Embed Size (px)
Citation preview

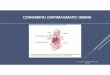
CONGENITAL DIAPHRAGMATIC
HERNIA

DEFINATION
• Congenital diaphragmatic hernia (CDH) is a structural birth defect characterized by protrusion of abdominal viscera into the thorax through an abnormal opening or defect that is present at birth

HISTORY• Diaphragmatic hernia was first described by Ambrose Pare
in the late 16th century• The first published case of congenital diaphragmatic hernia
in a child appeared in the early 18th century• The first report of a successful surgical repair was not until
the early 20th century.• Nearly 25 years later, Hedblom published a large series of
patients who underwent surgical repair for diaphragmatic hernia, concluding that early surgery would improve survival.
• Bowditch was the first to make the bedside diagnosis of CDH
• Successful repair of CDH was first reported by Gross and Ladd in 1940.

EPIDEMIOLOGY
• Incidence- 1 in 2000 to 3500• One third of infants with CDH are still born ( mortality due to other congenital anomalies)• When still born are counted with live births,
females appear to be more commonly inflicted• More common on the left sided.(80%)• B/L CDH are rare and are associated with other
anomalies.

EPIDEMIOLOGY• Infants with isolated CDH are more likely to be
premature, macrosomic and male and one third of affected infants may have associated major defects.
• Women who are thin or underweight for their height may have increased risk of having an infant with an isolated CDH.
• Recurrence rate in first degree relative 1 in 45 or around 2%
• Chromosomal abnormalities- 9-34%• CDH with abnormal karyotype has been associated
with poor prognosis

ETIOLOGY• Unknown• Exposure to environmental hazards or
pharmacological agents to genetically exposed or susceptible individuals.
• Alteration in retinoid regulated target genes may be responsible for CDH development

ANIMAL STUDIES
• In the 1970s, toxicological studies of the herbicide nitrofen(2,4-dichloro-phenyl-p-nitrophenyl ether) -nitrofen induced developmental anomalies in the lungs, hearts, diaphragm and skeletal tissues of fetuses exposed in utero
• Other related chemicals-– BPCA is a breakdown product of a thromboxane-A2
receptor antagonist– Bisdiamine is a spermatogenesis inhibitor,– SB-210661 is a benzofuranyl urea derivative developed
for inhibiting 5-lipoxygenase

ANIMAL STUDIES• Initial studies into the pathogenesis of the defect
– Abnormal phrenic nerve innervation – Myotube formation were responsible for the diaphragm defect
• Nitrofen studies– Inhibit the retinoic acid synthesizing enzyme, retinol
dehydrogenase-2 (RALDH2)
• Transgenic mice with Fgf10 inactivated do not develop lung tissue
• Despite having essentially no lungs,-Fgf10 null-mutant mice have normal diaphragms.
• Defects in the diaphragm can be induced by teratogen exposure in the absence of lung tissue

ANIMAL STUDIES
• PPF defects have been observed in rats bred on a Vitamin A-deficient diet and mice with a functionally inactivated wt1 gene—both of which also have Bochdalek CDH
• The PPF is best visualized at E13.5 of rat gestation. In nitrofen-exposed fetuses examined at this age, it is clear that the postero-lateral portion of the PPF is malformed

ANIMAL STUDIES
• Nonclosure of the PPCs or • Defect in muscularization gives rise to the hole in
the diaphragm.• The PPF mesenchyme forms between the 5th and
7th weeks of gestation in humans, before closure of the PPC and muscularization of the diaphragm;

ANIMAL MODEL

ANIMAL STUDIES
• Central to this hypothesis is the PPF, a transient structure which forms early in diaphragm development and is the target for migratory muscle precursor cells(MMC) and the phrenic nerve.
• Evidence from animal models– It is a malformation of the nonmuscular component of the PPF that underlies the defect in the mature diaphragm.

ASSOCIATIONS• Incidence 10-50%• Skeletal defects-32%
– Limb reductions– Costovertebral defects
• Cardiac anomalies-24%– Left ventricular hypoplasia with hypoplasia of the left
aortic arch– Other outflow defects- VSD,TOF,TGA,double outlet
right ventricle and aortic coarctation• Anatomical anomalies of the tracheobronchial
tree-18%– Congenital tracheal stenosis– Tracheal bronchus– Trifurcated trachea

ASSOCIATIONS
• Secondary Defects– Lung hypoplasia– Abnormalities in cardiac position and patent ductus
arteriosus – Intestinal malrotation
• Nonhernia-related anomalies -73% – Central nervous system– Cardiovascular system– Genitourinary and gastrointestinal systems

CDH-ASSOCIATED GENETIC SYNDROMES
• Fryns – Diaphragmatic defects, coarse facial features, abnormal
ear/nose, cleft lip and palate, micrognathia, genitourinary/renal anomalies, CNS anomalies, distal digital hypoplasia
• Donnai-Barrow– Diaphragmatic hernia, omphalocele, hypertelorism, absent
corpus callosum, myopia, severe sensorineural hearing loss• Thoracoabdominal• Craniofrontonasal• Cornelia de Lange• Beckwith-Wiedemann• Simpson-Golabi-Behmel

SPECIFIC CDH-RELATED GENES
• COUP-TFII (15q26)-Recurrently deleted in CDH
• WT1 (11p13)-Recurrently deleted in CDH • SLIT3 (5q35 ) Recurrently deleted in CDH • FOG2 (8q22)-Recurrently deleted in CDH

RECURRENCE
• Isolated-CDH, with a negative family history, the recurrence risk for future pregnancies -2%
• Positive family history, a specific genetic syndrome, or a chromosomal abnormality -50% recurrence risk for CDH or other congenital defects.

ASSOCIATIONS• Still born group
– Neural tube defects– Anencephaly– Myelomeningocele– Hydrocephalus– Encephaloceles
• Those who survive to birth– Neural tube defects– Cardiac defects– Esophageal atresia,Omphalocele and cleft
palate

EMBRYOLOGY• Four distinct components• The anterior central tendon forms from the septum
tranversum• The dorsolateral portions from the pleuroperitoneal
membranes• The dorsal crura from the esophageal mesentery• The muscular portions from the thoracic intercostal muscles

DIAPHRAGM

LUNG DEVELOPMENT
• Embryonic phase• Pseudoglandular phase• Canalicular phase• Saccular phase• Alveolar phase

EMBRYONIC PHASE
• 3rd Week-Formation of a diverticulum off the caudal end of the laryngotracheal groove
• 4th week- trachea and two primary lung buds forms
• 6th week-lung buds develop into defined lobar structures

PSEUDOGLANDULAR
• 7th – 16th week- lung airway differentiation
• All bronchial airways develop• Preacinar vascular development is
completed by 16 weeks

CANALICULAR
• 16th – 24th week-air space development occurs as crude alveolar air sacs begin to take shape
• Type 1 pneumocytes begin to differentiate• Type 2 pneumocytes begin to appear• Gas exchange becomes functional

SACCULAR
• 24th weeks to term-Maturation of crude alveolar air spaces
• Continued remodelling of the air space dimensions and maturation of surfactant synthesis

ALVEOLAR
• After birth- Mature adult like alveoli begin to appear
• Extensive alveolar maturation and multiplication takes place from birth until 8 years of life
• Some think alveolar formation may be completed by 2 years

PATHOLOGY• If closure of the pleuroperitoneal canal has not
occurred by the time midgut returns to the abdomen during gestation 9-10 week.
• The resulting abnormal position of the bowel prevents its normal counterclockwise rotation and fixation
• No hernial sac is present if the event occurs before the complete closure of the pleuroperitoneal canal
• Non muscularised membrane forms a hernial sac in 10-15% of cases

PATHOLOGY• CDH defects usually features a completely open space between the abdomen and
the chest although some may have a membrane of pareital pleura and peritoneum acting as a hernia sac
• Hernial contents may include left lobe of liver,spleen,stomach,entire GIT.
• The hepatic veins may drain ectopically into the right atrium and fibrous fusion between the liver and the lung.
• U/L visceral herniation affects both the I/L and C/L pulmonary development, although hypoplasia is predictably more on the I/L side

VASCULAR PATHOLOGY• Pulmonary vascular bed is distinctly abnormal in lungs from
patients wth CDH.• Significant adventitial and medial wall thickening has been
noted in pulmonary arteries in all sizes in CDH with abnormal muscularisation of the small preacinar and intraacinar arterioles
• Increased susceptibility to fixed and intractable pulmonary hypertension.
• Increased adventitial thickness of pulmonary veins has been noted in CDH infants which is secondary to pathology or treatment of pulmonary HT

DIAGNOSIS
• Prenatal USG- 40-90% of cases• As early as 11 weeks with mean gestational age -24
weeks• Polyhyramnios -80% of CDH(Kinking of
gastroesophageal junction)• Finding
– Stomach or fluid filled loops of intestine in the fetal thorax at the same cross section as the heart
– Absence of stomach in the abdomen– Presence of liver or any other solid viscera in the thorax
with or without rightward mediastinal shift.

Fetal MRI
• Poor accoustic contrast between fetal lung and herniated viscera
• Assess liver position with respect to diaphragm
• Assess lung volume and pulmonary hypoplasia

SYMPTOMS• Spectrum
– Degree of Pulmonary Hypoplasia– Reactive Pulmonary hypertension
• Respiratory Distress– At Birth( Majority first 24 hrs)– Cyanosis,gasping,sternal retractions and poor respiratory
effort• Scaphoid Abdomen• Asymmetrical distended chest• Absent breath sounds I/L side• Mediastinal compression

LATE PRESENTATION
• 10-20% • Recurrent respiratory illness• Chronic pulmonary disease• Pneumonia• Effusion• Empyema• Gastric Volvulus

RADIOGRAPHY
• Loops of intestine in the chest
• Location of the gastric bubble
• Shifting of the cardiac silhouette into the C/L side

DIAGNOSIS
• Renal and Cranial USG• ECHO

DIFFERENTIAL DIAGNOSIS
• Eventration of Diaphragm• Anterior Diaphragm Hernia of
Morgagni• Congenital Esophageal Hiatal Hernia• Congenital Cystic Disease of Lung• Primary Agenesis of Lung

PROGNOSTIC FACTORS• Anatomic factors
– Lung to head ratio(LHR< 1.0)– Analysis of Cardiopulmonary structure
• Cardioventricular index( LV/RV)• Cardiovascular index(Ao/PA)• Modified McGoon Index(Combined diameter
of hilar pulmonary arteries indexed to descending aorta) A modified McGoon index equal to or less than 1.3 predicted mortality with a sensitivity of 85% and specificity of 100%

PROGNOSTIC FACTORS• Physiological Parameters• Arterial blood gas
– Alveolar arterial oxygen gradient(AaDo2)• AaDo2 = [(713 X FiO2) - PaCO2/0.8] - PaO2
– Ventilatory Index• VI = (RR X MAP X PaCO2)
– Modified ventilatory Index• MVI = (RR X PIP X PaCO2) + 1000
– Oxygenation Index• OI = (MAP X FiO2/PaO2)

PROGNOSTIC FACTORS
• Pulmonary Function Test– Compliance
• >0.25 mL/cm H2O/kg– Initial Tidal Volume
• >3.5 mL/ kg– Functional Residual Capacity

MANAGEMENT• Prenatal Care• Preoperative Care
– Resuscitation– Ventilation– Pharmacology– Surfactant– Nitric Oxide
• Surgical Management• Post operative Management

PRENATAL CARE• Search for other congenital
anomalies• Karyotype evaluation• Reference to appropriate tertiary
care centre• Spontaneous vaginal delivery• Fetal intervention is investigational
and highly experimental

PRENATAL PREDICTION OF SURVIVAL IN FETAL CDH
• The position of the liver (“liver-up versus “liver-down”).– Current survival rate for liver-up CDH is around 50%.– The incidence of liver herniation is unknown, but up to
75% of CDH patients have some portion of the liver in the chest.
– Degree of liver herniation (mean liver/diaphragm ratio was significantly higher in the survivors compared with the non-survivors)
• Sonographic measurement of the right lung area-to-head circumference – (LHR is a sonographic measurement of right lung size
standardized to head circumference in left-sided CDH)

OTHER PREDICTORS• Three-dimensional measurement of lung volume by
fetal MRI.– High risk group with Lung vol<10 ml at 28WG or vol<25 ml
at 34WG• Three dimensional sonography• Measurement of pulmonary artery diameters.• Physiological assessment of fetal lung function is
ideal but limited– Pulmonary vascular function. – The pulmonary arterial pulsatility index with or without
maternal oxygen supplementation

PRENATAL INTERVENTION• Open fetal operation
– Maternal laparotomy, – Hysterotomy, and – Fetal laparotomy/thoracotomy– Successful repair was possible in fetuses with liver down
CDH• Therapeutic tracheal occlusion (TO)
– Increased lung tissue stretch (turns on mechano-transduction pathways resulting in lung growth
– Fetal lung growth in normal and CDH animal models– Increased number of alveoli accompanied by an
appropriate increase in capillary vessels– Remodeling of pulmonary arterioles which is likely to
ameliorate pulmonary hypertension

PRENATAL INTERVENTION
• Video and ultrasound-assisted fetal endoscopy “FETENDO clip”.– High rate of preterm delivery – Irreversible damage to the laryngeal nerve and
trachea• (FETENDO-balloon)
– Single 10-Fr cannula and a 1.2-mm fetoscope without maternal laparotomy under regional anesthesia

FETENDO V/s OPEN FETAL• FETENDO was less invasive compared with open fetal
surgery comparing – Cesarean delivery as delivery mode (58.8% versus 94.8%)– Requirement for intensive care unit stay (1.4% versus
26.4%), – Length of hospital stay (7.9 days versus 11.9 days)
• No differences– Requirement for blood transfusions (2.9% versus 12.6%). – Premature rupture of membranes(44.1% versus 51.9%), – Pulmonary edema (25.0%versus 27.8%)– Placental abruption (5.9% versus 8.9%),– Preterm delivery (26.5% versus 32.9%)– Interval from the procedure to delivery (6.0 weeks
versus 4.9 weeks) between FETENDO and open Sx.Golombeck K, Ball RH, Lee H, et al. Maternal morbidity after maternal-fetal
surgery. Am J Obstet Gynecol 2006;194:834-9.

LIMITATIONS OF FETO
• Lung growth response to TO was variable• Pulmonary function of the newborns treated with
TO was abnormal even when dramatic lung growth was observed in utero
• The mere distention of the existed lung air space can cause marked increase in LHR
• Prolonged TO reduces the number of type II cells, resulting in surfactant depletion
• Flake AW, Crombleholme TM, Johnson MP, et al. Treatment ofsevere congenital diaphragmatic hernia by fetal tracheal occlusion:clinical experience with fifteen cases. Am J Obstet Gynecol 2000;183:1059-66

PREOPERATIVE CARE• Resuscitation
– Physiological Emergency rather than a surgical emergency• Pulmonary hypoplasia• Reversible pulmonary hypertension
– Monitoring arterial oxygen saturation– Proper temperature regulation, glucose
hemostasis and volume status– Metabolic Acid Base

PREOPERATIVE CARE• Ventilation• Pressure Cycle Ventilator
– 100 breaths/min, PAP - 18-22 cm H2O , No PEEP
– 20-40 breaths/min, PAP- 22-35 H2O , 3-5 cm PEEP
• Goal Of Ventilation – Pa O2 > 60 mm Hg( Sa O 2 90%-100%)– P Co2 < 60 mm Hg

ROLE OF ECMO• Inclusion criteria for ECMO
– Oxygenation index (OI) > 25-40– Pa O2 postductally < 40 mm Hg over 2 hrs– Pa O2 preductally < 50 mm Hg over 2-4 hrs– Pa O2 postductally < 50 mm Hg over 12 hrs– Pa CO2 > 70 mm Hg under HFOV– Severe barotrauma/air leak, and/or refractory hypercarbia
• Exclusion criteria for ECMO – Prematurity (GA <34 weeks)– Weight below 2 kg– Intracranial hemorrhage and – Contraindication to anticoagulation.– Irreversible organ failure

QUESTIONS WITH ECMO
• Timing of repair• Complications of ECMO• Role of surfactant and Liquid lung
distension with ECMO• Role of HFOV with ECMO

PREOPERATIVE CARE• Pharmacology• Decrease pulmonary hypertension
– NTG, Nitroprusside, Isoproterenol, Captopril
• New Management strategies– Calcium channel blockers, Prostacyclin
derivatives, endothelin receptors antagonist, Phosphodiesterase-5 inhibitors

SURGICAL MANAGEMENT
• In 1940, Ladd and Gross stressed the importance of early surgical therapy for CDH patience.
• The paradigm shift from emergent to delayed repair occurred in 1987( Sakai et al).

END POINT OF PREOPERATIVE STABILISATION
• Hemodynamically stability• Acid-base status within the normal
physiological range• Minimal ventilatory support• Resolution of pulmonary hypertension• Improvement in pulmonary compliance• Resolving pulmonary radiographic
abnormalities

SURGICAL APPROACH• SMALL
– Closed primarily with nonabsorbable suture• LARGE
– Prosthetic materials:• Polytetrafluoroethylene (PTFE) (Gore-Tex)• Polypropylene (Marlex)• Dacron
– Muscle flaps:• Abdominal muscles• Latissimus dorsi• Latissimus dorsi and serratus anterior
– Bioactive Materials:• Surgisis

TUBE THORACOSTOMY
• Indication– Draining significant hemorrhage– Uncontrolled air leak– Chylothorax, pneumothorax or a– Large pleural effusion.
• Disadvantage– Contra- and ipsilateral iatrogenic pulmonary
injury via mediastinal shift after pleural suction and

MINIMAL INVASIVE SURGERY• Thoracoscopic approach
– Intraabdominal stomach– Minimal ventilator support (PIP <24)– No evidence of pulmonary hypertension
• Disadvantages• High failure rate (14%)• Prohibitive increases in PCO2• Acidemia• Gut cannot be deflated and controlled intarabdominally• Stretching and abdominally patching cannot be performed.

RECURRENT HERNIATION• Recurrent herniation is noted in up to 22% of CDH
survivors.• It is seen more frequently in those patients with
very large defects and requiring patch repair of the diaphragm.
• Recurrent herniation usually presents before 3 years of age,
• Some have described a bimodal distribution of recurrence with – 14% prevalence-( 1 and 3 months) – 28% prevalence-( 10 and 36 months).

SURGERY FOR RECURRENCE
• Optimal timing• Prompt repair,
– Minimizing the risk of incarceration.– Early repair in a newborn could be high risk
• Delayed Repair– Close followup, particularly if the patient is
without serious symptoms secondary to the re-herniation.

EVENTRATION OF DIAPHRAGM
• It is characterized by incomplete muscularization of the diaphragm, allowing the abdominal contents to protrude into the thoracic cavity in the areas where no muscle has formed, and the diaphragm is subsequently weaker.
• It may be congenital or acquired.

EVENTRATION OF DIAPHRAGM
• First noted in 1774 when Jean Louis Petit noted it on a postmortem examination
• It accounts for 5% of all diaphragmatic anomalies.
• most commonly unilateral with only a few bilateral cases
• The involvement of the diaphragm can be total or partial

ASSOCIATIONS
• Abnormal pulmonary segmentation, • Congenital heart disease• Chromosomal anomalies

CLINICAL MANIFESTATIONS• Respiratory symptoms
– Cyanosis– Dyspnea,– Repeated attacks of pneumonitis– Decreased exercise tolerance.
• Gastrointestinal symptoms – Difficulty feeding– Failure to thrive– Regurgitation– Nausea and heartburn– Complete gastric volvulus

INDICATION
• Large functional deficit in the function of the I/L lung on ventilation/perfusion studies
• Asymptomatic

MANAGEMENT
• Abdominal or Thoracic approach• Thoracoscopic or Laparoscopic
approach• Plication of diaphragm

MORGAGNI HERNIA
• Morgagni, retrosternal, or parasternal hernia.• This rare anterior defect of the diaphragm occurs
through the space of Larrey• Only 5% of all CDH cases. • Incidence among children with Down’s syndrome
may be as high as 1:1000.• It is characterized by herniation of abdominal
contents through the foramen of Morgagni; small triangular areas of the diaphragm adjacent to the lower end of the sternum.

SIGNS AND SYMPTOMS
• Usually present in older children or adults• Typically a sac is present which includes
the small intestine or colon• Associated anomalies may include
malrotation

MANAGEMENT
• Upper transverse incision• The diaphragm is sutured to underside of
the posterior rectus sheath at the costal margin after reduction of the hernia and resection of the sac.
• Thoracoscopic or laparoscopic approach are also used

CENTRAL TENDON DEFECT
• Central tendon defects are characterized by congenital herniation of abdominal contents through the central tendon ofthe diaphragm.
• The embryogenesis of this defect is poorly understood; – Failure to form, rupture, or stretching of the
central tendon due to an underlying weakness have all

LONG TERM RESULTS
• Heavily influenced by accompanying congenital morbidity
• Spirometry– Reduced lung capacity– Restricted and obstructive lung functions
• Prone to scoliosis and funnel chest• Neurological development was reduced in 45%• Children grow less and stay behind body weight in
the first 2 years of life.• Persistent pulmonary hypertension

CONCLUSION• Overall survival has reached 80% • Direct result of changes in medical and
surgical management.• Preoperative physiologic stabilization and
subsequent elective repair have become the cornerstones of management

THANK YOU