Embed Size (px)
Citation preview

COMPLICATIONS OF LAPAROSCOPIC
CHOLECYSTECTOMY
ByByDR. SEFEEN SAFE ATTYADR. SEFEEN SAFE ATTYASURGERY DEPARTMENT SURGERY DEPARTMENT
SOHAG TEACHING HOSPITALSOHAG TEACHING HOSPITAL

Laparoscopy is an art to do Laparoscopy is an art to do great things throughgreat things through
small openingssmall openings

The operative removal of the gallbladder is a standard
and one of the most often performed procedures in general surgical departments.
The operation is indicated in - cases of gallbladder stones creating symptoms - cases of acute infection of the gallbladder with or
without stones - cases of adenomatous structures in the gallbladder that may develop malignity

Nowadays more than 90% of the elective cholecystectomies are performed
laparoscopically.
Although laparoscopic cholecystectomy has become the gold standard of
treatment it does not preclude complications, whether major or minor.

Complications of stones within the gallbladder1- Biliary colic. Intermittent epigastric pain may radiate to the right and may be
induced by fatty food. 2. Acute cholecystitis. severe pain in the right upper quadrant which is constant.
pyrexia and tachycardia, and leucocytosis .3. Empyema of the gallbladder. Very severe acute cholecystitis
4- Emphysematous cholecystitis. Severe infections with anaerobic gas-forming organisms may occur in diabetics. Gas is seen in the wall of the gallbladder on a
plain radiograph.
5- Mirizzi syndrome. A gallstone impacted in Hartmann’s pouch, may result in obstructive jaundice by impinging on the common bile duct.
6- Mucocele. Impaction of a calculus in the neck of the gallbladder resulting in stasis and continued formation of mucus results in a mucocele.
7- Carcinoma. There is a small risk of malignancy in the gallbladder mucosa in association with gallstones. It is five times more common in females than
males.

Complications of stones outside the gallbladder1. Pancreatitis. Acute and chronic pancreatitis may result from the passage of
gallstones through the common bile duct. Approximately 50% of pancreatitis is gallstone-related.2. Biliary stricture. Chronic calculous inflammation may result in a benign bile duct stricture. This may cause obstructive jaundice and predispose to ascending
cholangitis, 3. Obstructive jaundice. This results from impaction of a calculus in the distal common bile duct. Multiple calculi may be present. 4. Ascending cholangitis. This is a severe infection, usually complicating benign obstruction of the biliary tree. The infecting organisms are usually Gram negative bacilli. Endotoxic shock may result. A diagnosis may be made clinically in the presence of Charcot’s triad: fever with rigors, jaundice, and an enlarged tender liver. It requires prompt diagnosis, i.v. fluids, antibiotics directed toward coliforms, and urgent relief from the obstruction. ERCP and sphincterotomy with stone extraction or temporary stenting is urgently undertaken. Open surgery is hazardous in acute
cholangitis.
5. Gallstone ileus. A large solitaire may erode into the duodenum and impact at the narrowest point of the small bowel, typically two feet proximal to the ileocaecal valve This presents as a small bowel obstruction.

Eric muhe performed Eric muhe performed the first the first laparoscopic laparoscopic cholecystectomy in cholecystectomy in germany in 1985 germany in 1985

BENEFITS OF lap.choleBENEFITS OF lap.chole..
1-Reduced traumatic insult to the patient 1-Reduced traumatic insult to the patient by the surgical intervention by the surgical intervention
2- absence of exposure or drying of 2- absence of exposure or drying of intestinal loops and lack of intestinal loops and lack of contamination of the intra-abdominal contamination of the intra-abdominal contents with operative room air contents with operative room air
3- The inevitable non-specific depression 3- The inevitable non-specific depression of the immune system after surgery has of the immune system after surgery has been shown to be less intense . been shown to be less intense .

4- Significant reduction in the wound 4- Significant reduction in the wound - related complications [wound - related complications [wound infection and dehiscence]infection and dehiscence]
5-Sigificant reduction of internal 5-Sigificant reduction of internal adhesion formationadhesion formation
6- Reduced hospital cost as a result 6- Reduced hospital cost as a result of the reduced hospital stay and of the reduced hospital stay and early return to employmentearly return to employment

Steps of L . C. Patient position and equipmentsPatient position and equipments Creation of pneumoperitoniumCreation of pneumoperitonium Trocar placementsTrocar placements Dissection of cystic duct and arteryDissection of cystic duct and artery Removal of the gall bladderRemoval of the gall bladder Extraction of the gall bladderExtraction of the gall bladder Chick for haemostasis Chick for haemostasis Closure of port sitesClosure of port sites

Patient position and Patient position and equipmentsequipments
the patient is stretched out with the left arm extended
The monitor system is on the right patient side.
The surgeon and his camera assistant who is basically the "eye" of the surgeon should stand on the left patient side in order to have the same viewing direction.
The second assistant stands on the right patient side in order to fulfil his role which is mainly static, by lifting the gallbladder up from underneath the liver to expose the infundibulum




Creation of Creation of pneumoperitoniumpneumoperitonium
CLOSED PNEUMOPERITONIUM CLOSED PNEUMOPERITONIUM
[veress needle][veress needle]
OPEN PNEUMOPERITONIUM OPEN PNEUMOPERITONIUM
[hasson’s technique][hasson’s technique]

CLOSED PNEUMOPERITONIUMCLOSED PNEUMOPERITONIUM
This is produced by the insertion of a veress This is produced by the insertion of a veress needle through the immediate subumbilical needle through the immediate subumbilical area in a previously unopened abdomen area in a previously unopened abdomen
It must be remembered that the distance It must be remembered that the distance between the anterior abdominal wall and the between the anterior abdominal wall and the aorta and its bifurcation average only 2 cmaorta and its bifurcation average only 2 cm
The most popular measure used to ensure The most popular measure used to ensure that the veress needle is lying in free that the veress needle is lying in free intraperitoneal space is the saline drop test intraperitoneal space is the saline drop test


Insertion of Veress Insertion of Veress needleneedle

Saline drop testSaline drop test

IN 1938, Veress developed a specially designed spring-loaded needle. Interestingly, Veress did not promote the use of his Veress needle for laparoscopy purposes. He used veress needle for the induction of pneumothorax.
Veress needle consists of an outer cannula with a beveled needle
point for cutting through tissues. Inside the cannula of verses needle is an inner stylet, stylet
is loaded with a spring that spring forward in response to the
sudden decrease in pressure encountered upon crossing the
abdominalwall and entering the peritoneal cavity.


Insertion of the first Insertion of the first trocartrocar

It is good practice once the It is good practice once the telescope is inserted to scan the telescope is inserted to scan the abdomen to establish that no injury abdomen to establish that no injury has been sustained during the has been sustained during the creation of pneumoperitonium and creation of pneumoperitonium and insertion of the optical port insertion of the optical port

Insertion of 2nd trocar underInsertion of 2nd trocar underdirect visiondirect vision

OPEN PNEUMOPERITONIUM OPEN PNEUMOPERITONIUM
The technique entails a small The technique entails a small subumbilical incision , the linea subumbilical incision , the linea alba is then divided and the alba is then divided and the peritonium opened , a sealing peritonium opened , a sealing optical cannula of the hasson type optical cannula of the hasson type is then inserted and held in place is then inserted and held in place by sutures by sutures
Insuflation of the peritoneal cavity Insuflation of the peritoneal cavity is then commenced through the is then commenced through the side port of the hasson cannulaside port of the hasson cannula

In 1978, Hasson introduced an alternative method for the creation of pneumoperitonium
He proposed a blunt minilaparotomy which permits direct visualization of trocar entrance
into the peritoneal cavity. This cannula is held in place by the use of stay sutures passed through the facial edges
and attached to the body of the cannula.

Placement of a Hasson trocar. Placement of a Hasson trocar. Two fascial sutures stabilize Two fascial sutures stabilize the abdominal wall, and the trocar is inserted under direct the abdominal wall, and the trocar is inserted under direct visionvision


Trocar placementsTrocar placements

Dissection of cystic duct and Dissection of cystic duct and arteryartery
Atraumatic grasping forcepses are placed through the right-sided ports to elevate the gallbladder
in both cephalad and rightward directions to expose the triangle of Clot.
The peritoneum overlying the base of the gallbladder and the triangle of Calot is incised,
exposing the cystic duct and cystic artery. The cystic duct and artery are doubly
clipped and divided.


Removal of the gall bladderRemoval of the gall bladder After division of the cystic duct and cystic artery the gallbladder is removed from underneath the liver bed. At this point diathermy can be of great assistance since small vessels in the liver bed can easily be coagulated together with the separation of the
connective tissue between the gallbladder and liver bed.
Nevertheless the risk of an iatrogenic gallbladder perforation remains therefore the preparation must
remain close to the gallbladder, but not so close that the gallbladder tears.

Extraction of the gall Extraction of the gall bladderbladder When the operation reaches the point of extraction the gallbladder from the abdominal cavity, it is
recommended that a plastic recovery bag be placed in the abdomen and the gallbladder put inside for removal. The organ should not removed in direct contact with
the abdominal wall since it may be contaminated by
bacteria and these bacteria may, in turn, come in contact with the abdominal wall of the trocar channel where the removal takes place causing local wound infection.

For For infected tissueinfected tissue and in and incase of case of suspected carcinomasuspected carcinoma tissue tissue
retrieval bag should be useretrieval bag should be use

After the safe removal of gallbladder, it is inspected visually and sent for histopathological
examination. a "last look into the abdomen". Any final bleedings, particular from the liver bed, must be detected and taken care of. We need to look for leaking blood vessels and also for leaking additional bile ducts that have to be closed.

drainagedrainage the need for a drainage system has to be determined. Generally speaking over the years the amount of drainages
placed in laparoscopic gallbladder surgery has decreased due to increased
awareness concerning the safety of operations and also the fact that
whilst drainage is indicated in specific instances, it should be avoided in others.
The situations where drainage is appropriate: 1- significant bleeding during the operation 2- significant bile leakage, 3- severe infection in acute cholecystitis
When drainage is indicated the passive drainage System is recommended

Closure of port sitesClosure of port sites The closure of the abdomen in laparoscopic surgery is very straightforward since the 5 mm trocar
positions simply require a skin suture or use of sterile stripes as necessary. The 10 mm trocar positions and especially the position where the gallbladder has been removed, need closure both, the peritoneum and the anterior sheath of the rectus muscle. This is mandatory to
prevent trocar hernia..

COMPLICATIONS OF COMPLICATIONS OF LAPAROSCOPIC LAPAROSCOPIC
CHOLECYSTECTOMYCHOLECYSTECTOMY GAS RELATED COMPLUCATIONS BILE DUCT INJURY BLOOD VESSLE INJURY GALLBLADDER PERFORATION &
LOSS OF STONES BOWEL INJURY PORT SITE INFECTION PORT SITE HERNIA

CO2 EMBOLISMCO2 EMBOLISM
Insuflation through the veress needle Insuflation through the veress needle accidentaly impaled in the uterus or accidentaly impaled in the uterus or liver liver
Through unsealed vessels in sufficiently Through unsealed vessels in sufficiently large amounts that exceed its solubility large amounts that exceed its solubility
The risk of embolism is accentuated by The risk of embolism is accentuated by the Use of the Use of argon gas beamerargon gas beamer this gas is this gas is
much less soluble much less soluble

Diagnosis of CO2 embolismDiagnosis of CO2 embolism Sudden drop in the blood pressure in Sudden drop in the blood pressure in
the absence of bleeding and in the the absence of bleeding and in the presence of a raised central venous presence of a raised central venous pressure pressure
A A crunching precordial murmurcrunching precordial murmur is is audible with the stethoscope audible with the stethoscope
ECG is diagnosticECG is diagnostic Treatment Treatment Immediate deflation of the Immediate deflation of the
pneumoperitoniumpneumoperitonium Head-down posturing of the patientHead-down posturing of the patient

Bile Duct Injuries Several description and classification systems
(such as Bisthmus class. Or Strasberg class.)
Bile duct injuries must be viewed as potentially
very severe complications bearing high morbidity,
long-term hospitalization, disease chronificationand possibly life threatening .

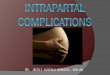
The most frequent The most frequent mechanism of injury is mechanism of injury is mistaking a major bile mistaking a major bile duct for the cystic duct duct for the cystic duct and clipping and cutting and clipping and cutting it it

Bisthmus class.
Type 1 injury: 2 cm. or more of the common Type 1 injury: 2 cm. or more of the common hepatic duct is preserved below the bifurcationhepatic duct is preserved below the bifurcation
Type 2 injury :less than 2 cm. remainsType 2 injury :less than 2 cm. remains Type 3 injury : injury reaches the bifurcation with Type 3 injury : injury reaches the bifurcation with
preservation of the continuity between the right preservation of the continuity between the right and left ductsand left ducts
Type 4 injury : involves destruction of the hepatic Type 4 injury : involves destruction of the hepatic duct confluence with separation of the right and duct confluence with separation of the right and left hepatic ductsleft hepatic ducts
Type 5 injury : involves injury of a separate Type 5 injury : involves injury of a separate inserting right sectorial duct with or without inserting right sectorial duct with or without common duct injurycommon duct injury


factors involved in the occurrence of bile factors involved in the occurrence of bile duct injuries during laparoscopic duct injuries during laparoscopic
cholecystectomycholecystectomy.. acute or chronic inflammation, obesity, anatomic variations, acute or chronic inflammation, obesity, anatomic variations,
and bleedingand bleeding. .
The bile duct injury rate is increased in patients with The bile duct injury rate is increased in patients with complications of gallstones, including acute cholecystitis, complications of gallstones, including acute cholecystitis, pancreatitis, cholangitis, and obstructive jaundicepancreatitis, cholangitis, and obstructive jaundice. .
Surgeon training and experienceSurgeon training and experience. . As surgeon experience As surgeon experience increases beyond 20 cases, the bile duct injury rate increases beyond 20 cases, the bile duct injury rate decreasesdecreases..
Recent reports have indicated that errors leading to Recent reports have indicated that errors leading to laparoscopic bile duct injuries from misperception, not laparoscopic bile duct injuries from misperception, not errors of skill, knowledge, or judgmenterrors of skill, knowledge, or judgment. . The primary cause The primary cause of error in 97% of cases was a visual perceptual illusion, of error in 97% of cases was a visual perceptual illusion, whereas only 3% of injuries were due to faults of technical whereas only 3% of injuries were due to faults of technical skill.skill.

PresentationPresentation
Patients with bile duct injuries can present Patients with bile duct injuries can present
intraoperatively, in the early postoperative intraoperatively, in the early postoperative period, or months or years after the initial injuryperiod, or months or years after the initial injury. .
About 25% of major ductal injuries are recognized About 25% of major ductal injuries are recognized intraoperatively because of bile leakage, an intraoperatively because of bile leakage, an abnormal cholangiogram, The most common abnormal cholangiogram, The most common presentation of a complete occlusion of the presentation of a complete occlusion of the common hepatic or bile ductcommon hepatic or bile duct is jaundice with or is jaundice with or without abdominal painwithout abdominal pain..
Patients may also present months or years after Patients may also present months or years after surgery with cholangitis or cirrhosis secondary to surgery with cholangitis or cirrhosis secondary to a biliary tract injurya biliary tract injury..

Diagnosis and Diagnosis and ManagementManagement
Isolated, small , partial lateral bile duct injury Isolated, small , partial lateral bile duct injury recognized at time of cholecystectomy can recognized at time of cholecystectomy can be managed with placement of a T tubebe managed with placement of a T tube. .
However, if the biliary injury is more However, if the biliary injury is more extensive, or if there is significant thermal extensive, or if there is significant thermal damage owing to cauterydamage owing to cautery--based trauma, or if based trauma, or if the injury involves more than 50% of the the injury involves more than 50% of the circumference of the bile duct wall, an endcircumference of the bile duct wall, an end--toto--side choledochojejunostomy with a Rouxside choledochojejunostomy with a Roux--enen--Y loop of jejunum should be performedY loop of jejunum should be performed. .

Similarly, major bile duct injuries, Similarly, major bile duct injuries, including transections of the common including transections of the common bile or common hepatic duct, can be bile or common hepatic duct, can be repaired if recognized at the time of repaired if recognized at the time of cholecystectomycholecystectomy. .
Isolated hepatic ducts smaller than 3 Isolated hepatic ducts smaller than 3 mm or those draining a single hepatic mm or those draining a single hepatic segment can be safely ligatedsegment can be safely ligated..
Ducts larger than 3 mm are more Ducts larger than 3 mm are more likely to drain several segments or an likely to drain several segments or an entire lobe and need to be entire lobe and need to be reimplantedreimplanted. .

Gallbladder Perforation and Loss of Stones
Due to the way the gallbladder is held and manoeuvred
during L.C. and due to its wall structure and probable
grade of infection, the risk of rupture of the gallbladder during L.C. is quantitatively high
This may lead to an increase of postoperativecomplications such as wound infections or
intraabdominalabscess formations .

Should a perforation occur, The bile liquid has to be promptly retrieved with adequate aspiration devices
It is imperative that spilled stones be completely identified and extracted
from the abdominal cavity.

Routinely performance of a blood sample including TLC, CRP and LFTs on the day after the operation.
In cases of fever or pain, an immediate ultrasound is indicated. Pain increase or complications may prompt
the need for surgical re-intervention Otherwise the patient is kept under close observation and possibly entailing a longer
hospitalization.

Biliary LeakBiliary Leak
Leaks from the cystic duct stump Leaks from the cystic duct stump unrecognized duct of Luschkaunrecognized duct of Luschka. . Bile leaks commonly present shortly after cholecystectomy Bile leaks commonly present shortly after cholecystectomy ((within 1 within 1
weekweek) ) with right upper quadrant pain, fever, chills, and with right upper quadrant pain, fever, chills, and hyperbilirubinemiahyperbilirubinemia. .
CT scan and ultrasound will confirm presence of a complex fluid CT scan and ultrasound will confirm presence of a complex fluid collection in the right upper quadrantcollection in the right upper quadrant. .
Immediate operative intervention with wide drainage is only Immediate operative intervention with wide drainage is only indicated if the patient is in septic shockindicated if the patient is in septic shock. . Attempts at early repair Attempts at early repair are dangerous because of the inflammatory response incited by the are dangerous because of the inflammatory response incited by the bile leakbile leak..
Percutaneous drainage of intraPercutaneous drainage of intra--abdominal fluid collections followed abdominal fluid collections followed by an endoscopic biliary stenting resolves most leaks without need by an endoscopic biliary stenting resolves most leaks without need for operative interventionfor operative intervention..
If bile leaks fail to resolve after 6 weeks, further imaging with MRC If bile leaks fail to resolve after 6 weeks, further imaging with MRC and endoscopic imaging may be necessary to rule out a common and endoscopic imaging may be necessary to rule out a common bile duct injurybile duct injury. . When the acute inflammation has resolved 6 to 8 When the acute inflammation has resolved 6 to 8 weeks later, operative repair is performedweeks later, operative repair is performed..

Retained Biliary StonesRetained Biliary Stones
Retained stones following cholecystectomy present soon Retained stones following cholecystectomy present soon after after ((<4 weeks<4 weeks) ) surgery and are best treated surgery and are best treated endoscopicallyendoscopically. .
If stones are found shortly after the cholecystectomy, they If stones are found shortly after the cholecystectomy, they are classified asare classified as retainedretained; ; those diagnosed months or years those diagnosed months or years later are termedlater are termed recurrentrecurrent
. . Patients will present most commonly shortly after Patients will present most commonly shortly after cholecystectomy with sharp, intense right upper quadrant cholecystectomy with sharp, intense right upper quadrant pain and jaundicepain and jaundice. . Bilirubin and alkaline phosphatase Bilirubin and alkaline phosphatase elevation should prompt endoscopic clearance of biliary elevation should prompt endoscopic clearance of biliary stonesstones. . Recurrent stones may be multiple and largeRecurrent stones may be multiple and large..
A generous endoscopic sphincterotomy will allow stone A generous endoscopic sphincterotomy will allow stone retrieval as well as spontaneous passage of retained and retrieval as well as spontaneous passage of retained and recurrent stonesrecurrent stones..

BlOOd Vessel Injuries
Cystic arteryCystic artery Right hepatic arteryRight hepatic artery Portal vein Portal vein Inferior epigastric vesselsInferior epigastric vessels

In order to clearly identify the cystic artery, without injuring larger branches, we need to identify the vessel where
it enters the wall of the gallbladder and divides itself.
so in preparing the cystic artery we need
to stay close to the gallbladder.

In the event of bleeding a "blind" clipping or the "blind" use of diathermy is not the method of choice though it sometimes appears to be the fastest way to stop bleeding.
Such methods should only be performed when confident that we are dealing with a second branch of the cystic artery and not with a more proximal
vessel.
Precarious clip placement or the extensive use of diathermy on such a larger supply vessel may result
in a reduction of the liver blood supply especially when dealing with a common hepatic artery.

Though it seems that isolated injuries of the righthepatic artery usually remain clinically insignificant inotherwise healthy patients,
Additional risk factors such as hypoxemia, cholangitis,
sepsis, liver cirrhosis or abnormally reduced portal venous blood flow,
All create a high risk for the development ofischemic liver necrosis,abscess formations in the liver and further
complicationssuch as destructive cholangitis and secondarybiliary cirrhosis.

Trocar channel bleedings may stop during trocar placement which places a certain pressure on
the bleeding vessel, but may reoccur at the end of the procedure due to removal of the trocar.
It is important to identify such events which can be effectively dealt with via
electrocoagulation or suture,

Postoperative bleeding complications involve cases of cystic artery damage, prolonged haemorrhage
from the gallbladder bed , parenchymal liver injuries and
also trocar channel bleedings.
Causes can be attributed to insufficient clipping, slipped clips, inadequate diathermy or to the fact
that the decrease of intraabdominal pressure at the end
of the procedurecan lead to a re-opening of compressed vesselsand to new bleeding as a consequence.

diathermy for electrocoagulation or the harmonic
scalpel should be used only under clear anatomic circumstances.
That means for example it is highly dangerous
to begin the laparoscopic cholecystectomy mainly with a preparation using diathermy-
a common practise in several hospitals.























THANK YOU