Embed Size (px)
Citation preview

Congenital Heart Disease
MD.Kiyumars Karimi
Congenital aortic stenosis
• Congenital valvular stenosis
• Subaortic stenosis
• supravalvular aortic stenosis
• hypertrophic obstructive cardiomyopathy
LV outflow obstruction
causes
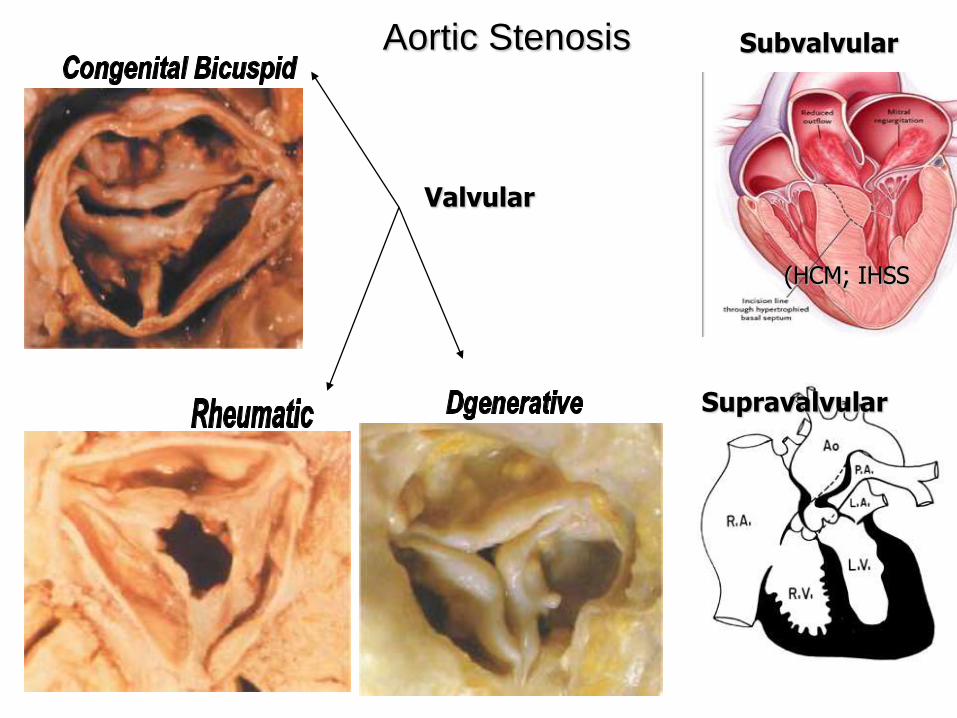
Aortic Stenosis Subvalvular
Supravalvular
Valvular
(HCM; IHSS
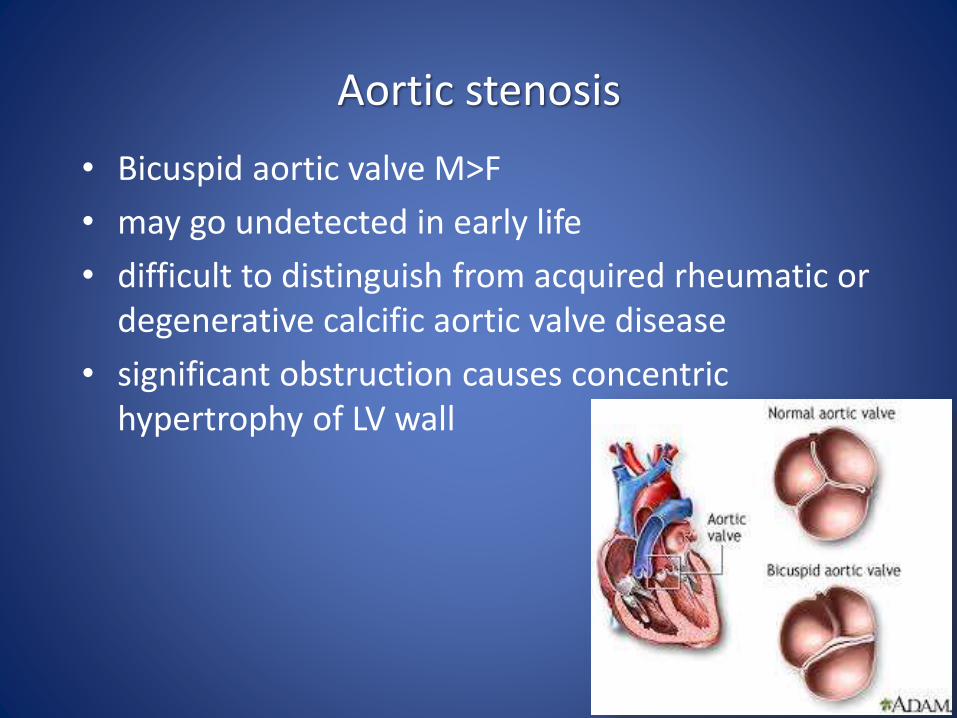
Aortic stenosis
• Bicuspid aortic valve M>F
• may go undetected in early life
• difficult to distinguish from acquired rheumatic or degenerative calcific aortic valve disease
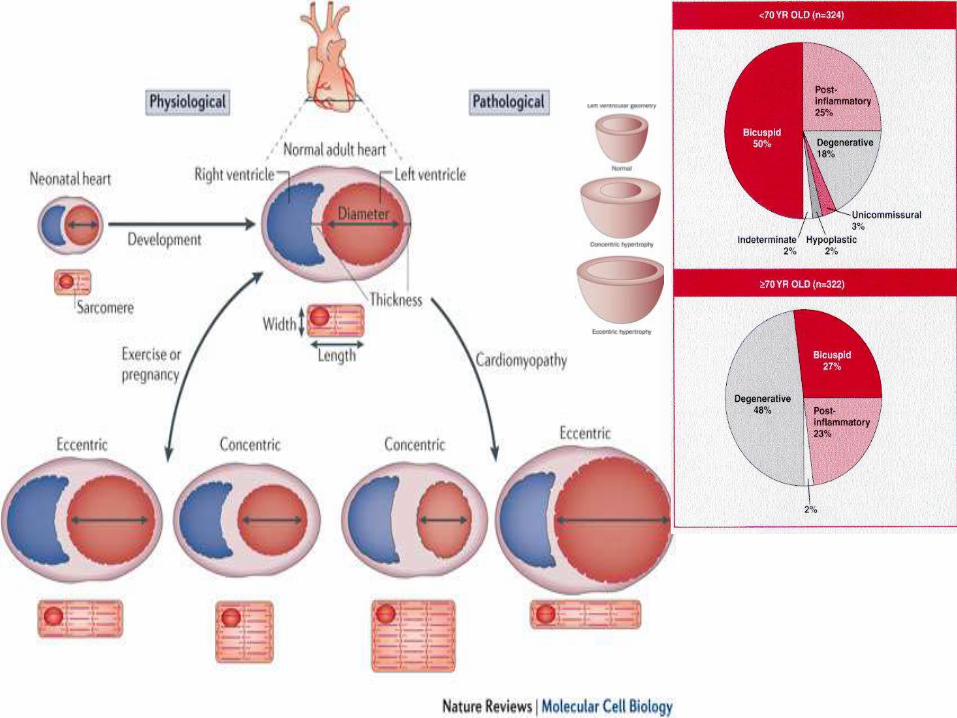
• significant obstruction causes concentrichypertrophy of LV wall
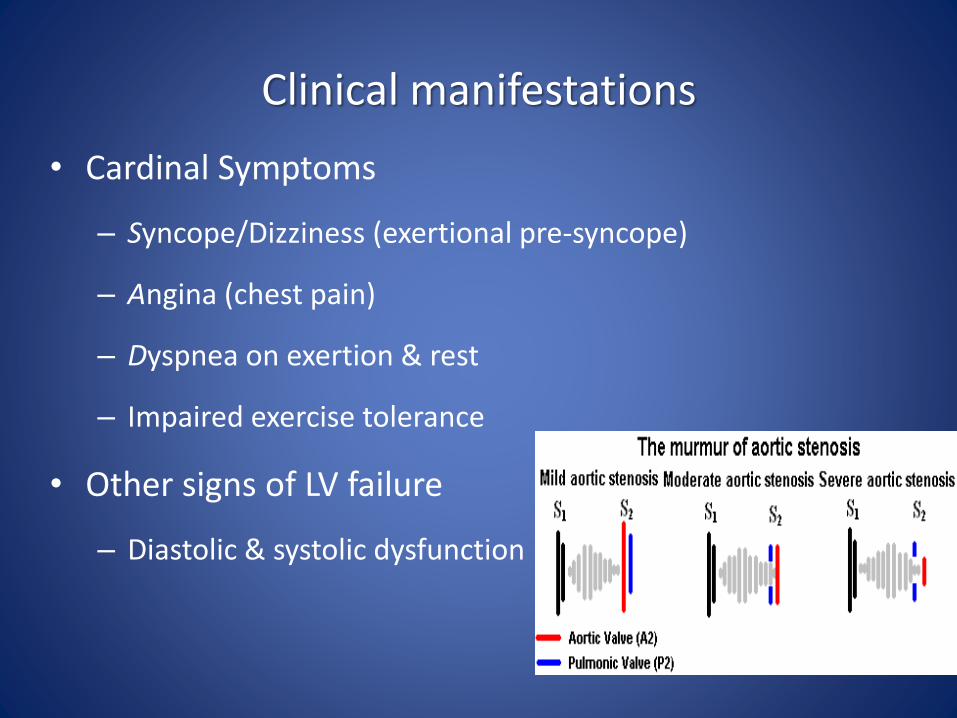
Clinical manifestations
• Cardinal Symptoms
– Syncope/Dizziness (exertional pre-syncope)
– Angina (chest pain)
– Dyspnea on exertion & rest
– Impaired exercise tolerance
• Other signs of LV failure
– Diastolic & systolic dysfunction
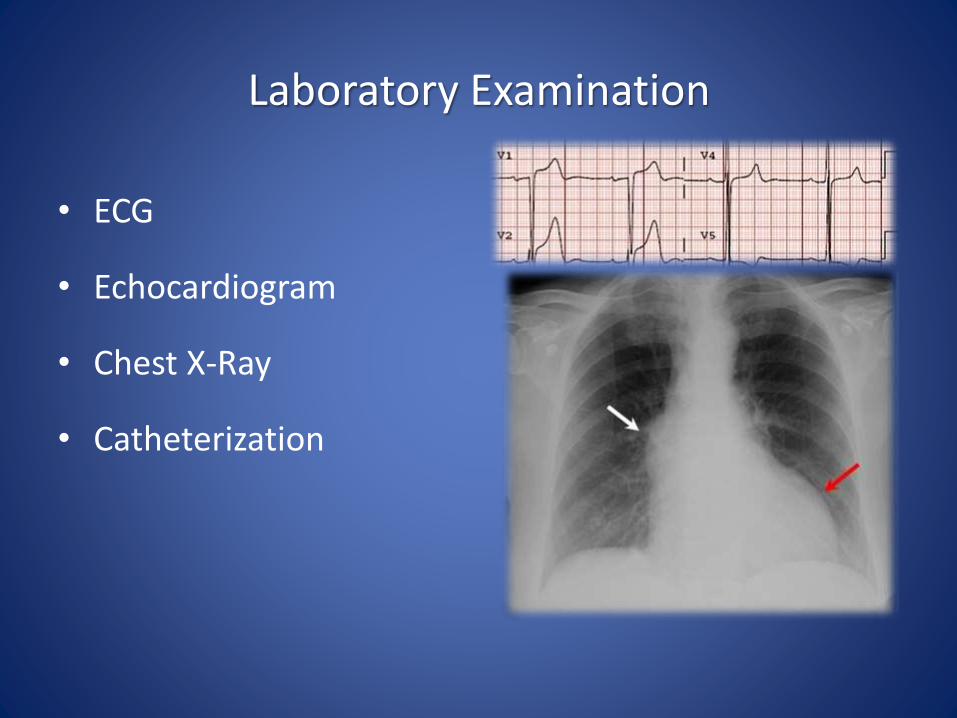
Laboratory Examination
• ECG
• Echocardiogram
• Chest X-Ray
• Catheterization
Treatment
Medical treatment
• Prophylaxis against infective endocarditits
• Diminished cardiac reservation
• Digoxin
• Diuretic
• Salt restriction
• Aortic root dilation
• Beta blocker
• Avoid strenuous physical activity
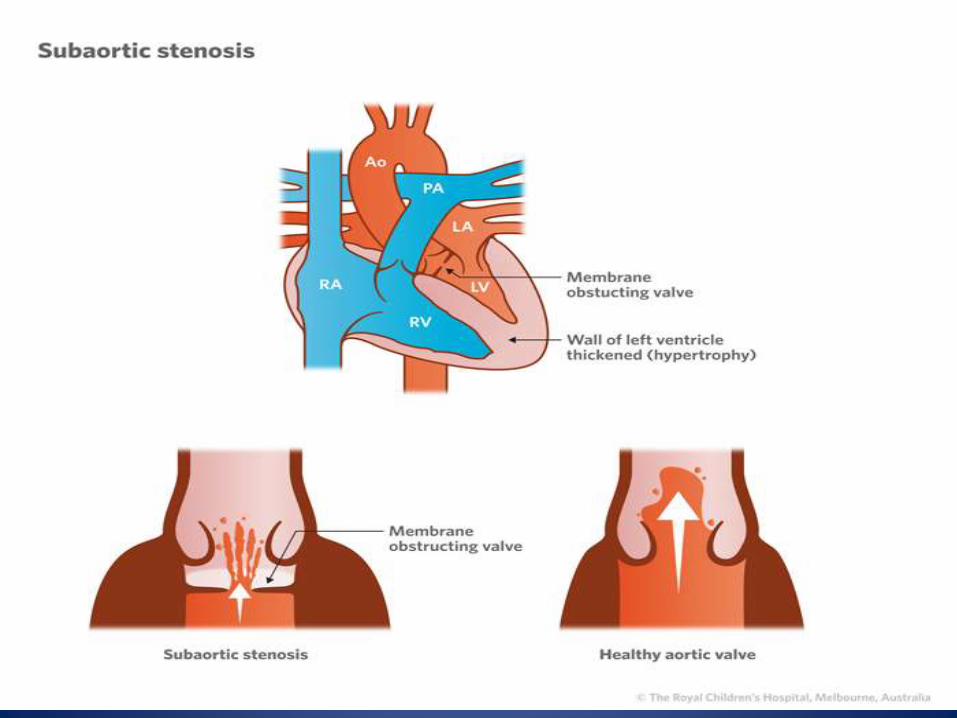
Subaortic stenosis
• The most common form is idiopathic hypertrophy
• The discrete form consists of a membranous diaphragm or fibromuscular ring encircling the LV outflow tract just beneath the base of the aortic valve.
• Treated by complete excision of the membrane or fibromuscular ring
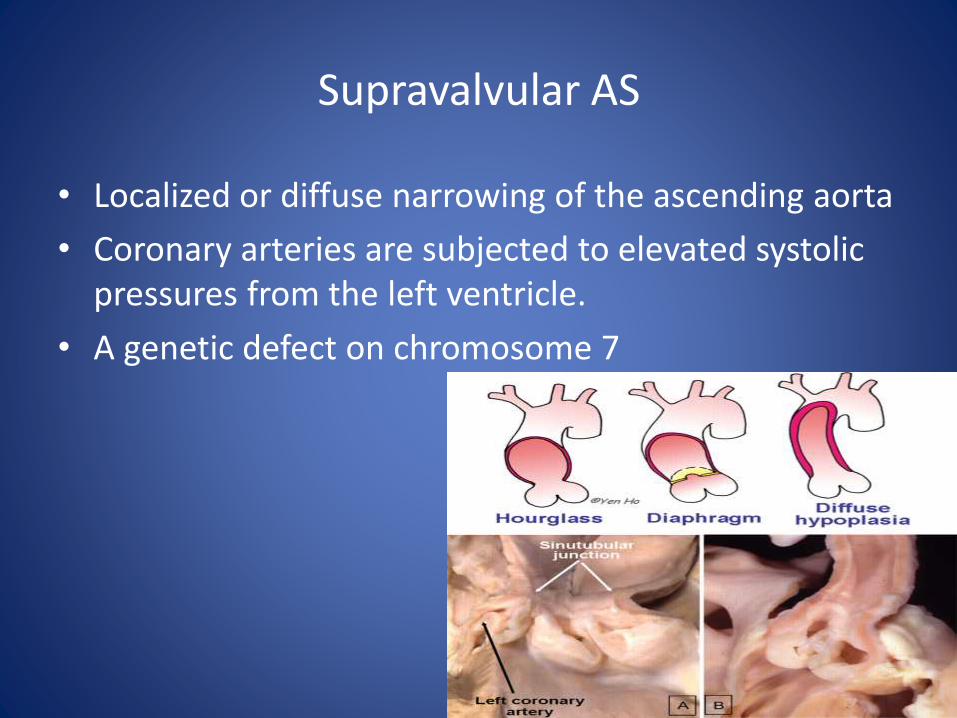
Supravalvular AS
• Localized or diffuse narrowing of the ascending aorta
• Coronary arteries are subjected to elevated systolic pressures from the left ventricle.
• A genetic defect on chromosome 7
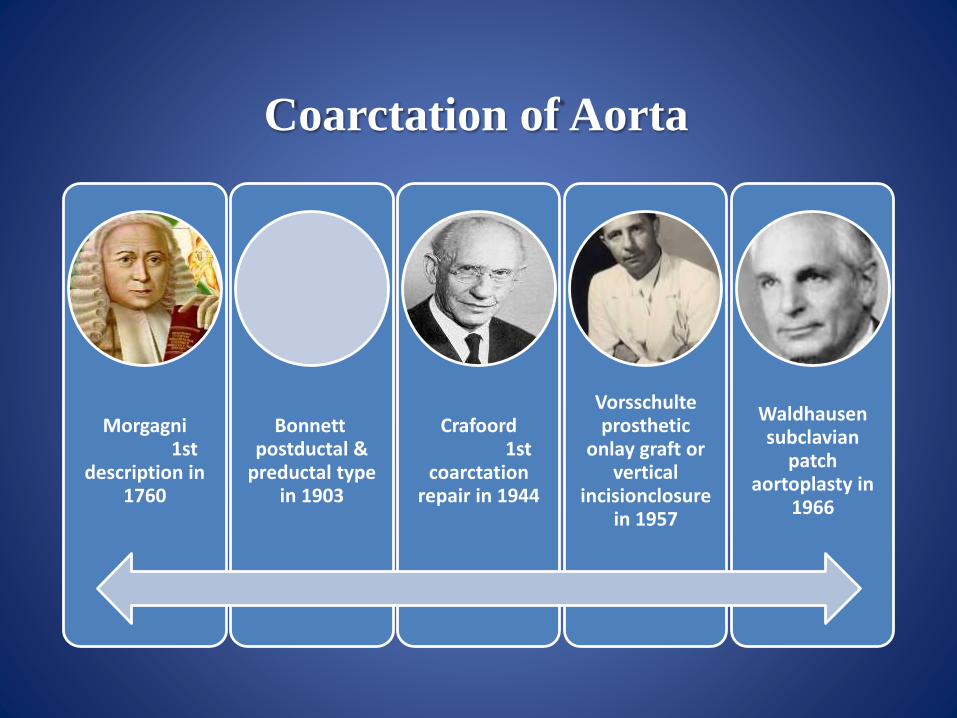
Coarctation of Aorta
Morgagni1st
description in 1760
Bonnettpostductal &
preductal type in 1903
Crafoord1st
coarctationrepair in 1944
Vorsschulteprosthetic
onlay graft or vertical
incisionclosure in 1957
Waldhausensubclavian
patch aortoplasty in
1966
Coarctation of the Aorta
• May occur anywhere along aorta length
• Occurs in ~7% of patients with CHD
• M>F
• Frequent in patients with gonadal dysgenesis
• manifestations depend on
– Site and extent of obstruction
– associated cardiac anomalies
• Circle of Willis aneurysms may occur in up to 10%
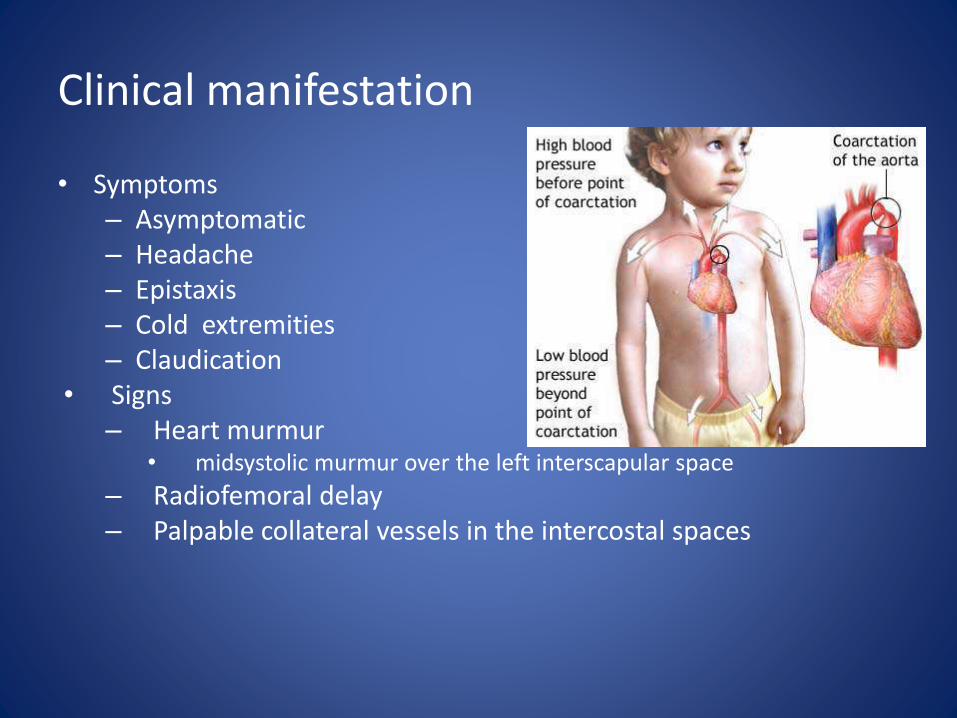
Clinical manifestation
• Symptoms– Asymptomatic– Headache – Epistaxis– Cold extremities– Claudication
• Signs– Heart murmur
• midsystolic murmur over the left interscapular space
– Radiofemoral delay– Palpable collateral vessels in the intercostal spaces
Complications
• Chief hazards of proximal aortic severe hypertension include:
– cerebral aneurysms and hemorrhage
– aortic dissection and rupture
– premature coronary arteriosclerosis
– LV failure
– infective endarteritis
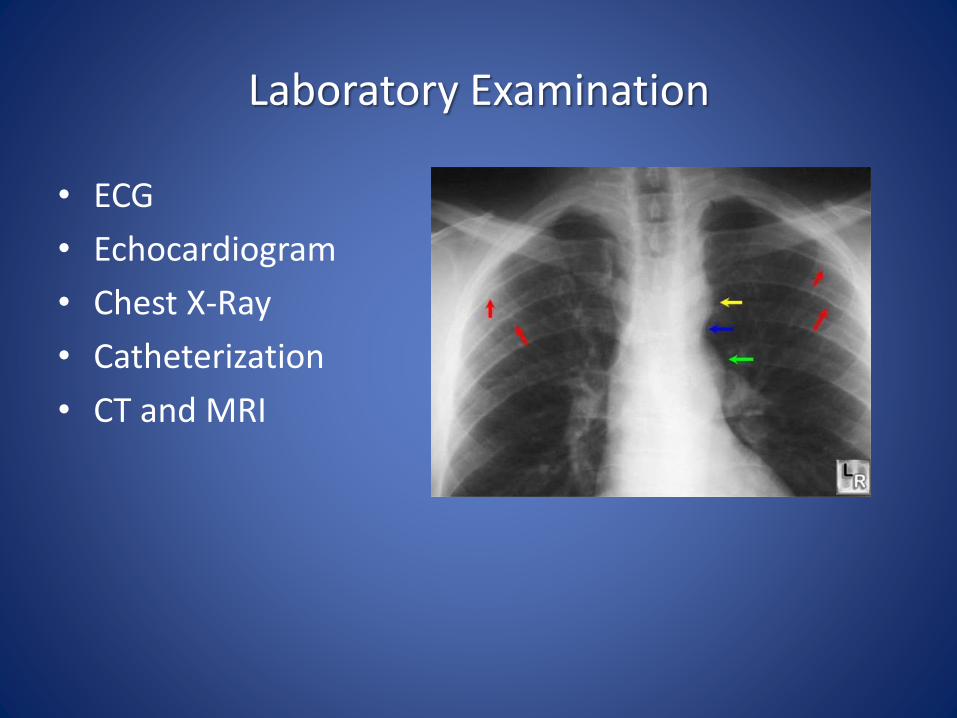
Laboratory Examination
• ECG
• Echocardiogram
• Chest X-Ray
• Catheterization
• CT and MRI
Treatment
• Treatment is usually surgical.
• percutaneous catheter balloon with stent dilatation
• Follow-up of rest and exercise blood pressures is important
• excessive systolic hypertension is seen during exercise, in part due to a diffuse vasculopathy.
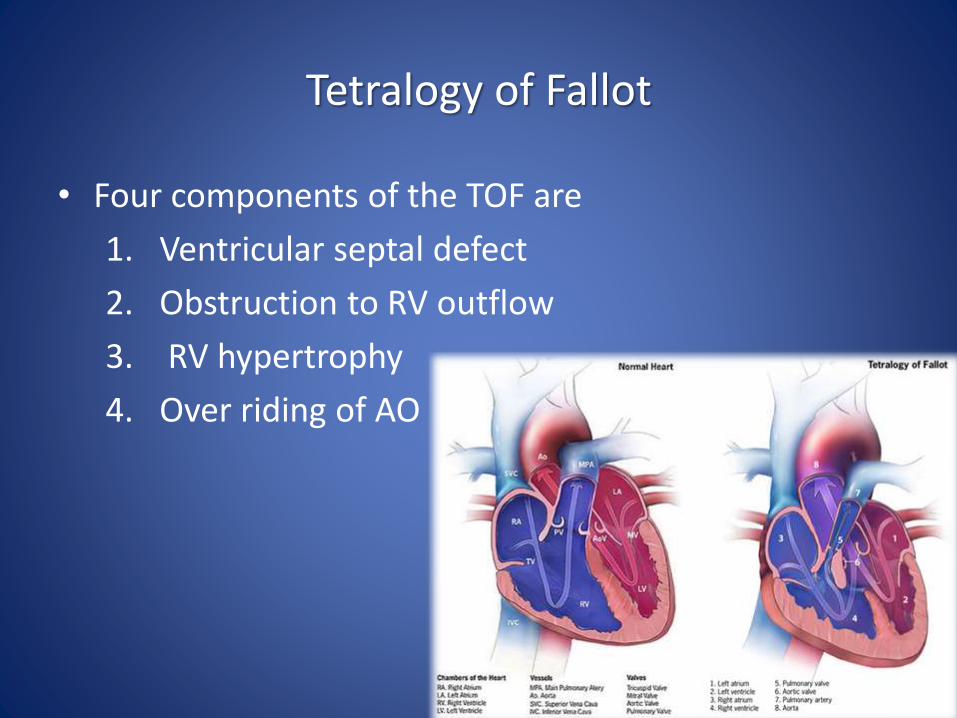
Tetralogy of Fallot
• Four components of the TOF are
1. Ventricular septal defect
2. Obstruction to RV outflow
3. RV hypertrophy
4. Over riding of AO
History
• Cyanosis during feeding
• Poor feeding
• fussiness, tachypnea, and agitation.
• Birth weight is low.
• Growth is retarded.
• Development and puberty may be delayed.

Clinical manifestation
• Clinical presentation is determined by RV outflow obstruction
• Symptomatic any time after birth
• Paroxysmal attacks of dyspnea
– Anoxic spells
– Child cry
– Dyspnea
– Blue
– Lose conscious
– Convulsion
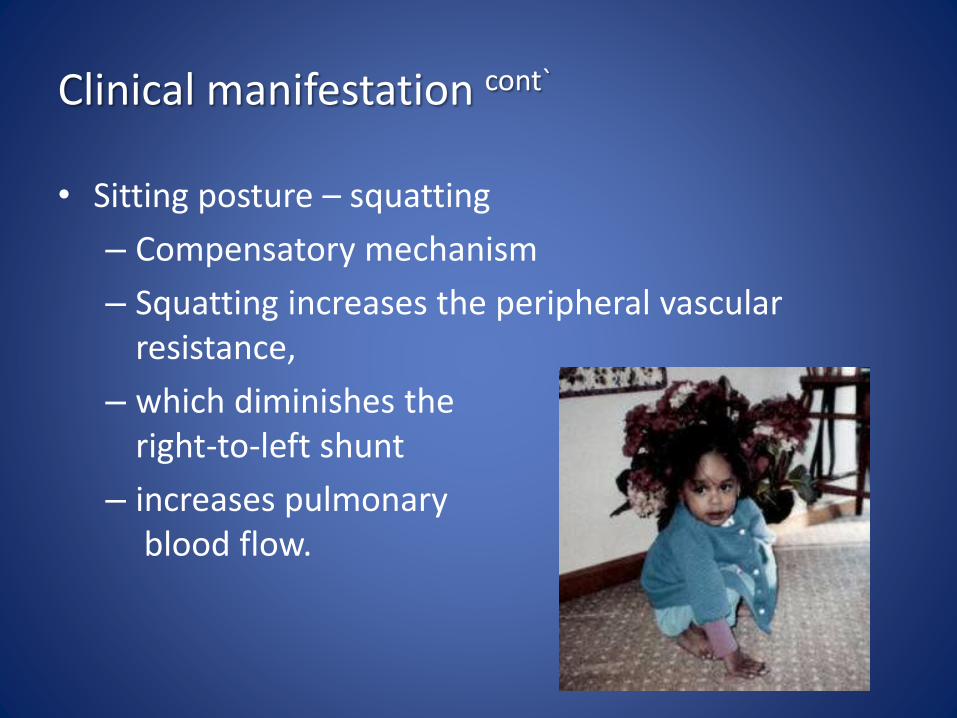
Clinical manifestation cont`
• Sitting posture – squatting
– Compensatory mechanism
– Squatting increases the peripheral vascular resistance,
– which diminishes the right-to-left shunt
– increases pulmonaryblood flow.
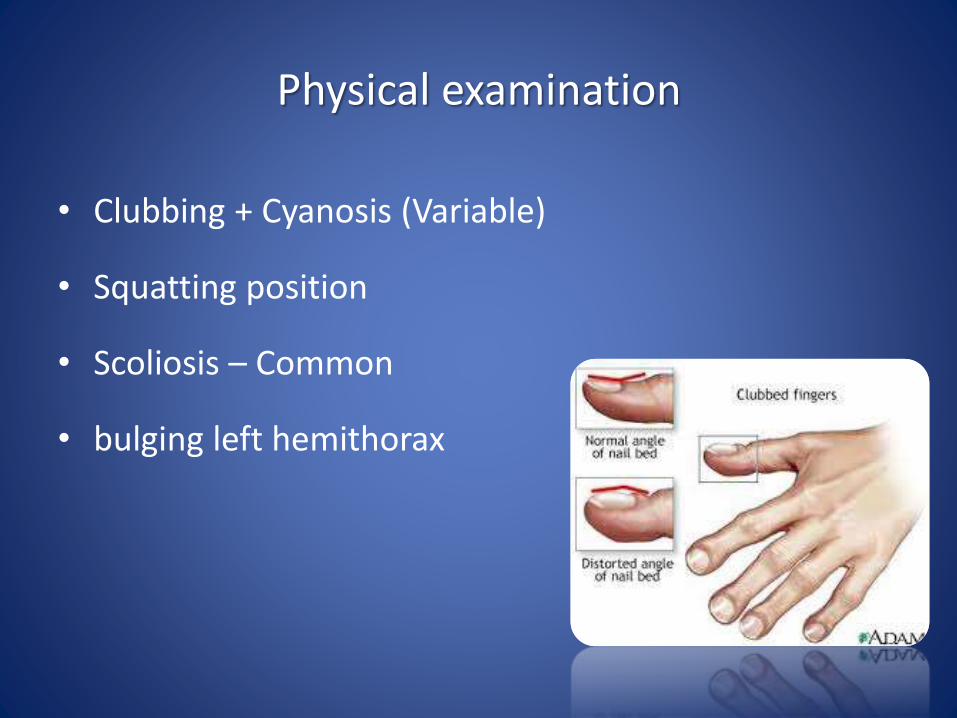
Physical examination
• Clubbing + Cyanosis (Variable)
• Squatting position
• Scoliosis – Common
• bulging left hemithorax
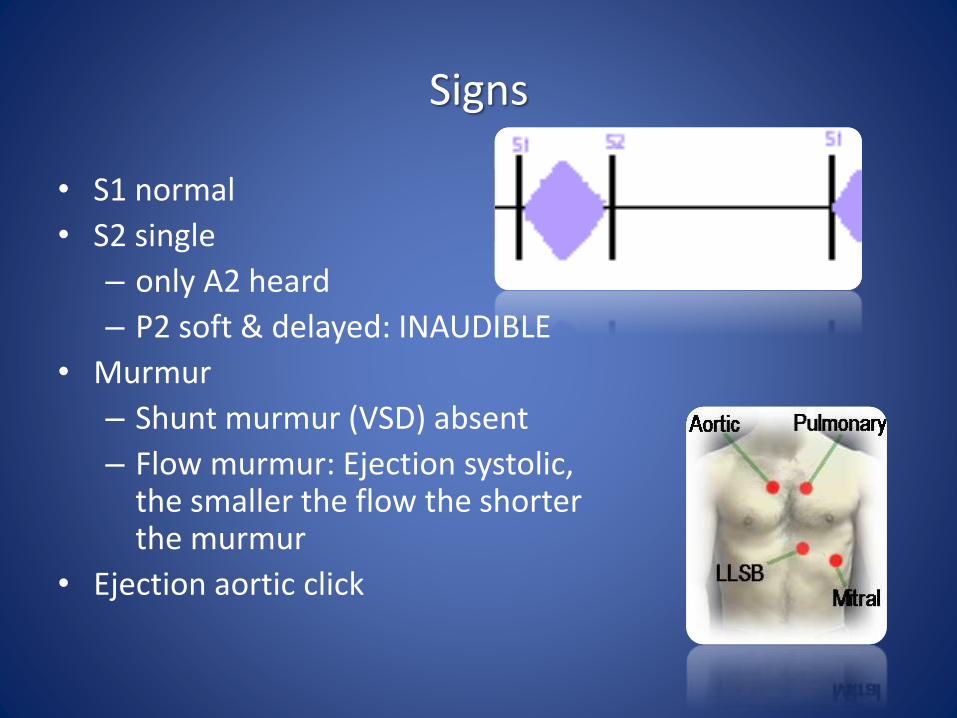
Signs
• S1 normal
• S2 single
– only A2 heard
– P2 soft & delayed: INAUDIBLE
• Murmur
– Shunt murmur (VSD) absent
– Flow murmur: Ejection systolic, the smaller the flow the shorter the murmur
• Ejection aortic click
ECG
•ECG
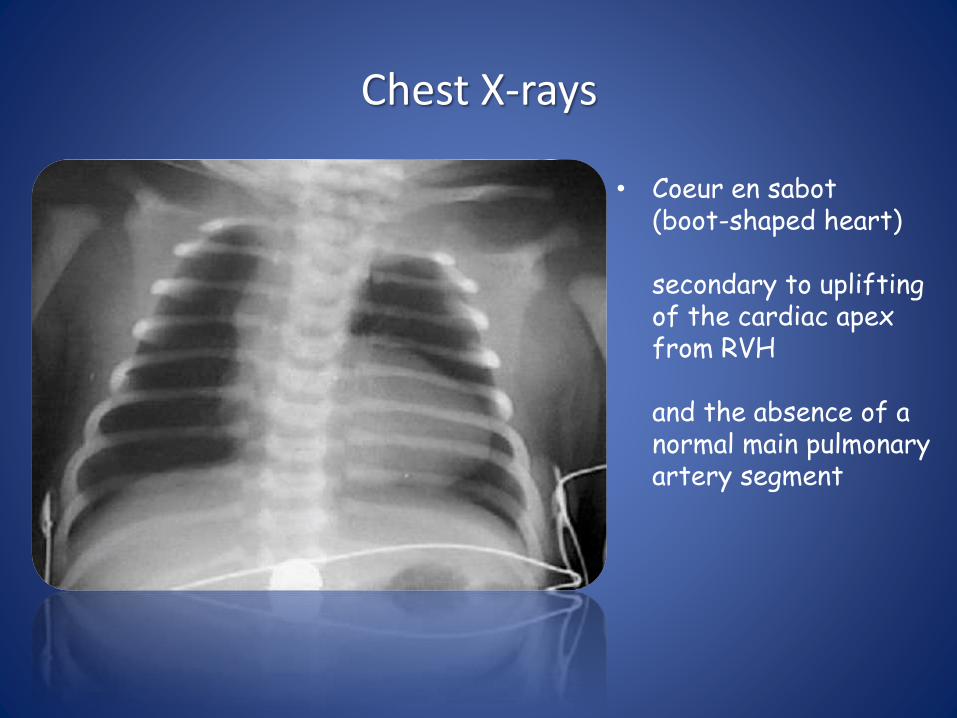
Chest X-rays
• Coeur en sabot (boot-shaped heart)
secondary to uplifting of the cardiac apex from RVH
and the absence of a normal main pulmonary artery segment
Chest X-rays
• Normal heart size due to the lack of pulmonary blood flow and congestive heart failure
Chest X-rays
• Decreased pulmonary vascularity
Chest X-rays
• Right atrialenlargement
• Right-sided aortic arch (20-25% of patients) with indentation of leftward-positioned tracheobronchialshadow
Echocardiography
• Reveals a large VSD
• overriding aorta
• variable degrees of right ventricular outflow tract
(RVOT) obstruction
Course and Complication
1) Each anoxic spell is potentially fatal
2) Polycytemia
• Cerebrovascular thrombosis
3) Anoxic infaction of CNS
• Neurological complication
Management of anoxic spell
1) Knee chest position
2) Humified O2
3) Be careful not to provoke the child
• Especially you are bad at gaining IV access
• Permit the baby to remain with mother
4) Morphine 0.1 -0.2 mg/Kg Subcutaneous
5) Correct acidosis – Sodium Bicarb IV
6) Propanolol
1) 0.1mg/kg/IV during spells
2) 0.5 to 1.0 mg/kg/ 4-6hourly orally
7) Vasopressors: Methoxamine IM or IV drip
8) Correct anemia
9) GA is the last resort
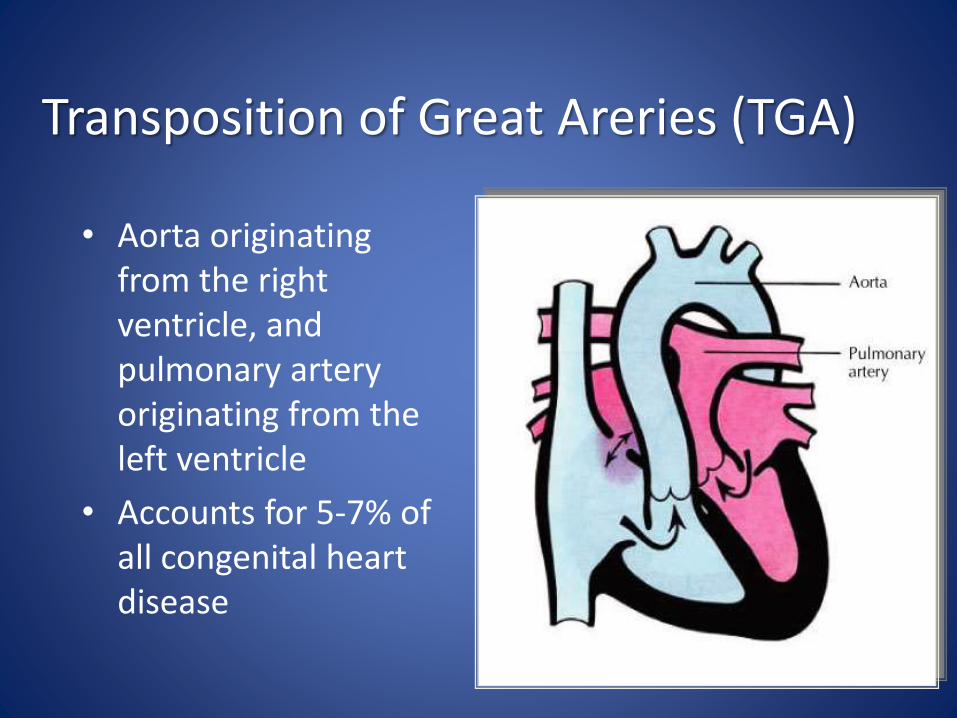
Transposition of Great Areries (TGA)
• Aorta originating from the right ventricle, and pulmonary artery originating from the left ventricle
• Accounts for 5-7% of all congenital heart disease
TGA
• Survival is dependent on the presence of mixing between the pulmonary and systemic circulation
• Atrial septal defect is essential for survival
• 50% of patients have a VSD
• Usually presents in the first day of life with profound cyanosis
• More common in boys
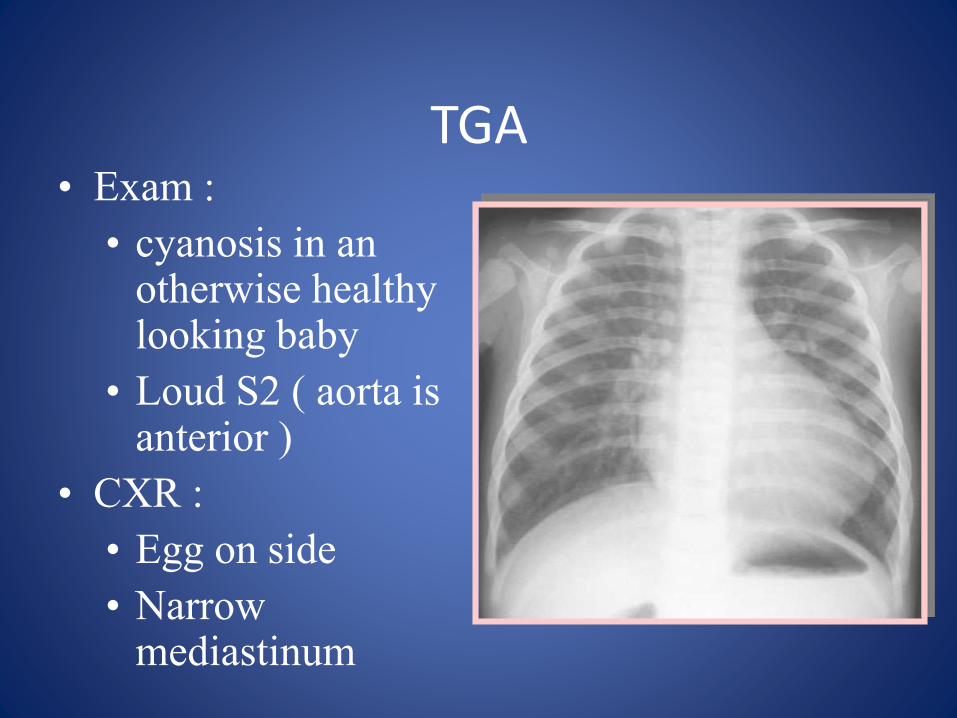
TGA• Exam :
• cyanosis in an otherwise healthy looking baby
• Loud S2 ( aorta is anterior )
• CXR :
• Egg on side
• Narrow mediastinum
TGA .. Acute Management
• PGE-1 with no supplemental O2
Maintain ductus arteriosus patency, this will increase the effective pulmonary blood flow, and thence increase the left atrial pressure, therefore inhance the left to right shunt at the atrial level
• Balloon atrial septostomy
Life saving procedure in the presence of inadequate atrial septal defect
TGA .. Surgical Management
• Arterial switch
– with re-implantation of the coronary artery to the new aortic site.
• Atrial switch :
– Redirecting the pulmonary and systemic venous return to result in a physiologically normal state
– The right ventricle remains the systemic ventricle
– Rarely needed












