Embed Size (px)
Citation preview

The Next Era in GI The Next Era in GI Surgery Surgery BioDynamixTM
AnastomosisThe Colon Ring
Clinical Training Team
BENIGN PATHOLOGYBENIGN PATHOLOGYInflammatory Bowel Inflammatory Bowel
DiseaseDisease

2
Inflammatory Bowel Disease – Overview
• The term inflammatory bowel disease (IBD) covers a group of disorders in which the intestines become inflamed due to unknown factors.
• Two major types of IBD are described: ulcerative colitis (UC) and Crohn’s disease (CD), also known as granulomatous colitis.
• The two entities are different from each other and do not occur together in the same patient.
• Both entities are characterized by remissions and exacerbations.
• When there is severe inflammation, the disease is considered to be in an active stage.
• When the degree of inflammation is less (or absent), the person is often without symptoms.

3
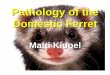
Inflammatory Bowel Disease – Ulcerative Colitis
• Ulcerative colitis is limited to the large intestine.
• The rectum is almost always involved (proctitis), but it may involve rectum and sigmoid (proctosigmoiditis) or the entire colon and rectum (full-blown proctocolitis).
• There are usually no “skip” areas.
Tiny ulcers

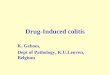
Inflammatory Bowel Disease – Crohn’s Disease
• Crohn’s disease can involve any part of the gastrointestinal tract from the mouth to the anus, but it most commonly affects the small intestine and/or the colon, often with “skip” areas.
Granulomas
“Cobblestone” Street

5
Inflammatory Bowel Disease – Causes
• Researchers do not yet know what causes inflammatory bowel disease. Therefore, IBD is called an idiopathic disease.
• An unknown factor/agent (or a combination of factors) triggers the body’s immune system to produce an inflammatory reaction in the intestinal tract that continues without control.
• As a result of the inflammatory reaction, the intestinal wall is damaged, leading to bloody diarrhea and abdominal pain.

6
Inflammatory Bowel Disease – Symptoms
• Symptoms may range from mild to severe and generally depend upon the part of the intestinal tract involved. They include the following:
Abdominal cramps and pain Severe urgency to have a bowel movement Bloody diarrhea Anemia (due to blood loss) Loss of appetite Weight loss

7
Inflammatory Bowel Disease – Complications
• Intestinal complications of inflammatory bowel disease include the following:
Profuse bleeding from the ulcers. Perforation (rupture) of the bowel. Strictures and obstruction.
In Crohn’s disease, strictures often are inflammatory and frequently resolve with medical treatment.
In ulcerative colitis, colonic strictures should be presumed to be malignant.
Fistulae and perianal disease.These are more common in Crohn’s disease.They may not respond to medical treatment.Surgical intervention often is required, and there is a high risk of
recurrence.

8
Inflammatory Bowel Disease – Complications
Toxic megacolon (acute non-obstructive dilation of the colon):This is a life-threatening complication of ulcerative colitis and
requires urgent surgical intervention.
Malignancy:The risk of colon cancer in ulcerative colitis begins to rise
significantly above that of the general population after approximately 8-10 years of diagnosis.
The risk of cancer in Crohn’s disease may equal that of ulcerative colitis if the entire colon is involved.
The risk of small intestine malignancy is increased in Crohn’s disease.

9
Surgery
• Surgical treatment in persons with inflammatory bowel disease varies, depending upon the disease.
• Ulcerative colitis is a surgically curable disease because the disease is limited to the colon.
• Surgical resection is not curative in persons with Crohn’s disease and is used to treat complications of the disease.
• Excessive surgical intervention in persons with Crohn’s disease can lead to more problems.

10
Surgery – Ulcerative Colitis
• Ulcerative colitis: In about 25-30% of persons with ulcerative colitis, medical
treatment is not completely successful. In such persons and in persons with dysplasia, surgery may be
considered. Options:
First option: removal of the entire colon and rectum (proctocolectomy) with the creation of an ileostomy.
Second option: removal of the colon, creation of an internal ileal pouch (from the small intestine) with attachment to the anal sphincter muscle (ileoanal anastomosis), and creation of a temporary ileostomy. After the ileoanal anastomosis heals, the ileostomy is closed; and passage of feces through the anus is reestablished.

11
Surgery – Crohn’s Disease
• Crohn’s Disease— Even though surgery is not curative in Crohn’s disease,
approximately 75% of patients will require surgery at some point in time for complications.
Options:The most simple surgery for Crohn’s disease is segmental
resection of the involved segment.Ileorectal or ileocolic anastomosis is an option in some
persons who have lower small intestine or upper colonic disease.
In patients with severe perianal fistulae, diverting ileostomy/colostomy is a surgical option.