features even if treatment is delayed, but for mental and intellectual development early treatment is crucial.
Sometimes early treatment may also fail, to prevent mental sub normality due to severe intra-uterine deficiency of thyroid hormones

April 12, 2023 35
THANKYOU