Embed Size (px)
Citation preview

© Ramaiah University of Applied Sciences
1
Faculty of Dental Sciences
Complications in implantology
Dr. Zeeshan Arif

© Ramaiah University of Applied Sciences
2
Faculty of Dental Sciences
Contents
Classification
Risk factors
Surgical problems
- stage one surgery
--haemorrhage
--edema
--flap dihescence
--implant mobility
--implant location
--problems placing cover screw
--post operative pain
--paraesthesia
--infection
--exposure following placement-stage two surgery--failure to integrate--lack of osseointegration--problems placing abutments--bony defects--painImplant related problems-pain-infectionPeri implant mucositisPeri implantitis-thread exposure-loss of integration
Biomechanical problems-screw fracturesImplant body fracture-prosthesis fractureFunctional problems-appearance-speech -MasticationConclusion References

© Ramaiah University of Applied Sciences
3
Faculty of Dental Sciences
Introduction
• Since the introduction of the concept of osseointegration the
success of implants have increased dramatically
• Endosseous dental implants have been a successful treatment
alternative for restoring missing teeth
• However the treatment is not always successful as the implant is a
foreign body
• The research focus is shifting from description of clinical success to
identifications of factors causing implant failures

© Ramaiah University of Applied Sciences
4
Faculty of Dental Sciences
Classificaton
– Rosenberg et al.classified implant failures as:
1. Infections
2. Traumatic
© Ramaiah University of Applied Sciences
5
Faculty of Dental Sciences
• Esposito et al classified implants according to the Osseointegration
Concept
1. Biological
2. mechanical
3. iatrogenic
4. Inadequate patient education

© Ramaiah University of Applied Sciences
6
Faculty of Dental Sciences
• Truhlar classified failures as
1. Early failures
2. Late failures

© Ramaiah University of Applied Sciences
7
Faculty of Dental Sciences
• Hobo et al. listed out the various complications occurring in implants as follows:

© Ramaiah University of Applied Sciences
8
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
9
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
10
Faculty of Dental Sciences
• According to Cranin

© Ramaiah University of Applied Sciences
11
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
12
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
13
Faculty of Dental Sciences
• El askary et al. have divided the FAILURES into seven categories

© Ramaiah University of Applied Sciences
14
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
15
Faculty of Dental Sciences
Systemic Factors Potential medical risks (Matukas1988):
1. Cardiovascular – Heart failure, CHD, hypertension
2. Respiratory – COPD, Asthma.
3. GIT– Nutritional disorders, Hepatitis malabsorption,
inflammatory bowel disease.
4. Genitourinary – Chronic renal failure.
5. Endocrine – Diabetes, pituitary/adrenal disease.
6. Musculoskeletal, arthritis, osteoporosis.
7. Neurologic – Stroke, Palsy.

© Ramaiah University of Applied Sciences
16
Faculty of Dental Sciences
Absolute Medical Contraindications: -
1. Brittle diabetes
2. Haemophelia
3. Ehler-Dahnlos syndrome
4. Marfan's syndrome
5. Osteoradionecrosis
6. Renal failure
7. Fibrous dysplasia
8. Crohn's Disease

© Ramaiah University of Applied Sciences
17
Faculty of Dental Sciences
Psychological Factors:
1. Lack of support
2. Mental retardation
3. Dementia
4. Psychosis
5. Emotional problems
6. Interpersonal problems
7. Behavioral problems - Problematic attitudes and beliefs.

© Ramaiah University of Applied Sciences
18
Faculty of Dental Sciences
SURGICAL PROBLEMS
STAGE-ONE SURGERY
Haemorrhage
• Excessive haemorrhage usually occurs as a result of involving a blood
vessel or perforating the bony cortex so that the adjacent soft
tissues are traumatized.
• Where this occurs in the mandible distal to the mental foramina the
possibility of damage to the mandibular canal must be considered.
• Prevention of this is based on careful radiographic assessment and
surgical technique.
© Ramaiah University of Applied Sciences
19
Faculty of Dental Sciences
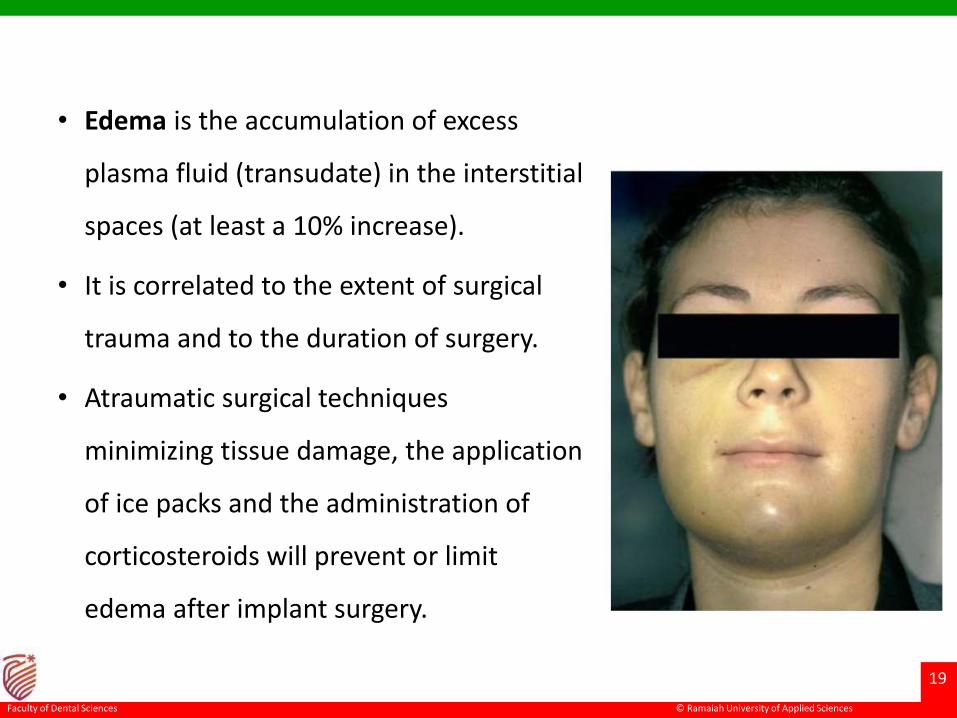
• Edema is the accumulation of excess
plasma fluid (transudate) in the interstitial
spaces (at least a 10% increase).
• It is correlated to the extent of surgical
trauma and to the duration of surgery.
• Atraumatic surgical techniques
minimizing tissue damage, the application
of ice packs and the administration of
corticosteroids will prevent or limit
edema after implant surgery.

© Ramaiah University of Applied Sciences
20
Faculty of Dental Sciences
Flap dehiscence
• Dehiscence is opening of the surgical wound edges exposing part or
all of the implant head and/or surrounding bony tissues.
• failure to ensure closure of the flap
• presence of large edema or hematomas
• insufficient or excessive tension on the suture
• previous prosthodontic surgery or radiation therapy affecting the
vascularity of the flap

© Ramaiah University of Applied Sciences
21
Faculty of Dental Sciences
• sudden trauma by the opposing
dentition
• premature use of a removable denture
• incomplete tightening of the cover screw
• bone debris trapped under the
periosteum
© Ramaiah University of Applied Sciences
22
Faculty of Dental Sciences
Implant mobility
• This can arise where there are problems in obtaining primary
stability because of the anatomy and density of the bone, or the
implant site has been prepared without due care.
• They can often be managed by the use of 'oversized' or tapered
implants, which a number of manufacturers provide.
• Failure to secure good primary fixation is associated with increased
implant failure

© Ramaiah University of Applied Sciences
23
Faculty of Dental Sciences
Implant location
• Incorrect positioning of the
implant can lead to considerable
difficulties during the
restorative phase of treatment.
• It is extremely important that
implant locations are planned
with the prosthodontist prior to
surgery.

© Ramaiah University of Applied Sciences
24
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
25
Faculty of Dental Sciences
• Minimum distance between an implant
and a tooth should be 1.5 to 2 mm.
• Lateral biologic width around an
implant is around 1.3 mm.
• Violation of this width results in bone
loss on the implant and adjacent
structures.
• Minimum distance between 2 implants
should be 3 mm to maintain
interproximal bone height.

© Ramaiah University of Applied Sciences
26
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
27
Faculty of Dental Sciences
Problems placing cover screw
• These usually arise as a result of contamination of
the linking recess in the implant body,
misalignment of the screw or damage to the
screw threads in the implant body.
• Where necessary, the internal thread in the
implant body may have to be redefined with the
tap provided by the manufacturer, although this is
a rare occurrence

© Ramaiah University of Applied Sciences
28
Faculty of Dental Sciences
Postoperative pain
• This is an uncommon complaint
• Where it occurs immediately after implant placement, nerve involvement, inflammation and thermal trauma should all be considered.
• Pain arising later is often related to periimplant infection, or excessive pressure from the temporary prosthesis, where one is used.
• Pain immediately following implant placement can usually be
managed with mild analgesics; however, if it persists then further
investigations are required.

© Ramaiah University of Applied Sciences
29
Faculty of Dental Sciences
Paraesthesia
• This arises due to trauma to one of the nerves in the region of the
implant site.
• It usually subsides where direct mechanical damage to the
neurovascular bundle has not occurred.
• It is best avoided by careful preoperative assessment and surgery.

© Ramaiah University of Applied Sciences
30
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
31
Faculty of Dental Sciences
Infection
• Infection following surgery is unusual provided that a careful sterile
technique has been used.
• There is evidence that the use of prophylactic antibiotics can reduce
both this problem and the incidence of early implant failure.
• Where infection occurs it should be managed symptomatically.

© Ramaiah University of Applied Sciences
32
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
33
Faculty of Dental Sciences
Exposure following placement
• It is most likely to occur as a result of poor design of
the surgical flap, tension in the flap, or excessive
pressure from a temporary prosthesis or its
premature insertion.
• Where it arises the patient should be instructed to
clean thoroughly around the area, and if a denture is
being used, then this should be eased to relieve any
excessive pressure.

© Ramaiah University of Applied Sciences
34
Faculty of Dental Sciences
STAGE-TWO SURGERY
Failure to integrate
• This is usually noted as a loose implant and is more likely to occur
where factors predisposing to implant failure are present.
• Since integration is very unlikely to be established around a clinically
loose implant at this stage, management requires its removal.
• An assessment must then be made of the implications, and
consideration given to either replacement of the implant, after a
healing period, insertion of an implant in an adjacent site, or
modification of the treatment plan using a smaller number of
fixtures.

© Ramaiah University of Applied Sciences
35
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
36
Faculty of Dental Sciences
• Where the potential exists for increased implant failure, some
clinicians advocate the initial insertion of a generous number of
implants so that the original treatment plan can proceed, even if
some do not become integrated.
• This requires adequate space for implant insertion and resources to
pay for the additional costs.
• In this technique it is common, where failures do not occur, for some
of the implants to remain buried.
• These are known colloquially as 'sleepers'.

© Ramaiah University of Applied Sciences
37
Faculty of Dental Sciences
• Lack of osseointegration is diagnosed at phase II surgery or
restoration when the implant is loaded.
• The main causes for lack of osseointegration include
1. reduced healing capacity,
2. occlusal loading during osseointegration,
3. failure to follow the planned protocol,
4. technical errors during surgery (such as accidental contamination
of the implant surface),
5. bone overheating during implant site preparation.

© Ramaiah University of Applied Sciences
38
Faculty of Dental Sciences
• Clinically, lack of osseointegration is diagnosed when the implant has
loosened and a muffled sound is heard upon percussion.
• Radiographic evidence consists of a small radiolucent margin around
the implant indicating that there is no direct contact between the
bone and the implant.
• Treatment will require removal of the loose implant and accurate
debridement of the area involved so that a new implant may be
inserted after healing has taken place

© Ramaiah University of Applied Sciences
39
Faculty of Dental Sciences
Problems placing abutment
• These frequently arise due to damage to the
internal linking features of the implant body
during implant placement, particularly if this is a
screw, or misalignment of the abutment,
producing a crossed thread.
• Contamination of the internal features of the
implant, typically by bone chips, can also cause
the problem.

© Ramaiah University of Applied Sciences
40
Faculty of Dental Sciences
Bony defects
• A horizontal or vertical bony defect around an implant is a
complication that may be observed on assessing the bone-implant
interface at the time of phase II surgery.
• The causes that may lead to bone defects are
1. direct trauma to the bone or an insult to the periosteum reducing
vascularity,
2. decreased bone density,
3. implant placement into fresh extraction sockets,

© Ramaiah University of Applied Sciences
41
Faculty of Dental Sciences
4) wrong inclination of the implant
5) excessive torque during insertion
6) the presence of a bone dehiscence not treated at phase I surgery
7) an extremely thin alveolar crest,
8) wound dehiscence during healing
9) perforation of the mucoperiosteum
10) postoperative infection
11) excessive loading by the temporary prosthesis

© Ramaiah University of Applied Sciences
42
Faculty of Dental Sciences
• In the presence of: – a vertical defect of less
than 2 mm, horizontal osteoplasty can be
performed to reduce the defect without
compromising the restorations or the cosmetic
result;
• – a vertical defect of more than 2 mm involving
less than half of the implant, autologous bone
taken from an intraoral site may be grafted.

© Ramaiah University of Applied Sciences
43
Faculty of Dental Sciences
When the bone loss is greater than
25% of the circumference of the
implant, grafting may be combined
with a membrane.

© Ramaiah University of Applied Sciences
44
Faculty of Dental Sciences
Pain
• Pain at the time of second-stage surgery can arise prior to, during or
following the placement of the abutment.
• Pain prior to placement is indicative of infection, poor integration or
mechanical problems related to the temporary prosthesis.
• Where infection is present, this must be resolved prior to placement
of the abutment.

© Ramaiah University of Applied Sciences
45
Faculty of Dental Sciences
• Pain during second-stage surgery is usually indicative of failure to
achieve adequate local anaesthesia.
• Where it occurs immediately after implant abutment placement, it is
often indicative of trapping of the oral mucosa between the
abutment and the head of the implant body, or inadequate seating
of the abutment due to misalignment or trapping of adjacent bone.

© Ramaiah University of Applied Sciences
46
Faculty of Dental Sciences
IMPLANT-RELATED PROBLEMS
• Biological
• Pain
• Pain arising some time after implant placement may be associated
with mechanical overload, loss of integration, loosening of the joints
between the implant body and connecting components, infection
and mechanical failure of one of the components.

© Ramaiah University of Applied Sciences
47
Faculty of Dental Sciences
Infection
• Infection may arise as a result of poor oral hygiene or the impaction
of a foreign body.
• Calculus on the abutment can be a significant problem.
• Attention to oral hygiene, syringing of the pockets around the
abutments using a chlorhexidine solution, and cleaning of the
abutments where necessary, using plastic sealers, usually result in a
significant improvement in the condition.
• Sometimes it is necessary to remove the abutment to aid in
irrigation of the site or scaling of the abutment.

© Ramaiah University of Applied Sciences
48
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
49
Faculty of Dental Sciences
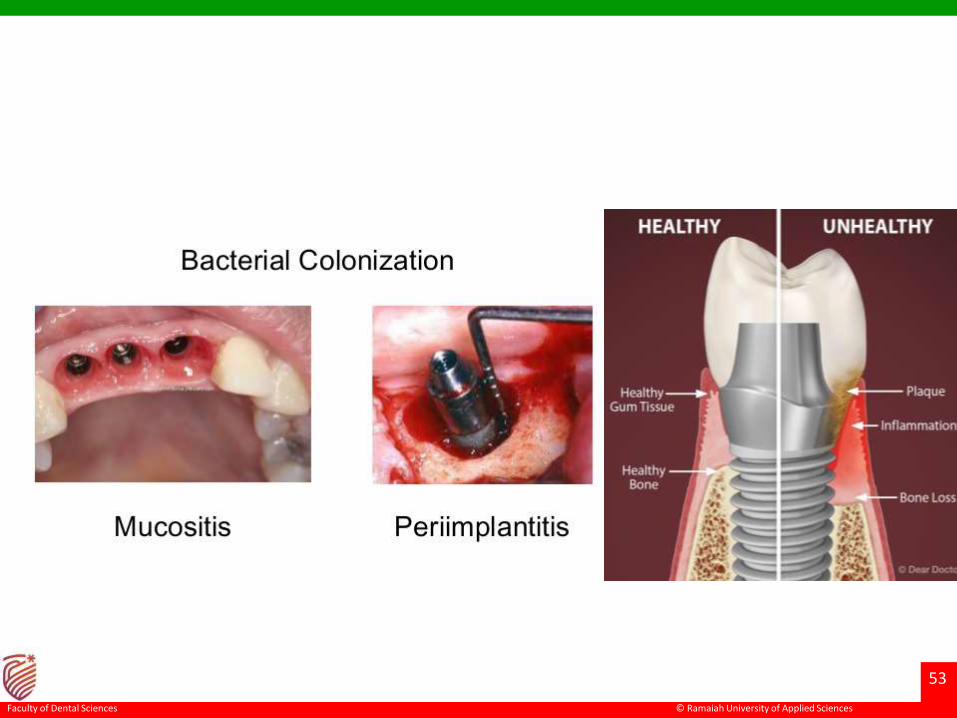
Peri-Implant mucositis
• This is a condition characterized by inflammation of the soft tissues
adjacent to the implant but excluding involvement of the peri-
implant bone.
• The characteristics of the condition include increased probing
depths, inflammation, swelling, ready bleeding on probing and
tenderness.
• It is associated with mechanical irritation and bacterial proliferation
in the peri-implant sulcus.

© Ramaiah University of Applied Sciences
50
Faculty of Dental Sciences
• The condition can also arise as a result of mechanical irritation,
particularly the presence of calculus and other foreign bodies within
the periimplant sulcus, as well as a poor fit between the abutment
and the implant body.

© Ramaiah University of Applied Sciences
51
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
52
Faculty of Dental Sciences
Peri-implantitis
• Peri-implantitis is a more severe condition, which involves loss of
bone-implant contact due to infection of the connective tissues
adjacent to the implant.
• pain around the implant
• diagnosis is by means of clinical examination, including probing of
the peri-implant sulcus.
• This will be deepened where bone loss has occurred in the crestal
region, typically all around the implant body, a finding which will
also be evident on radiographic examination.
© Ramaiah University of Applied Sciences
53
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
54
Faculty of Dental Sciences
• Predisposing factors- smoking, poorly controlled diabetes.
• Local predisposing factors include poor plaque control, bacterial
colonization of the peri-implant sulcus, mechanical irritation and
mechanical overload of the implant-bone interface.
• The link between ongoing periodontal disease and peri-implantitis is
unclear; however, it is recommended that implants should not be
used in patients with ongoing periodontal disease.
© Ramaiah University of Applied Sciences
55
Faculty of Dental Sciences
• Where the systemic factors are amenable to control then
management of these should be started as soon as the condition is
diagnosed.
• Local management, must be instigated as soon as possible to
minimize risk of the loss of the implant.
• Examination should include an assessment of masticatory loads,
plaque control, the presence of any foreign bodies around the
implant and fit of the implant components between each other.

© Ramaiah University of Applied Sciences
56
Faculty of Dental Sciences
Thread exposure
• implants have been placed too superficially
• allowance has not been made for the buccal curvature of the
alveolus
• marginal bone loss has been greater than anticipated.
• bone is excessively heated during site preparation.

© Ramaiah University of Applied Sciences
57
Faculty of Dental Sciences
Management by prevention is to be
preferred
• careful planning on a diagnostic cast
should be carried out.
• a short flange may be provided
• soft-tissue grafting to cover the defect.

© Ramaiah University of Applied Sciences
58
Faculty of Dental Sciences
Loss of integration
• there is no sufficient bone-implant contact to maintain functionality
• It may be diagnosed radiographically as well as by looseness of the
implant
• Total loss of integration is usually recognized clinically by looseness
of the implant or the ability to rotate it out of the bone.
• It is sometimes, but not always, associated with pain, which is more
likely to occur when the implant is loaded

© Ramaiah University of Applied Sciences
59
Faculty of Dental Sciences
implant failure with purulent discharge and 7.0 mmpocketing. (b) Radiograph of bone loss.

© Ramaiah University of Applied Sciences
60
Faculty of Dental Sciences
• Interim treatment will depend upon the superstructure design and
number of implants remaining.
• If there are sufficient implants, and the patient is using a fixed
superstructure, it may be possible to use the prosthesis with a
reduced number of abutments
• A final decision will depend upon the number, length and location of
the implants, the nature of the surrounding bone and the occlusal
loads.

© Ramaiah University of Applied Sciences
61
Faculty of Dental Sciences
Biomechanical
Fractures
Screws
• The principle of a screwed joint is put into tension due to its elastic
deformation and that of the clamped components, and thus compresses
the joint.
• This force is known as preload, and maintains the integrity of the joint
provided that the forces which tend to separate the components are less
than the preload.
• Forces above this will open the joint and, if they exceed the plastic limit of
the screw, cause its permanent deformation and loss of joint integrity.
• Excessive tightening of the screw will similarly cause plastic deformation of
the screw, leading to a potentially weaker joint, followed by fracture.

© Ramaiah University of Applied Sciences
62
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
63
Faculty of Dental Sciences
Screws may fracture for many reasons:
• Overtightening.
• Poorly aligned components.
• Overload.
• Fatigue failure.

© Ramaiah University of Applied Sciences
64
Faculty of Dental Sciences
Management
• The first action must be to remove the superstructure and identify
the scope of the damage.
• Following this, the fractured screw should be removed and its
housing assessed for damage.

© Ramaiah University of Applied Sciences
65
Faculty of Dental Sciences

© Ramaiah University of Applied Sciences
66
Faculty of Dental Sciences
Implant body
• Fracture of the implant body is very unusual
and almost invariably occurs as a result of
high occlusal loads or external forces, as for
example in a road traffic accident.
• The only available options in these
circumstances are either to remove the
implant body or, where the remaining
components are deep within the tissues, to
leave it buried.

© Ramaiah University of Applied Sciences
67
Faculty of Dental Sciences
PROSTHESIS PROBLEMS
Prosthesis fracture
• loss of a porcelain or acrylic resin facing, or
fracture of the metal substructure itself.
• framework is insufficiently rigid or so large
that it flexes in function to such an extent
that the porcelain/metal interface fails.
• acrylic resin facing, although this material
has a much lower modulus of elasticity
than porcelain and is therefore unlikely to
fracture as a result of substructure flexure.

© Ramaiah University of Applied Sciences
68
Faculty of Dental Sciences
• Fracture of fixed and removable prostheses may be caused by:
1. excessive loads
2. fatigue failure
3. substructure flexure
4. poor bonding between the tooth and framework or base
5. inadequate design or construction
6. Bruxism

© Ramaiah University of Applied Sciences
69
Faculty of Dental Sciences
Excessive loads
• These can arise from occlusal schemes that place high loads on
individual teeth, for example canine guidance.
• They are also associated with tooth clenching and grinding habits,
and are managed by modified design of the occlusion and
strengthening of the teeth or their occlusal or palatal coverage with
metal where they are made of porcelain or a polymer.
© Ramaiah University of Applied Sciences
70
Faculty of Dental Sciences
• Fatigue failure This by definition occurs after extended use,
especially where loads are unduly high, and is best avoided by
designs that minimize the loads on individual teeth.
• Substructure flexure This reflects inadequate design or failure to
recognize the patient who is likely to use high occlusal loads. It
results in high shear stresses at the interface between the tooth and
the substructure, which is therefore more likely to fail.

© Ramaiah University of Applied Sciences
71
Faculty of Dental Sciences
• Bond failure Poor bonding between the tooth and the framework or
base results from inadequate construction, whether it be the
bonding of porcelain to an alloy or a polymeric tooth to the
underlying acrylic resin.
• As with other problems tooth fracture is best managed by
avoidance.
• Where this is not practicable then repairs are usually possible,
especially with polymeric teeth.
• The replacement of porcelain is much more expensive as it requires
often extensive refiring.

© Ramaiah University of Applied Sciences
72
Faculty of Dental Sciences
Functional problems
Appearance
• Appearance problems related to fixed-implant superstructures are
more common in the upper jaw.
• They are related to the difficulties of placing teeth in the positions of
their natural predecessors
• Where it is desired for the crowns to have the appearance of arising
from the edentulous ridge, the disparity in the preferred positions of
the crown and implant body may be difficult or impossible to
disguise effectively, resulting in an unnatural appearance.
• Bone-grafting procedures can be used to modify the ridge contour

© Ramaiah University of Applied Sciences
73
Faculty of Dental Sciences
• 'black triangle' appearance.
• Soft tissues can be the contoured at the
second stage of surgery; however, it is
difficult to achieve a satisfactory result if
there is an excessive gap between the
implants.
• Problems relating to tooth mould, shade
and contour

© Ramaiah University of Applied Sciences
74
Faculty of Dental Sciences
Speech
• Speech problems can arise as a result of
changes in the labiopalatal positioning of
the anterior teeth and the level of the
occlusal plane.
• Many of these problems are usually quite
quickly overcome by adaptation
• gap between its framework and the
underlying mucosa- escape of air or
saliva, which can influence the speech

© Ramaiah University of Applied Sciences
75
Faculty of Dental Sciences
• Some patients learn to adapt to this situation, while others need to
make use of a removable component to obturate the defect.
• This may consist of an elastomeric bung, which is placed palatally, or
a removable acrylic labial flange.
• It is important when planning implant treatment to inform the
patient in advance if it is thought that speech problems are likely to
occur.

© Ramaiah University of Applied Sciences
76
Faculty of Dental Sciences
Mastication
• Masticatory problems when using implant-stabilized bridges are
unusual
• Usually due to the occlusal scheme and nature of the opposing
dentition.
• These can be managed using standard prosthodontic techniques.
• Cheek biting sometimes occurs due to the failure to place maxillary
teeth sufficiently buccally
• Patients must be warned of such potential problems when planning
treatment.

© Ramaiah University of Applied Sciences
77
Faculty of Dental Sciences
Conclusion
• Implant therapy has become common practice and will probably
gain in popularity during the next several years.
• This implies that dental professionals will have to deal more with
implant failure and related complications.
• When an implant fails, a tailor made treatment plan should be
provided to each patient according to all relevant variables.
• Patients should be informed regarding all possible treatment
modalities after implant failure and give their consent to the most
appropriate treatment option for them.

© Ramaiah University of Applied Sciences
78
Faculty of Dental Sciences
References
• Misch : Contemporary implant dentistry Atlas of implant dentistry,
• Why do dental implants fail: part I : Askary et al ID 1999 vol8 no2 173-183
• Why do dental implants fail: part II : Askary et al Id 1999 vol 3 : 265-275
• A.S.Sclar; Soft tissue & esthetic considerations in implant dentistry.
• Myron Nevins; Implant therapy.
• Torosian J, Rosenberg ES. The failing and failed implant: a clinical, microbiologic, and treatment review.
• J Esthet Dent. 1993. Failures in implant dentistry.W. Chee and S. Jivraj. British Dental Journal 202, 123 - 129 (2007)
• Yoav Grossmann. Prosthetic treatment for severely misaligned implants: A clinical report. J Prosthet Dent 2002;88:259-6.
• Goodacre C J, Bernal G, Rungcharassaeng K, Kan J Y. Clinical complications with implants and implant prostheses. J ProsthetDent 2003; 90: 121–132.
• Effect of implant size and shape on implant success rates: A Literature review JPD 2005;94:377-81