Embed Size (px)
Citation preview
Coronary Artery Coronary Artery DiseaseDisease
Sanjay Kumar KulchaniaSanjay Kumar Kulchania (LECTURER)(LECTURER)
GURU NANAK COLLEGE OF GURU NANAK COLLEGE OF NURSING, DHAHAN KALERANNURSING, DHAHAN KALERAN
ArteriosclerosisArteriosclerosis
• Arteriosclerosis - “hardening of the arteries”.• Atherosclerosis – build up of plaque (atheroma)
on the lining of arteries.• End results for both are the same
– Stenosis of the lumen of artery– Ulceration of plaque– Rupture of plaque with thrombus formation– Obstruction of blood flow– Ischemia of tissue distal to thrombus
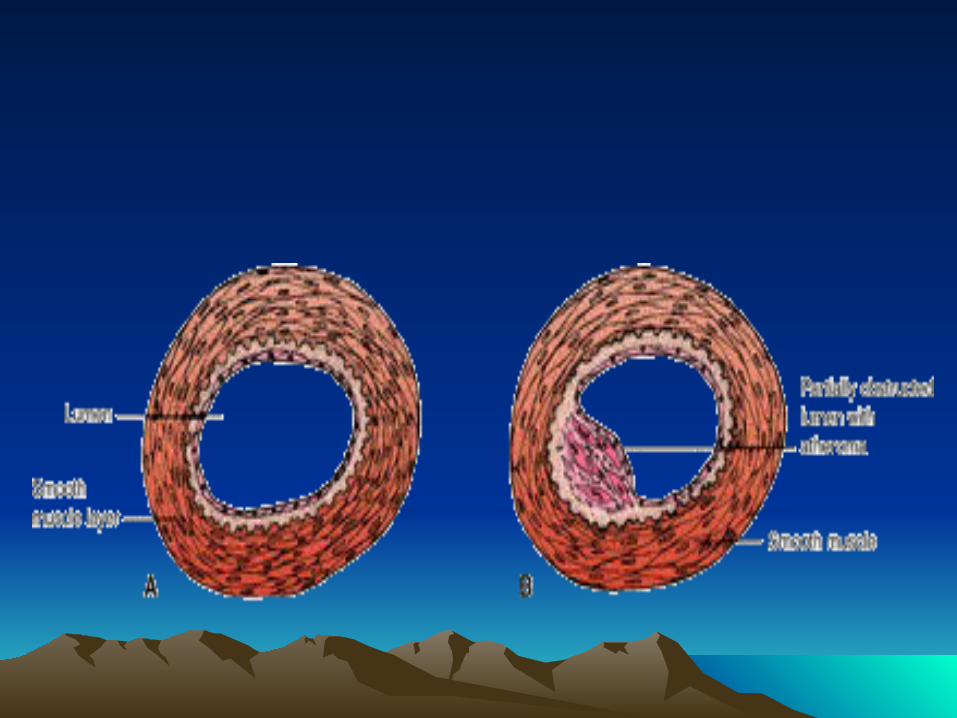
• Inflammatory response secondary to injury is mostly widely accepted theory for development of atherosclerosis.– Endothelial injury from shearing stresses,
radiation, chemicals, hyperlipidemia– Inflammatory response– Beginning of atheroma
Causes of Coronary Artery Causes of Coronary Artery DiseaseDisease
• Atherosclerosis
• Vasospasm
• Thrombus or embolus
Non-modifiable Risk Factors Non-modifiable Risk Factors Contributing To CADContributing To CAD
• Heredity
• Increasing age
• Gender
Modifiable Risk Factors Modifiable Risk Factors Contributing To CADContributing To CAD
• Hypercholesterolemia - dyslipidemia– Measures to reduce cholesterol
• Diet – Therapeutic Lifestyle Changes Diet - total fat < 35%, 50-60% CHO, 15% protein, cholesterol < 200 mg, 20-30 gms fiber
• Exercise• Smoking cessation• Plant stanols• Red yeast rice• Omega 3 fatty acids
• Medications
– HMG-CoA Reductase Inhibitors (statins)
• Most commonly used to decrease LDL and triglycerides, and increase HDL
• Side effects – myopathy (weakness), rhabdomyolysis, hepatotoxicity
• Precautions – avoid grapefruit. Also, may interact with erythromycin, Ca channel blockers and ketoconazole
• Drugs – pravastatin (Pravachol), simvastatin (Zocor), atorvastatin (Lipitor), rosuvastatin (Crestor)
–Nicotinic acid (Vit B3)
• Most effective in increasing HDL and decreasing triglycerides
• Side effects – flushing, hyperglycemia, upper GI distress, hepatotoxicity, hyperuricemia
• Precautions – take with food, take at bedtime, or take ASA 325 mg 30 min before med
• Drugs – Niaspan, Niacin
–Fibric acid
• Used to decrease triglycerides and increase HDL
• Side effects – GI distress, rash, myopathy, increased risk of cholilithiasis, renal failure
• Precautions – can potentiate action of Coumadin
• Drugs – Tricor (fenofibrate), (Lopid) gemfibrozil
–Cholesterol Absorption Inhibitor
• Inhibits absorption of cholesterol in intestines
• Decreases LDL & triglycerides, increases HDL
• Precautions – liver disease
• Side effects – abdominal pain, arthralgia, diarrhea, HA
• Drugs - Zetia (ezetimibe), Vytorin (Zetia & Zocor)
–Bile acid sequestrants (resins)
• Decrease absorption of bile acids in intestines
• Effective in decreasing LDL and slightly increasing HDL
• Side effects – constipation, decreased absorption of other meds, increased flatulence
• Drugs - -cholestyramine (Questran), colesevelam (Welchol)
–Hypertension
• Smoking
–Carbon monoxide displaces oxygen on Hgb
–Nicotinic acid triggers release of catecholamines
–Nicotine increases platelet aggregation
• Diabetes• Physical inactivity - beneficial effects of
exercise– Increases HDL– Decreases LDL, triglycerides, glucose– Increases insulin sensitivity– Decreases BP and body mass
• Obesity
• Metabolic syndrome
• Stress
• Elevated homocysteine levels
• Elevated C-reactive protein (CRP)
• Elevated Lp – PLA2
Angina PectorisAngina Pectoris
• From Latin word meaning “to choke”
• Clinical syndrome characterized by episodes of discomfort or pressure in the upper chest
• Result of ischemia
• Atherosclerosis is most common cause
Factors Known To Precipitate Factors Known To Precipitate Typical AnginaTypical Angina
• Physical exertion
• Exposure to cold
• Eating a heavy meal
• Stress or emotional situation
Various Classifications of Various Classifications of AnginaAngina
• Stable angina – classic angina
• Unstable angina – pre-infarction angina
• Variant angina – Prinzmetal’s angina
Clinical Manifestations of Clinical Manifestations of Typical AnginaTypical Angina
• Heaviness, squeezing, pressure, tightness in upper chest
• Choking or smothering sensation
• Indigestion or gas
• Radiation to neck, jaw, shoulders and arms
• Feeling of weakness or numbness in arms, wrists or hands
• Associated symptoms– Dyspnea– Diaphoresis– Dizziness– N/V– Anxiety
Diagnostic Findings With Diagnostic Findings With AnginaAngina
• Diagnosis often made by evaluating clinical manifestations and history
• 12 lead ECG
• Stress test with or without nuclear scan or ECHO
• Cardiac catheterization
• EBCT
Objectives of Medical Objectives of Medical Management of AnginaManagement of Angina
• Decrease oxygen demands of myocardium or myocardial oxygen consumption
• Increase oxygen supply
Treatment of AnginaTreatment of Angina
• Pharmacologic therapy
• Control risk factors
• Revascularization– Invasive interventional procedures– Coronary artery bypass grafting (CABG)
Pharmacologic Therapies For Pharmacologic Therapies For AnginaAngina
• Nitrates – mainstay of treatment– Dilate veins – decreases preload– Dilate arteries – decreases afterload as well as
dilates coronary arteries– Administer- spray, sublingually, PO, IV, topically– Side effects – hypotension, HA, flushing,
tachycardia– Ex: Nitrostat SL or Tridil (nitroglycerin), Imdur
(isosorbide mononitrate)– Need a nitrate free interval– DO NOT administer with Viagra
• Client teaching related to sublingual (SL) nitroglycerine (NTG)– Carry NTG on person at all times– Heat, light, and moisture cause NTG to
lose its potency. Store in original container.
– Renew every 6 months– Sit or lie down when taking– Take one tablet under tongue every 5 min
until angina relieved. If no relief after 3 tabs, call 911!!
– May take immediately before activity causing angina
• Beta blockers
– Reduce myocardial oxygen consumption by decreasing heart rate, contractility and blood pressure
– Caution client not to stop med abruptly; may cause rebound angina
– Monitor heart failure clients for worsening failure– Side effects – hypotension, bradycardia,
bronchial spasm, masks hypoglycemia– Ex: Lopressor or Toprol (metoprolol), Inderal
(propranolol), Tenormin (Atenolol)
• Calcium channel blockers– Dilate arteries – decreases SVR which
decreases workload and O2 consumption– Decrease heart rate and myocardial
contractility – decreases O2 consumption– Avoid in clients with severe heart failure– Side effects - hypotension, bradycardia,
constipation, edema, AV blocks– Ex: Adalat or Procardia (nifedipine),
Cardene (nicardipine), Cardizem (diltiazem)
• Antiplatelet medications– Prevent platelet aggregation on atheroma or
thrombus • ASA – side effects: GI irritation, bleeding,
increased bruising• Ticlid (ticlopidine) – side effects: neutropenia,
GI upset, N/V/D, rash. Must monitor CBC• Plavix (clopidogrel) – side effects: increased
bleeding tendencies, N/V/D, rash
• Anticoagulants– Heparin
• Given IV in acute situations or subcutaneous in non-acute situations
• Monitor partial thromboplastin time (PTT) or anti-Xa level (measure of Factor Xa in coag cascade)
• Antidote – Protamine Sulfate• Observe bleeding precautions• Monitor for signs and symptoms of bleeding• Half-life of 1-2 hrs• Monitor for Heparin induced thrombocytopenia
(HIT)

– Coumadin (warfarin)• Used long term; given PO• Effects do not occur for 3-5 days• Monitor Prothrombin time (PT) or International
Normalized Ratio (INR)• Antidote – Vitamin K (AquaMEPHYTON)• Affected by certain foods• Contraindicated in pregnancy, clients with liver
dysfunction or those at risk for bleeding
• Oxygen therapy– Administered usually at 2 L/min per nasal
cannula– Increases amount of O2 delivered to
myocardium
Nursing Interventions For Client Nursing Interventions For Client With AnginaWith Angina
• Treat pain – indicates ischemia– Instruct client to stop activities and sit or lie in semi-
Fowler’s position– Assess pain, monitor VS, observe for dyspnea– Administer O2 at 2L per NC if hospitalized– Obtain 12 lead ECG– Administer NTG - reassess client and vital signs every
5 min.– Inform physician if pain severe or unrelieved
• Reduce anxiety
• Teach self care– Risk factor modification– Medications– When to call physician– When to call 911
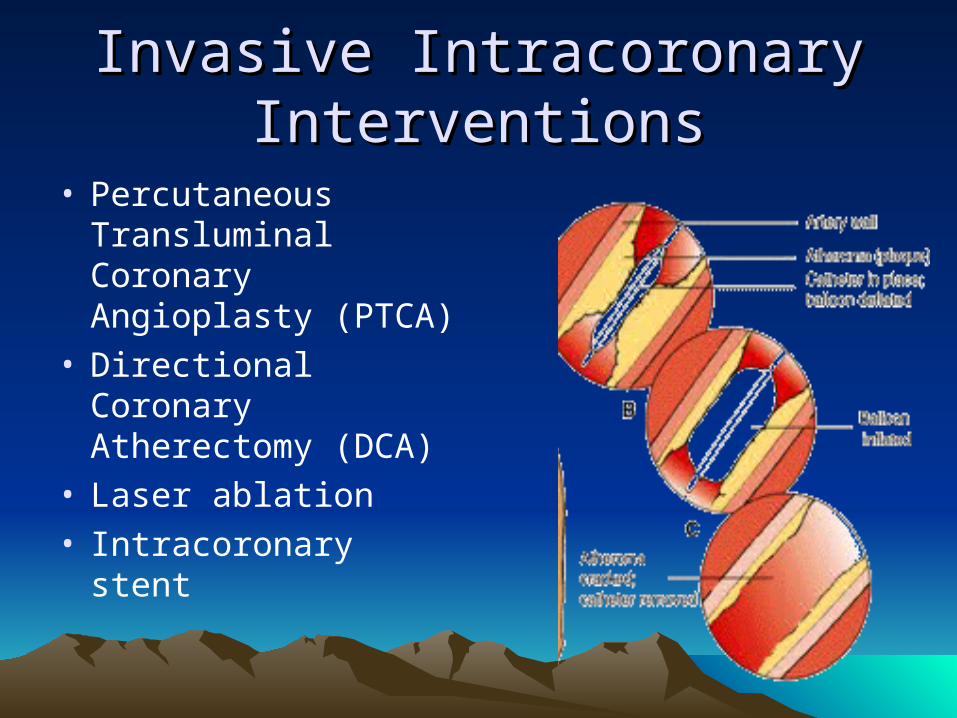
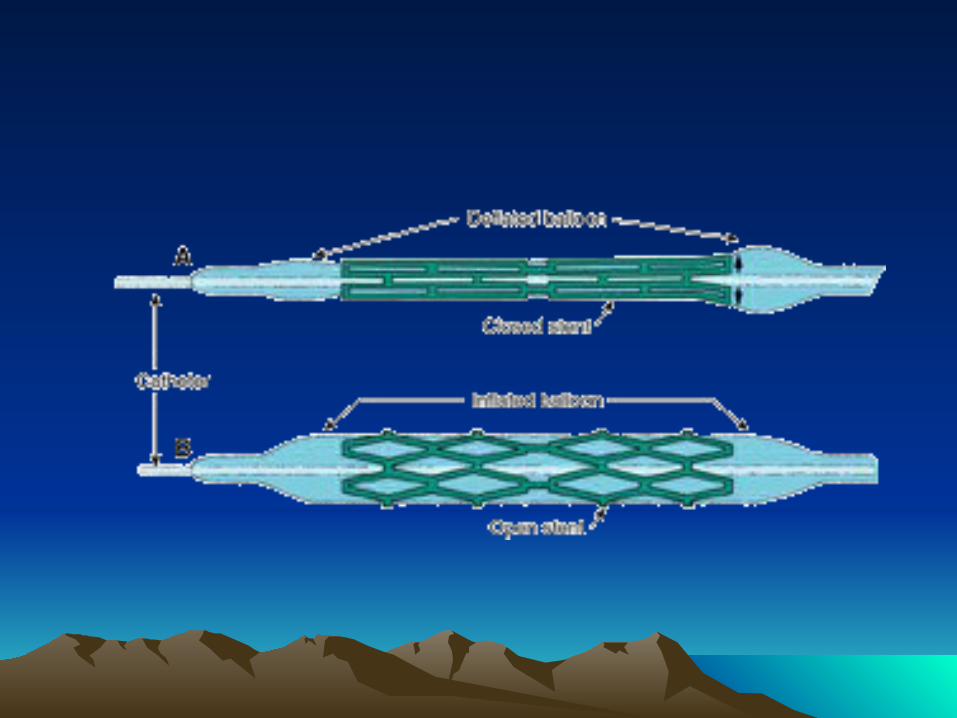
Invasive Intracoronary Invasive Intracoronary InterventionsInterventions
• Percutaneous Transluminal Coronary Angioplasty (PTCA)
• Directional Coronary Atherectomy (DCA)
• Laser ablation• Intracoronary stent
Complications Related To Invasive Complications Related To Invasive Intracoronary InterventionsIntracoronary Interventions
• Dissection, perforation, abrupt closure, vasospasm
• Acute MI
• Dysrhythmias
• Cardiac arrest
• Restenosis of coronary artery
• Bleeding or hematoma formation
• Retroperitoneal bleeding
• Pseudoaneurysm
• Arteriovenous fistula
• Arterial thrombosis
Post Procedure Nursing CarePost Procedure Nursing Care
• Achieve homeostasis after sheath removed• Frequent monitoring of VS and cath site for
bleeding• Frequent monitoring of access limb for
vascular problems• Administration of Heparin or platelet inhibitor
(Integrelin, Aggrastat) as ordered
• Administration of IV NTG as ordered
• Bed rest with HOB elevated 30 degrees
• Keep access extremity straight
• Monitor for complications
• Force fluids
Coronary Artery Coronary Artery RevascularizationRevascularization
• Classic coronary artery bypass grafting (CABG)
• Minimally invasive direct CABG – MIDCABG
• Port access coronary artery bypass grafting
• Transmyocardial laser revascularization
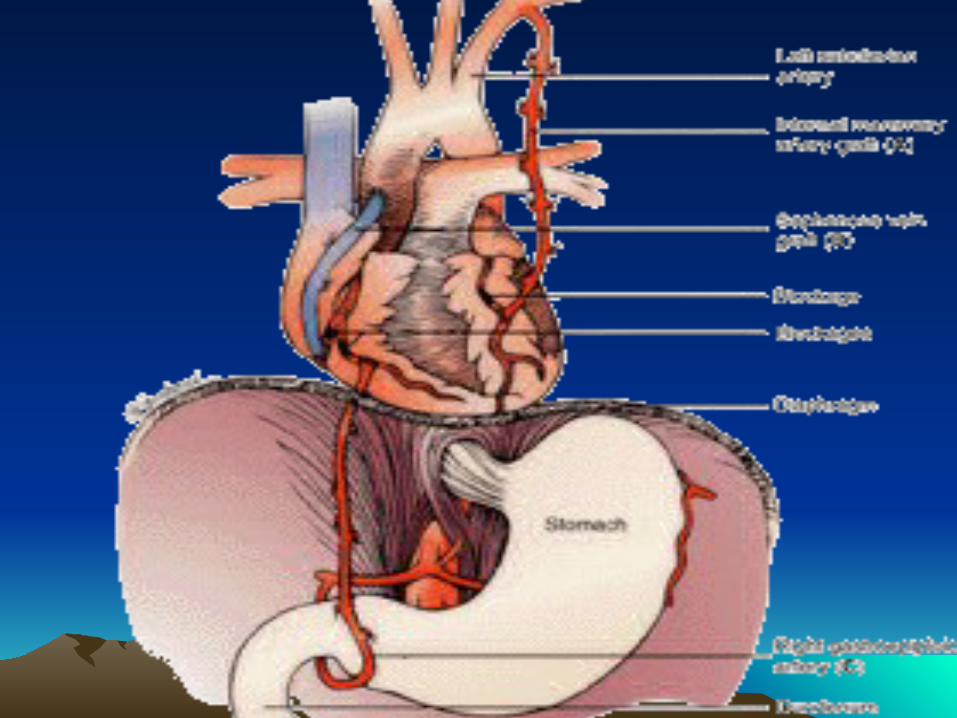
Graft Selection For CABGGraft Selection For CABG
• Greater saphenous vein
• Lesser saphenous vein
• Cephalic and basilic vein
• Internal mammary arteries
• Radial artery
Complications After CABGComplications After CABG
• Dysrhythmias
• Hemorrhage
• Fluid and electrolyte imbalances
• Respiratory dysfunction
• Wound infection and dehiscence
• Thrombus and embolus
• Intra-operative stroke or MI
• Renal failure
• Multiple organ failure
• Death

Nursing Interventions Post CABGNursing Interventions Post CABG
• Maintain patent airway
• Promote lung re-expansion
• Monitor cardiac status
• Monitor and maintain fluid and electrolyte balance
• Monitor cerebral circulation

• Provide pain relief
• Monitor GI function
• Monitor and prevent thrombophlebitis
• Monitor for dysrhythmias
• Post operative education– Walking– Activity restrictions– Resumption of sexual activity– Wound cleaning– Symptoms to report to MD
Expected OutcomesExpected Outcomes
• Relief of angina
• Decreased anxiety
• Absence of complications
• Verbalizes understanding of treatment regimen
• Adheres to self-care program
Pathophysiology of Pathophysiology of Myocardial Infarction Myocardial Infarction
• Interruption of blood flow
• Ischemia develops
• Ischemia lasting greater than 20 min results in infarction
• Acidosis in myocardial cells leads to conduction disorders
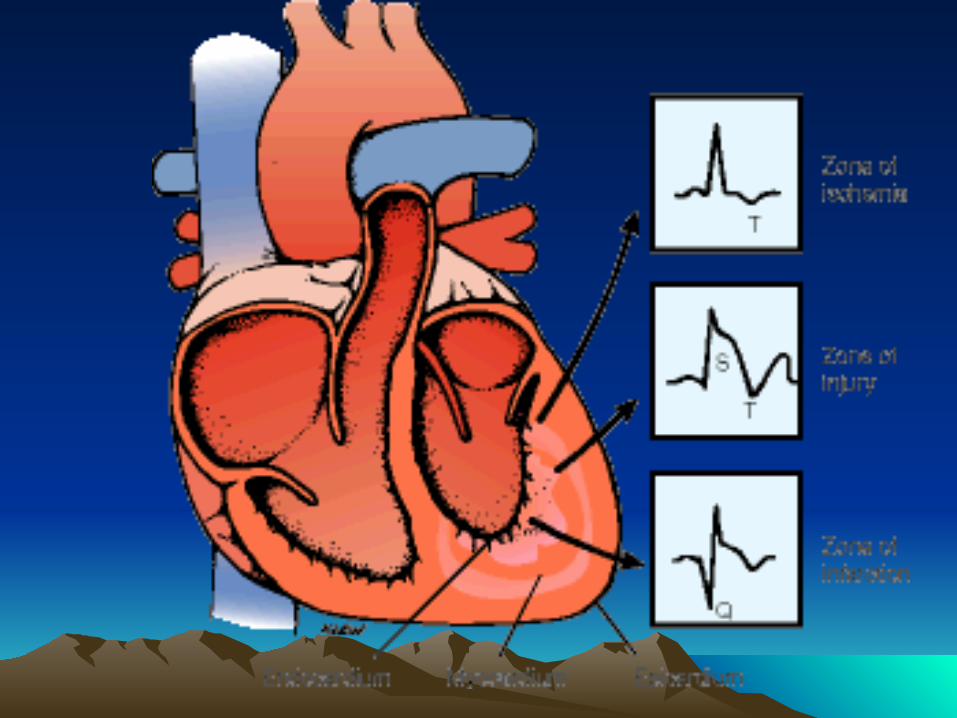
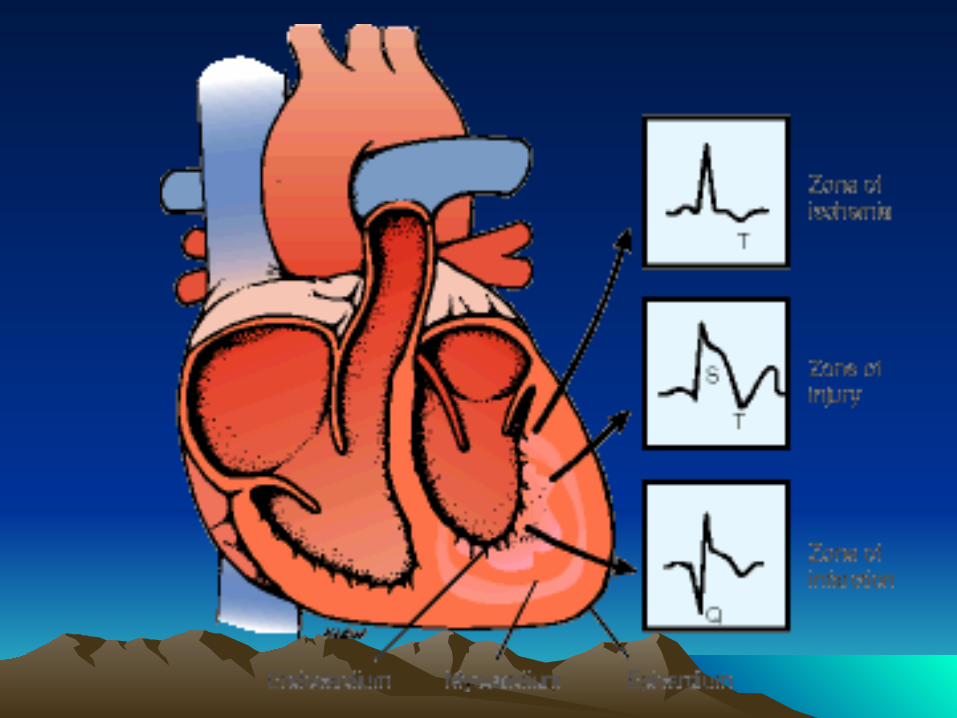
• Zones of damage– Zone of infarction– Zone of hypoxic injury– Zone of ischemia
• Remodeling occurs
Depth Of Myocardial InfarctionDepth Of Myocardial Infarction
• Transmural infarction – Q wave MI or ST segment elevation MI (STEMI)
• Subendocardial infarction – Non Q-wave MI or non-ST segment elevation MI (Non-STEMI)
Locations Of Myocardial Locations Of Myocardial InfarctionInfarction
• Anterior myocardial infarction (AMI)– From occlusion of LAD– Risk for failure, shock, conduction problems
• Inferior myocardial infarction (IMI)– From occlusion of RCA– Risk for dysrhythmias due to effect on SA & AV
node• Lateral infarction (LMI)
– From occlusion of LCX • Posterior infarction (PMI)
– From occlusion of LCX or PDA
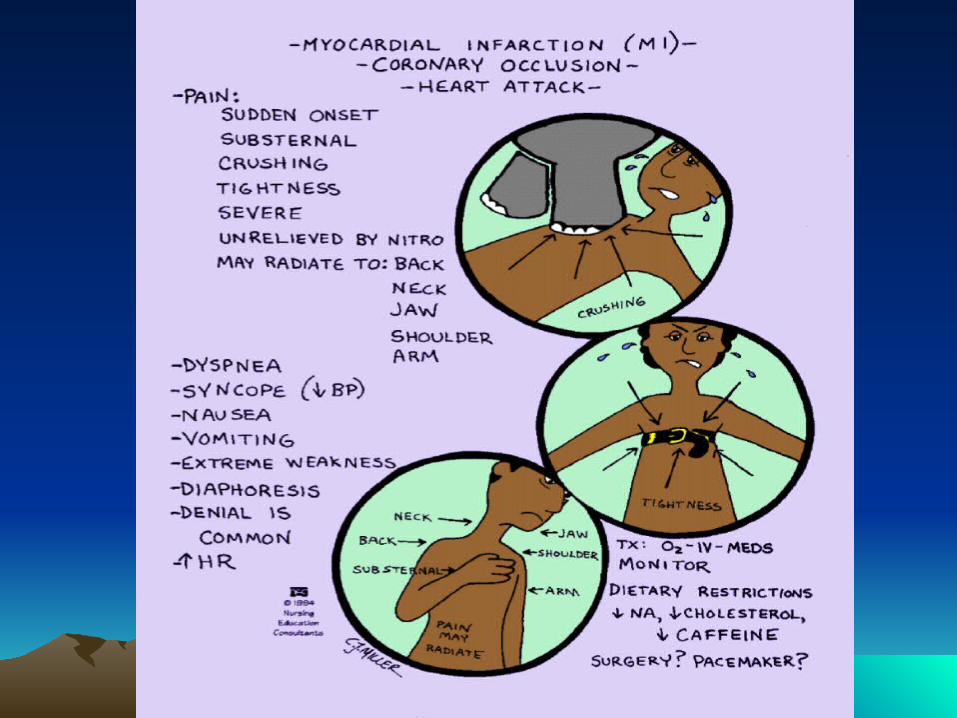
Clinical Manifestations Of An MIClinical Manifestations Of An MI
• Similar to unstable angina
• Discomfort not relieved with rest or 3 NTG
• Lasts longer then 20 min
• Sense of impending doom
Diagnostic Tests For MIDiagnostic Tests For MI
• 12 lead ECG
• Cardiac enzymes
• ECHO
• Cardiac catheterization
Major Goals For Care Of Client Major Goals For Care Of Client With MIWith MI
• Initiate prompt care
• Minimize myocardial damage
• Manage complications
• Rehabilitate and educate client and family
Provide Immediate Care To Client Provide Immediate Care To Client With Suspected MIWith Suspected MI
• Keep client calm and quiet
• O2 per NC
• Assess VS
• Connect client to heart monitor
• Perform 12 lead ECG
• Administer NTG
• Start IV lines, draw blood for labs
• Administer ASA
MONA Greets Everyone At The MONA Greets Everyone At The DoorDoor
• M
• O
• N
• A
Minimize Myocardial DamageMinimize Myocardial Damage
• Interventions to reduce pain – indicates ischemia – O2
– Coronary vasodilators– Morphine sulfate– Beta blockers
• Reperfuse coronary artery– Thrombolytics - lyse clots by converting
plasminogen to plasmin• Ex: Streptokinase, Urokinase, recombinant tissue
plasminogen activator (tPA) ie. Activase or Retavase
– Nursing interventions with thrombolytics• Minimize number of skin punctures• Avoid IM injections• Start at least 2 IV lines • Monitor for signs and symptoms of bleeding• Monitor for reperfusion dysrhythmias• Monitor for allergic reactions with Streptokinase• Treat bleeding with direct pressure and notify
physician
– ASA– Heparin– PCI
• Reduce myocardial oxygen consumption or demand– Bed rest– Gradually increase activity. Rest 1hr after
meals. No isometric exercises or straining– ACE inhibitors– Beta blockers
Monitor For And Manage Monitor For And Manage ComplicationsComplications
• Dysrhythmias– Provide continuous cardiac monitoring– Assess client’s tolerance– Inform physician– Administer anti-dysrhythmics as ordered or
per protocol (Lidocaine, Atropine, Adenosine, Verapamil)
– Defibrillation– Temporary pacing
• Cardiogenic shock – occurs due to loss of contractile forces in heart– Monitor for signs of shock– Improve cardiac output – positive inotropic
drugs (Inocor, Dobutamine, Dopamine) or IABP
• Heart failure and pulmonary edema – may occur at onset of MI or later– Monitor for signs and symptoms– Monitor daily weights and I&O– May limit fluid intake 2000cc/24 hrs– Restrict diet to 2gm NA– Meds to tx: Lasix, ACE inhibitors, Lanoxin– For PE: high Fowler’s, O2, MS, Lasix
• Pericarditis – inflamed area of MI rubs against pericardium causing loss of lubricating fluid– Monitor for chest pain that increases with
movement or deep inspiration– Monitor for pericardial friction rub– Administer anti-inflammatory agents –
Indocin (indomethacin), ASA, ibuprofen, steroids
– Administer analgesics
• Dressler’s Syndrome – Form of pericarditis that occurs as late as 6
wks to months after MI– Treatment same as pericarditis
Complications Less Likely To Complications Less Likely To OccurOccur
• Papillary muscle rupture– Monitor for new systolic murmur, heart failure– Emergency valve surgery required
• Ventricular septal rupture– Monitor for new systolic murmur– Emergency surgical correction required
• Cardiac rupture– Monitor for CP, hypotension, elevated JVD,
dyspnea– Death occurs
Educate and Rehabilitate Client Educate and Rehabilitate Client and Familyand Family
• Provide education on– Progressive activity guidelines– Diet– Medications– When to call 911– Symptoms to inform physician of
• Begin Myocardial Infarction Rehabilitation Program (MIRP) – Phase I– Phase II– Phase III– Phase IV
Expected OutcomesExpected Outcomes
• Relief of angina
• No signs of respiratory difficulties
• Adequate tissue perfusion
• Absence of complications
• Decreased anxiety
• Adherence to self-care program
PacemakerPacemaker
• Provides an electrical stimulation to the atria or ventricles, or both, which causes contraction
• Indications– SA node fails to fire or generates impulses too slowly– Conduction system fails to conduct impulses properly– Tachydysrhythmias that are unresponsive to meds
Time Frames For Pacemaker Time Frames For Pacemaker UseUse
• Temporary
• Permanent
Pacemaker DesignPacemaker Design
• Electronic pulse generator– Circuitry that senses
cardiac activity– Battery that generates
impulses
• Lead wire– Flexible conductive
wire with electrode at end
– Relays cardiac info back to generator and delivers impulse to myocardium
Pacing MethodsPacing Methods
• Transcutaneous (External) pacing– Used in emergencies– Large amounts of energy needed to traverse
tissues to heart resulting in burns
• Epicardial (Transthoracic) pacing– Generally used with open heart surgeries– Four electrodes attached to epicardium
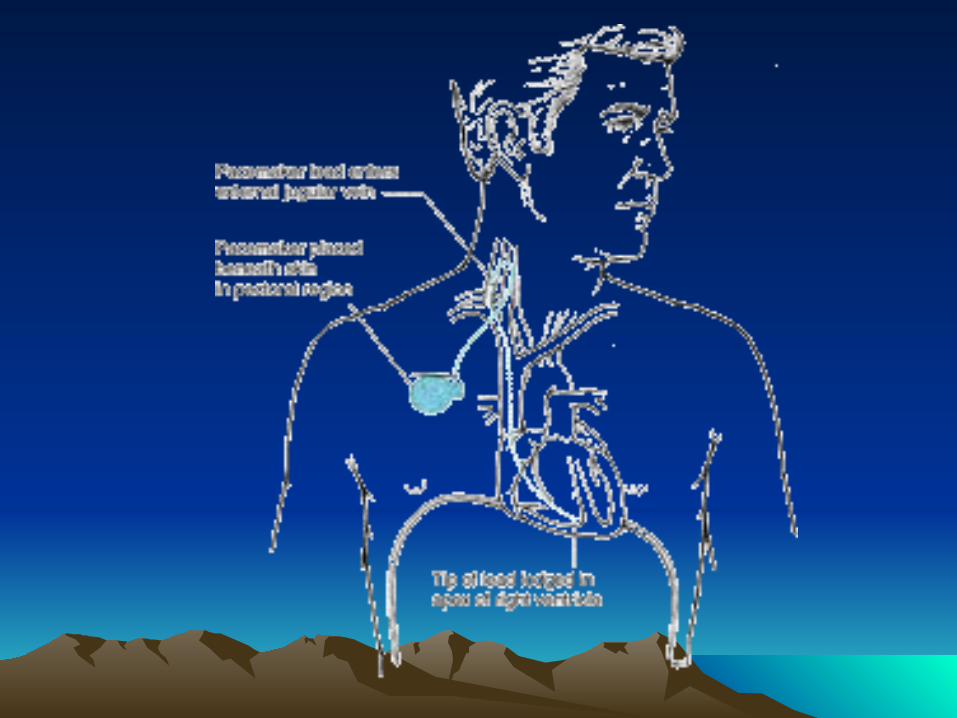
• Transvenous (Endocardial) pacing– Used in temporary and permanent situations– Lead wires inserted into subclavian, brachial,
jugular, femoral vein– Temporary use – external generator– Permanent use – generator implanted under
skin


Pacemaker ModesPacemaker Modes
• Fixed rate mode (asynchronous)– Set to fire continuously at preset rate– If fires during repolarization, can cause VT or
VF
• Demand mode– Senses heart’s intrinsic activity– Fires only when heart rate fall below preset
rate
Complications Associated With Complications Associated With Pacemaker InsertionPacemaker Insertion
• Infection
• Thrombophlebitis
• Bleeding or hematoma
• Ventricular dysrhythmias
• Pneumothorax, hemothorax
• Lead displacement
• Pacemaker malfunction
• Stimulation of phrenic nerve or diaphragm
• Cardiac tamponade
Nursing Care of Client Post Nursing Care of Client Post Pacemaker InsertionPacemaker Insertion
• Monitor VS frequently• Obtain chest x-ray• Continuous ECG monitoring
• Obtain 12 lead ECG with and without magnet if demand pacer
• Monitor for infection at insertion site of pulse generator or leads
• Exposed epicardial wires must be covered with nonconductive material
• Avoid excessive extension or abduction of arm on operative site
• Assess client for anxiety
• Assess and medicate for pain
• Elevate HOB
• Educate client and family on home care
Teaching For Client With Teaching For Client With PacemakerPacemaker
• Assess wound daily and report any swelling, redness, warmth, drainage
• Wear loose fitting clothes over generator• Do not lift more than 5-10 lbs with affected arm
for 6 wks• Do not raise elbow above shoulder or toward
back for 6 wks• Check pulse daily for 1 minute. Report
decreases or increases
• Report sensations of heart “racing’, beating irregularly, dizziness, fainting
• Avoid strong electromagnetic fields
• Can safely use most appliances and tools that are grounded
• Metal detectors may be triggered. Avoid use of hand scanners over generator
• Do not carry cell phone, turned on, directly over generator
• Avoid contact sports • Carry medical ID with pacer and physician
info• Explain importance of pacer follow-up.
Generator will need to be changed out periodically
Implantable Cardiovertor Implantable Cardiovertor Defibrillator (ICD)Defibrillator (ICD)
• Cardioverts/defibrillates lethal dysrhythmias
• Can perform overdrive pacing or demand pacing
• Inserted the same as permanent pacer
• Complications same as permanent pacer