Embed Size (px)
Citation preview
Competition vs. Collaboration: Physicians, Nurse Practitioners
and Physician Assistants
Tyree M.S. Winters, DONCH Clinical Lead Physician
Primary Care Obesity NetworkNationwide Children’s Hospital/Ohio State University Wexner
Medical Center
Disclosure Statement: I developed this lecture without influence (financial/intellectual) from outside parties. I do not have any relevant financial relationships with any commercial interests
Objectives
• Discuss the current practice guidelines for nurse practitioners and physician assistants
• Review current research outcomes focusing on nurse practitioners and physician assistants utilized as independent providers, and how it can impact access to health care
• Discuss the current political climate surrounding the relationship between physicians and nurse practitioners/physician assistants in the future of the nation's health care delivery system
The brain is an amazing organ. It starts working the moment you get up in the morning and doesn’t stop until you get into work
-David Frost
Nurse Practitioners (NP)
• There are more than 205,000 nurse practitioners (NPs) licensed in the U.S.
• 95.1% of NPs have graduate degrees
• 96.8% of NPs maintain national certification
• 86.5% of NPs are prepared in primary care
• NPs hold prescriptive privilege in all 50 states and D.C., with controlled substances in 49
• 42 states require a NP to hold a master’s degrees in nursing and retain national certification in order to practice
• In 2011, the mean, full-time base salary was $91,310, with average full-time NP total income at $98,760
• The majority (69.5%) of NPs see 3 or more patients per hour
AANP 2015
Change in State Regulation for NPs: 2000-2010• Over the decade, fewer states required physician
involvement in treatment and diagnosis
• 32 states in 2001 to 27 states in 2010 – supervision (8 to 4)– collaboration (3 to 29)– direction (1 across the decade)– delegation (4 to 3)
E.A. Gadbois, et. al. Trends in state regulation of nurse practitioners and physician assistants, 2001 to 2010. Medical Care Research and Review: MCRR 2015, 72 (2): 200-19
• States that increased training requirement (MSN or above)– Arkansas, Colorado, New Hampshire and Tennessee
• States who allowed NPs autonomous practice in treatment and prescriptive authority – Arizona, Colorado, Hawaii, Idaho, Michigan, Rhode Island,
Washington and Wyoming
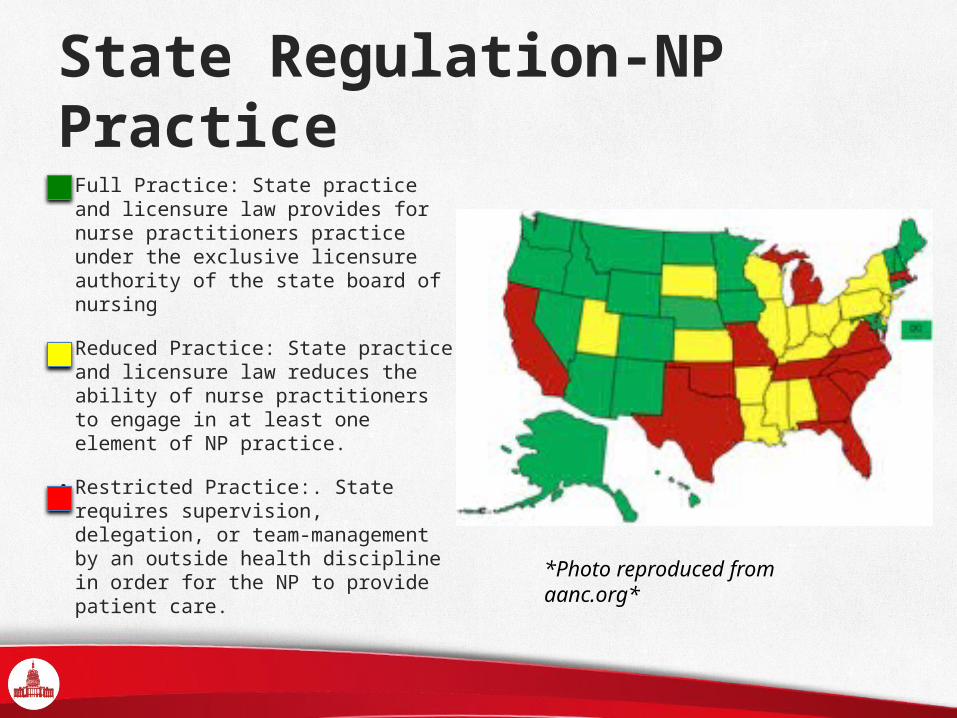
State Regulation-NP Practice • Full Practice: State practice and
licensure law provides for nurse practitioners practice under the exclusive licensure authority of the state board of nursing
• Reduced Practice: State practice and licensure law reduces the ability of nurse practitioners to engage in at least one element of NP practice.
• Restricted Practice:. State requires supervision, delegation, or team-management by an outside health discipline in order for the NP to provide patient care.
*Photo reproduced from aanc.org*
Physician Assistant (PA)
• Approximately 101,977 certified PAs as of December 2014
• Certified PAs practice medicine in all 50 states and D.C.
• The median age of certified PAs was 38 in 2014.
• Today 66.6% of all certified PAs are female.
• By 2020, all PA programs must confer a graduate degree to be accredited by the Accreditation Review Commission on Education for the Physician Assistant
• The average salary of certified PAs was $98,387 with the highest paid to those working in dermatology, emergency medicine, critical care medicine and surgery subspecialties.
• Full-time (40+ hours per week) PAs see an average of 76 patients per week (1.9 patients/hour) in their principal clinical position
NCCPA 2015
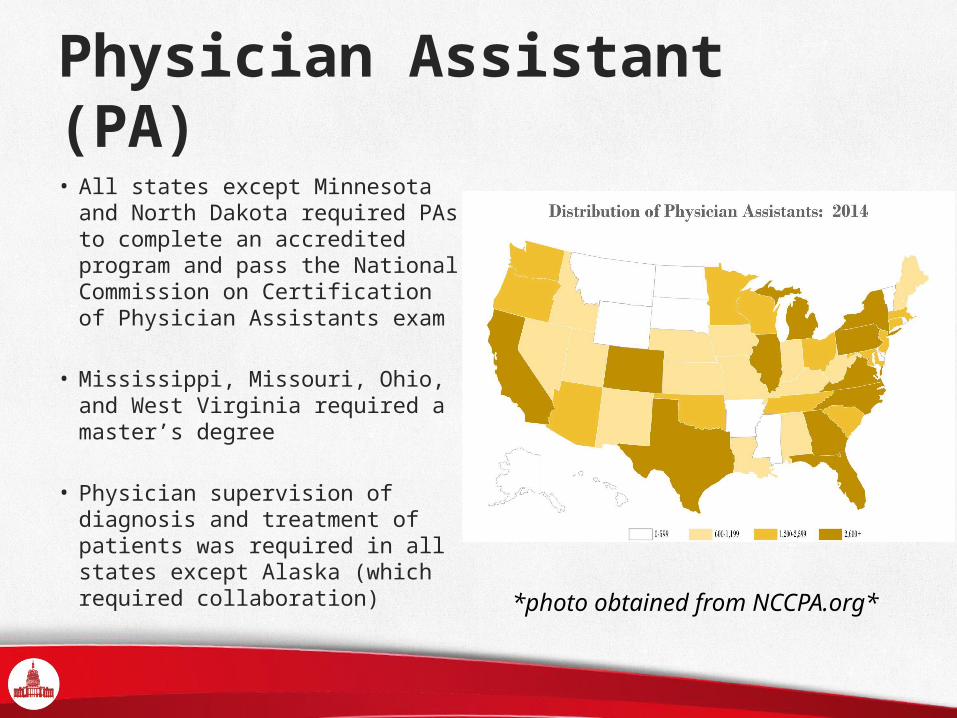
Physician Assistant (PA)• All states except Minnesota and
North Dakota required PAs to complete an accredited program and pass the National Commission on Certification of Physician Assistants exam
• Mississippi, Missouri, Ohio, and West Virginia required a master’s degree
• Physician supervision of diagnosis and treatment of patients was required in all states except Alaska (which required collaboration)
*photo obtained from NCCPA.org*
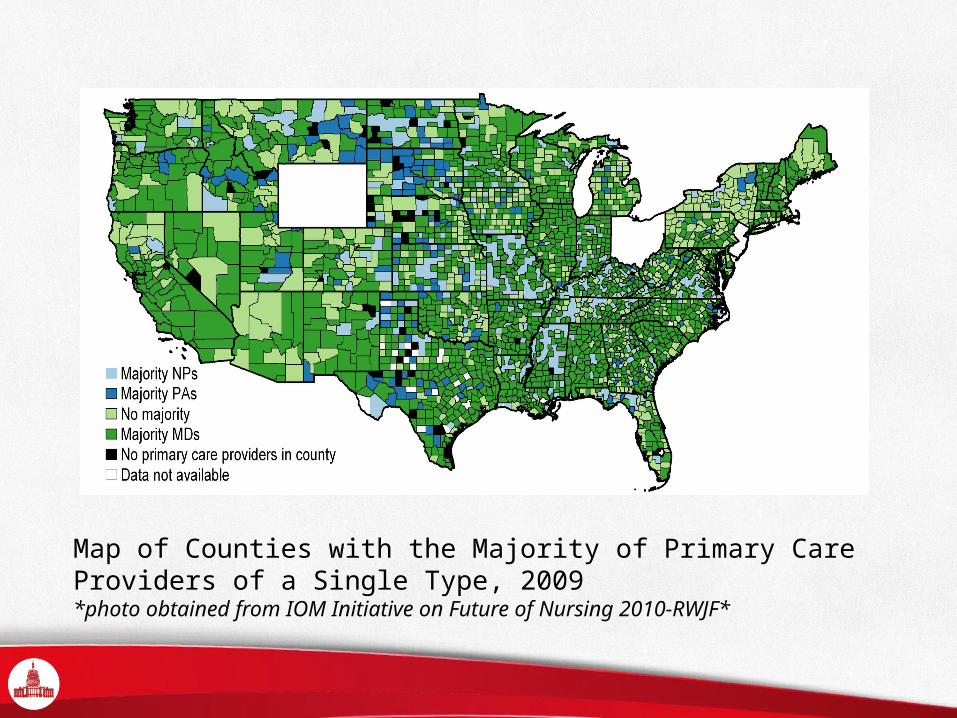
Map of Counties with the Majority of Primary Care Providers of a Single Type, 2009*photo obtained from IOM Initiative on Future of Nursing 2010-RWJF*

Institute of Medicine: Future of Nursing Recommendations
• Remove scope-of-practice barriers– Allow full independent practice according to level of
training • Implement nurse residency programs– encourage state boards of nursing and other national
agencies to support the training of nurses to complete a “transition-to-practice” program (nurse residency)
• Double the number of nurses with doctorate degrees by 2020
IOM 2010
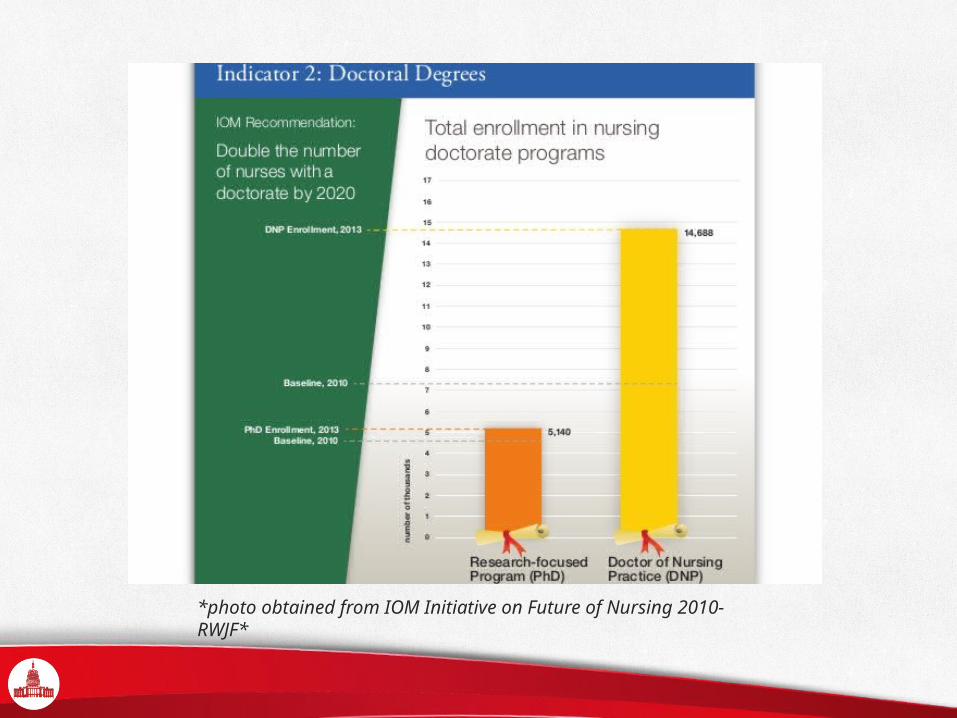
*photo obtained from IOM Initiative on Future of Nursing 2010-RWJF*
Support for NP/PA Independent Practice
• Several studies have shown that APRNs produce outcomes comparable to those of physicians and that the care they provide encompasses 80 to 90 percent of the services provided by physicians (Lenz et al., 2004)
• NPs and PAs have been documented to deliver care for a large fraction of diagnoses at equivalent quality and lower cost than physicians (Eiber et al., 2009)
• Study conducted by Massachusetts Division of Health Care Finance and Policy on cost savings for care provided by NPs and PAs in retail clinics (Eiber et al., 2009)
• Compared cost of treatment for only 6 simple acute conditions (cough, throat symptoms, fever, earache, skin rash, and nasal congestions) and preventative wellness visits
• Demonstrated potential savings in Massachusetts over a ten-year period ranged from a lower bound of $4.2 billion to a higher bound of $8.4 billion for treatment of these six diagnoses
Malpractice
• According to 2010 Pearson Report
– no increase in claims registered in the Healthcare Integrity and Protection Data Bank in states where APRNs have full authority to practice and prescribe independently
– Overall ration of claims against NPs is 1 for every 166 NPs in the nation compared with 1 for every 4 physicians
Income Variation
• One study using Current Population Survey data found that in states where NPs had higher levels of autonomy, physicians and NPs earned less, while PAs earned more (Safriet, B.J., 2011)
• Greater NP authority led to increased NP income, reduces physician income, and had a differential impact on PA income. In contrast, increased PA authority had little effect on PA income but was associated with reduced NP and increased physician income. (Safriet, B.J., 2011)
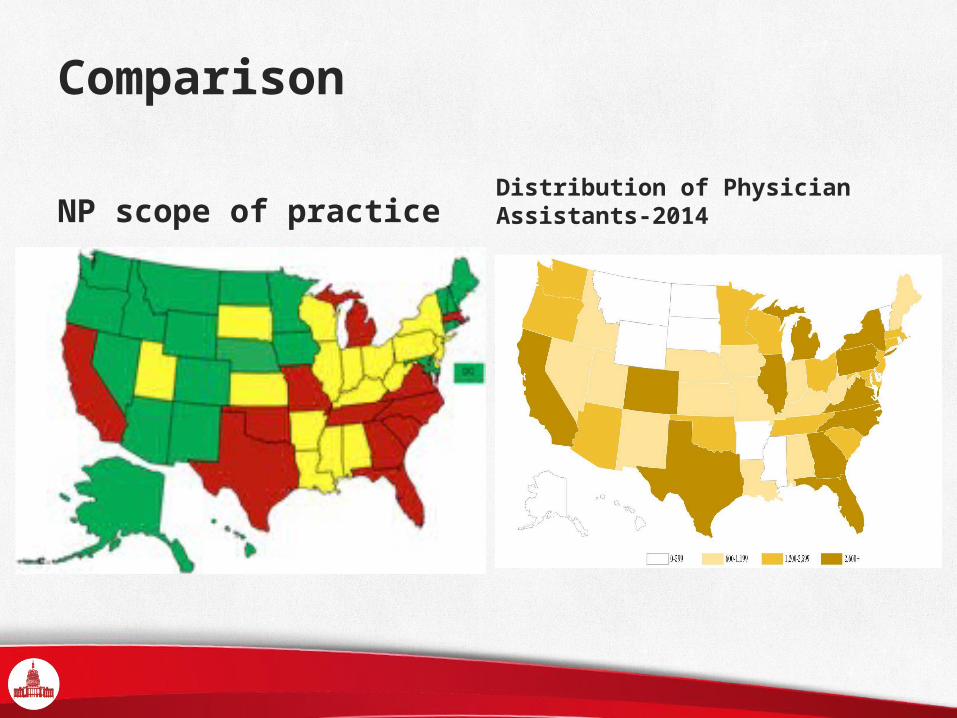
Comparison
NP scope of practiceDistribution of Physician Assistants-2014
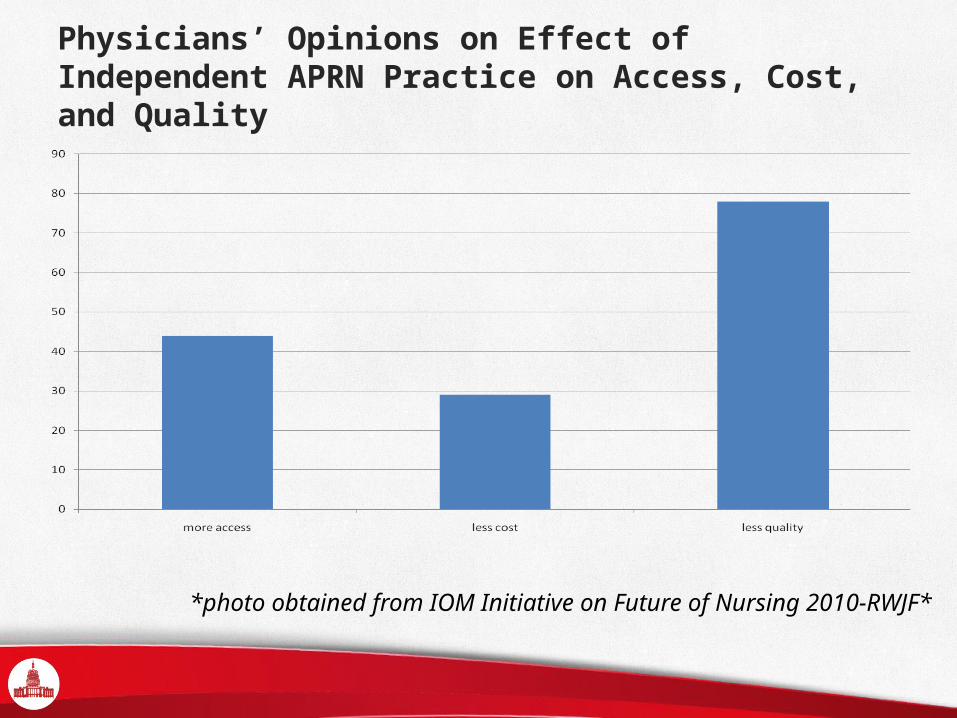
Physicians’ Opinions on Effect of Independent APRN Practice on Access, Cost, and Quality
*photo obtained from IOM Initiative on Future of Nursing 2010-RWJF*
Physicians’ Group Position Statements: Nurse Practitioner• Several national physician organizations condemn
NPs operating as independent health practitioners and recommend that NPs should only operate under the supervision of a practicing, licensed physician– American Academy of Family Physicians (AAFP)– American Academy of Pediatricians (AAP)– American Medical Association (AMA)– American Osteopathic Association (AOA)
Physicians’ Group Position Statements: Physician Assistant • AAFP and AAPA believe that family physicians and
PAs working together in a team-oriented practice and that PAs function as primary care providers in the patient-centered medical home as part of a multidisciplinary, physician-directed clinical team.
Collaborator vs. Competitor?
• What are your thoughts?
-How do you view the future of health care
-Primary care?
-Specialty care?
Educational Changes
Extend NP training period• Require doctorate degree
• Post-doctoral training after completing degree or if changing scope of practice (nurse residency)
Decrease physician training period• AMA has committed $11 million
over 5 year period to fund innovations on medical education
• Create more flexible, individualized learning plans
• Promoting exemplary methods to achieve patient safety, performance improvement and patient-centered team-based care
Trend for primary care
• 33% of physicians are now in primary care (projected to decrease as fewer students choose primary care)
• 52%-66% of NPs are in primary care practice (83% are trained in primary care)
• NPs are also more likely to practice in rural and underserved areas, where a primary care shortage is likely to be more acute
Pauly, MV and Naylor, M. Primary Care Shortages: It’s More Than Just a Head Count. Pen LDI Interdisciplinary Nursing Quality Research Initiative Research Brief. November 2014
Trends for primary care-Physician Assistants• PAs reporting primary
care as their specialty has decreased– 50% in 1997– 43.1% in 2002
• In 2012, 34 percent of practicing PAs reported that their specialty was one of the primary care fields– Family Medicine (25%)– General Internal
Medicine (7%)– Pediatrics (2%)
Virtual Mentor. May 2012, Volume 14, Number 5: 411-414
Trends for specialty care-Physician AssistantsAs of 2012, 63% of PAs practiced within a non-primary care specialty field
-general surgery/surgical subspecialties (25%)-emergency medicine (12%)-internal medicine subspecialties (11%)-orthopedics (9%)-dermatology (4%) -obstetrics/gynecology (2%)
Virtual Mentor. May 2012, Volume 14, Number 5: 411-414
Collaborator vs. Competitor? Final Thoughts
Questions?
References• E.A. Gadbois, et. al. Trends in state regulation of nurse practitioners and physician
assistants, 2001 to 2010. Medical Care Research and Review: MCRR 2015, 72 (2): 200-19 • N.A. Martínez-González, et. al.Task-Shifting From Physicians to Nurses in Primary Care
and its Impact on Resource Utilization: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medical Care Research and Review: MCRR 2015 May 12
• Lenz, et. al. Primary Care Outcomes in Patients treated by Nurse Practitioners or Physicians: Two-Year Follow-Up Med Care Res Rev September 2004 61: 332-351
• Barbara J. Safriet, J.D., L.L.M. 2011. Federal Options for Maximizing the Value of Advanced Practice Nurses in Providing Quality, Cost-Effective Health Care. The Future of Nursing: Leading Change, Advancing Health
• Pearson, L. 2009. The Pearson Report. The American Journal for Nurse Practitioners 13(6).
• RWJF (Robert Wood Johnson Foundation). 2010. Nursing Leadership from Bedside to Boardroom: Opinion Leaders’ Perceptions. Gallup Survey for the Robert Wood Johnson Foundation
• Eiber, C. E., P. S. Hussey, M. S. Ridgely, and E. A. McGlynn. 2009. Controlling Health Care Spending in Massachusetts: An Analysis of Options . Santa Monica, CA: RAND Corporation
• Pauly, MV and Naylor, M. Primary Care Shortages: It’s More Than Just a Head Count. Pen LDI Interdisciplinary Nursing Quality Research Initiative Research Brief. November 2014
• Virtual Mentor. May 2012, Volume 14, Number 5: 411-414





























