- 1. References Grossmans Textbook of Cardiac Catheterization
Kerns Handbook of Interventional Catheterization Hursts The Heart
13th Edition Braunwalds Heart Disease 9th edition Greys Anatomy
Carlo Di Mario, Nilesh Sutaria. CORONARY ANGIOGRAPHY IN THE
ANGIOPLASTY ERA: PROJECTIONS WITH A MEANING Heart
2005;91:968976
2. Coronary Anatomy Main coronary trunks lie in one of two
orthogonal planes Anterior descending and posterior descending
coronary arteries lie in plane of IVS Right and circumflex coronary
trunks lie in plane of AV valves 60 LAO projection is looking down
plane of IVS, with plane of AV valves seen en face 30RAO
projection, one is looking down plane of AV valves, with plane of
IVS seen en face Major segments and branches: BARI modification of
CASS nomenclature 3. Clinical division of RCA Proximal - Ostium to
1st main RV branch Mid - 1st RV branch to acute marginal branch
Distal - acute margin to crux 4. Clinical division of LAD Proximal
- Ostium to 1st major septal perforator Mid - 1st perforator to D2
(90 degree angle) Distal - D2 to end 5. Clinical division of the
LCX Proximal - Ostium to 1st major obtuse marginal branch Mid - OM1
to OM2 Distal - OM2 to end 6. Normal calibre of major coronaries
LMCA: 4.5 0.5 mm LAD: 3.7 0.4 mm LCX : 3.5 0.5 mm ( 4.2 mm if
dominant) RCA: 3.9 0.6 mm ( 2.8 mm if non-dominant) 7. LCA ostium ~
4mm RCA ostium~ 3.2mm 8. Coronary Anatomy Right-Dominant
Circulation-85% RCA conus branch (supplies RVOT) AM(supply free
wall of RV) AV nodal artery, PDA-PLV (supplies inf part of IVS) 9.
Left-Dominant Circulation- 8%, PD,PLV & AV nodal all supplied
by terminal portion of LCX Balanced-Dominant Circulation- 7% RCA-
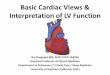
PD LCX- all PLV 10. Coronary Segment Classification 11. Right
coronary 1, prox 2, mid 3, distal 4,PD 5, posteroatrioventricular
6, 1st PL 7, 2nd PL 8, 3rd PL 9, inferior septals; 10, AM Left
coronary 11, LM 12, prox LAD 13, mid LAD 14, distal LAD 15, 1st
diag (a, br of 1st diag) 16, 2nd diagonal,;17, septals (anterior
septals); 18, prox LCX 19, mid LCX 19a, distal LCX 20, 21, and 22,
1st, 2nd, 3rd OM 23, left atrioventricular; 24, 25, and 26, 1st,
2nd, 3rd, PL (in left- or balanced-dominant system); 27, left PD
(in left- dominant system); 28, ramus (ramus intermedius); 29, 3rd
Diag 12. Angiographic Views-Nomenclature AP position Image
intensifier is directly over patient with beam traveling
perpendicularly back to front (i.e., from posterior to anterior) to
patient lying flat on x-ray table RAO position Image intensifier is
on right side of patient. A, anterior; O, oblique LAO position
Image intensifier is on left side of patient Lt Lateral position
Image intensifier rotated 90 deg parallel to floor Cranial Image
intensifier is tilted toward head of patient Caudal Image
intensifier is tilted toward feet of patient 13. AP caudal or
shallow RAO LMCA -entire length Prox LAD & LCX (branches
overlapped) After LM segment, slight RAO or LAO angulation may be
necessary to clear density of vertebrae /catheter shaft 14.
LAO-cranial view LMCA (slightly foreshortened) LAD-Septal &
diagonal are separated clearly LCX/OM: foreshortened/ overlapped
PD/PL of left-dominant circulation are displayed clearly Deep
inspiration helpful Cranial angulation permits view of LAD/LCX
bifurcation LAO-cranial angulation that is too steep or inspiration
that is too shallow produces considerable overlapping with
diaphragm and liver, degrading the image 15. RAO-caudal LMCA
bifurcation Origin & course of LCX/OM, RI & prox LAD seen
clearly One of the best for visualization of LCX LAD beyond
proximal segment obscured Apical LAD displayed clearly 16.
RAO-cranial Used for origins of diagonals along mid /distal LAD
Diagonals bifurcations well visualized Diagonals projected upward
Prox LAD/LCX usually overlapped 17. LAO-caudal (spider view) LMCA
(foreshortened) & LMCA bifurcation Prox & mid LCX with
origins of OM 18. Lateral view Best view to show mid & distal
LAD LAD/LCX well separated Diagonals usually overlapped RI course
well visualized It best shows insertions of bypass grafts into mid
LAD 19. LAO-cranial Origin of RCA Entire length of mid RCA PDA
bifurcation (crux) Cranial angulation tilts PDA down to see vessel
contour / reduce foreshortening Deep inspiration is necessary to
clear diaphragm 20. RAO view Shows mid RCA & length of PDA / PL
Septals coursing upward from PDA, supplying occluded LAD artery via
collaterals, may be clearly identified PL are overlapped, may need
addition of cranial view 21. AP cranial Shows origin of RCA Mid
segment foreshortened Best view for PD/PL of dominant RCA system
and size of collateralized LAD 22. Lateral view Shows RCA origin
(especially in pt with more anteriorly oriented orifices) and mid
RCA PDA and PL are foreshortened 23. Saphenous vein graft views 1.
RCA graftLAO cranial, RAO, and AP cranial 2. LAD graft (or internal
mammary artery)lateral, RAO cranial, LAO cranial, and AP (lateral
view is especially useful to visualize anastomosis to LAD) 3. CFX
(and obtuse marginal branches) graftsLAO caudal and RAO caudal 4.
Diagonal graftLAO cranial and RAO cranial 24. Routine Angio views
Left Coronary Artery For Concentration on Vessel Segment Straight
AP or 5 -10 deg RAO with caudal Left main 30- 45 deg LAO & 20
-30 deg cranial LAD-circumflex bifurcation 30- 40 deg RAO & 20
- 30 deg caudal Circumflex + marginal branches 5 - 30 deg RAO &
20 - 45 deg cranial LAD + diagonals 50 - 60 deg LAO & 10 - 20
deg caudal (spider view) LAD-circumflex bifurcation, circumflex,
marginals Lateral (optional) Bypass conduits to LAD Right Coronary
Artery For Concentration on Vessel Segment 30 - 45 deg LAO & 15
- 20 deg cranial Proximal, mid, PDA 30 - 45 deg RAO Proximal, mid,
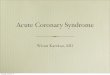
PDA Lateral (optional) 25. Optimal angiographic views for coronary
segments Carlo Di Mario, Nilesh Sutaria. CORONARY ANGIOGRAPHY IN
THE ANGIOPLASTY ERA: PROJECTIONS WITH A MEANING Heart
2005;91:968976. 26. Optimal angiographic views for coronary
segments Carlo Di Mario, Nilesh Sutaria. CORONARY ANGIOGRAPHY IN
THE ANGIOPLASTY ERA: PROJECTIONS WITH A MEANING Heart
2005;91:968976. 27. Optimal angiographic views for coronary
segments Carlo Di Mario, Nilesh Sutaria.CORONARY ANGIOGRAPHY IN THE
ANGIOPLASTY ERA: PROJECTIONS WITH A MEANING Heart 2005;91:968976.
28. Optimal angiographic views for coronary segments Carlo Di
Mario, Nilesh Sutaria.CORONARY ANGIOGRAPHY IN THE ANGIOPLASTY ERA:
PROJECTIONS WITH A MEANING Heart 2005;91:968976. 29. Optimal
angiographic views for coronary segments Carlo Di Mario, Nilesh
Sutaria.CORONARY ANGIOGRAPHY IN THE ANGIOPLASTY ERA: PROJECTIONS
WITH A MEANING Heart 2005;91:968976. 30. Optimal angiographic views
for coronary segments Carlo Di Mario, Nilesh Sutaria. CORONARY
ANGIOGRAPHY IN THE ANGIOPLASTY ERA: PROJECTIONS WITH A MEANING
Heart 2005;91:968976. 31. Optimal angiographic views for coronary
segments Carlo Di Mario, Nilesh Sutaria.CORONARY ANGIOGRAPHY IN THE
ANGIOPLASTY ERA: PROJECTIONS WITH A MEANING Heart 2005;91:968976.
32. Optimal angiographic views for coronary segments Carlo Di
Mario, Nilesh Sutaria.CORONARY ANGIOGRAPHY IN THE ANGIOPLASTY ERA:
PROJECTIONS WITH A MEANING Heart 2005;91:968976. 33. Thank you