Embed Size (px)
DESCRIPTION
Dr. Maynard’s presentation on the types of collagen vascular disease in children (presented on 9/22/11).
Citation preview

Collagen Vascular Disease
in Children
Roy Maynard, M.D.
September 22, 2011

2 of 46
Objectives
• Define collagen vascular disease.
• Identify 3 collagen vascular diseases
that affect children.
• Understand the role new biological
modifying agents have on treating
collagen vascular disease.

3 of 46
Definition
• A diverse group of multi-system inflammatory disorders, affecting primarily collagen in the skin and joints. Autoantibody formation and other autoimmune dysfunction suggest a complex immune basis in the pathogenesis of the disease process which remains largely idiopathic

4 of 46
Classification
• Vasculitis
• Arthritides
• Connective tissue disease
• Infectious diseases

5 of 46
Collagen Vascular Disease
• Systemic Lupus Erythematous
• Dermatomyositis
• Scleroderma
• Juvenile Idiopathic Arthritis

6 of 46
Epidemiology
• 150-200 children/million
• 0.015 to 0.02% of children
• Female preponderance
• Fairly uncommon disease in children

7 of 46
Pathogenesis
• Molecular mimicry: Infectious agents alter the surface markers of ones own cells leading to them being recognized as foreign by your immune system.
• Autoimmunity: Idiopathic alterations in the basic immune system leading to the recognition of cells and tissues as foreign and subsequently attack as foreign.

8 of 46
Treatment
• Glucocorticsteroids
• Immunosuppressives
• Immunomodulators
• Anti-inflammatory

9 of 46
Systemic Lupus Erythematosus
• Diagnosis
– Malar rash
– Discoid rash
– Photosensitivity
– Oral ulcers
– Arthritis
– Serositis (pleural or pericardial)
– Renal (proteinuria)

10 of 46
Systemic Lupus Erythematosus
Malar rash
http://www.emedicinehealth.com/script/main/art.asp?articlekey=107976 Accessed on 9/19/11

11 of 46
Systemic Lupus Erythematosus
• Epidemiology
– 0.36 to 0.4 children/100,000
– Girls/boys (4:2 to 7:1)
– Rare diagnosis before age 5
– Peaks young adulthood
– 15-20% of adults started disease in childhood
– Age 12 to 14 years when disease diagnosed

12 of 46
Systemic Lupus Erythematosus
• Diagnosis
– Neurologic (seizures or psychosis)
– Hematologic
• Hemolytic anemia
• Leukopenia
• Lymphopenia
• Thrombocytopenia
– Immunologic disorder
• Positive LE prep
• Anti-dsDNA antibody
• Anti-Smith antibody
• False positive syphilis test
• Antinuclear antibody, C3 and C4
– Other organs
• Kidneys, lungs, cardiac

13 of 46
Systemic Lupus Erythematosus
• Prognosis
– In 1950, only 30% survived 5 years
– Now 5-year survival > 90%
– Pediatric SLE has a worse prognosis than adult SLE
– Risk factors for poor outcome include kidney disease, frequent flares, infections, neuropsychiatric manifestations
– Lower physical and psychosocial than healthy children

14 of 46
Systemic Lupus Erythematosus
• Treatment
– Hydroxychloroquine
– Azathioprine
– Glucocorticoids
– NSAID
– Chemotherapeutic agents • Methotrexate, Cyclophosphamide
– IVIG
– Biologicals - rituximab

15 of 46
Dermatomyositis
• Autoimmune disease
• Primarily affects skin and muscle
• Incidence: under age 16, affects 3,000-5,000 children in U.S. 3 new cases per year/million people
• Average age of onset is 7 (ages 5 – 10)
• Found worldwide, more prevalent in North America
• May be more common in African-Americans
• Adult version presents age 50

16 of 46
Dermatomyositis
• Etiology idiopathic
• Combination of genetics and infection
• May be partially inherited (genetic
predisposition to acquire the disease)
• Not contagious
• More common in females than males

17 of 46
Dermatomyositis
• Signs and symptoms:
– Fever
– Fatigue
– Skin rash
– Muscle weakness
– Pain
– Lung disease
– Joint contractures

18 of 46
Dermatomyositis
Heliotrope rash
http://www.pediatricsconsultantlive.com/pedsquiz/content/article/1803329/1691415 Accessed on 9/20/11

19 of 46
Dermatomyositis
• Diagnosis:
– Clinical diagnosis
– Increased CPK, aldolase, SGOT
– MRI of involved muscles
– Muscle biopsy

20 of 46
Dermatomyositis
http://www.learningradiology.com/caseofweek/caseoftheweekpix2006/cow207lg.jpg Accessed on 9/20/11

21 of 46
Dermatomyositis
http://www.nlm.nih.gov/medlineplus/ency/imagepages/1866.htm Accessed on 9/20/11

22 of 46
Dermatomyositis
• Treatment:
– Prednisone
– Methotrexate
– Hydroxychloroquine
– Cyclosporine
– IVIG
– Mycophenolate

23 of 46
Dermatomyositis
• Prognosis:
– Most children go into remission within 2 years
– Pulmonary involvement heralds poor prognosis
– Increased risk for malignancy
– Joint contractures are a long term complication
– Some do not respond well to medications

24 of 46
Scleroderma
• Autoimmune disease
• Normal tissues replaced with dense, thick scar tissue
• Skin most common site
• Kidneys, heart, lung, GI tract

25 of 46
Scleroderma
• 5,000 – 7,000 children in U.S.
• Only 1.5% develop disease before age 10
• 7% develop disease between age 10 to 19
• 2/3 are female
• Immune system triggers other cells to produce excessive collagen
• Idiopathic
• Not contagious

26 of 46
Pediatric Scleroderma
• Two types:
– Localized scleroderma
• Skin (linear and morphea)
– Systemic scleroderma
• multiple organs

27 of 46
Pediatric Scleroderma
• Localized Scleroderma:
– Most common form in children
– Usually skin only, occasionally underlying muscle
– Linear type appears as a band usually on
extremities, may limit motion when crosses a joint
– Morphea type - patches, waxy skin with an ivory or
white color
– Both appear white with purple borders

28 of 46
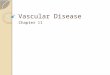
Scleroderma
• Signs and symptoms:
– Loss of stretch in skin
– Discoloration of skin
– Thinning of the skin
– Contractures of fingers
– Joint inflammation
– Raynaud’s phenomenon
– Ulcers on fingertips
– Dysphagia and other GI tract problems
– Fatigue, muscle weakness

29 of 46
Scleroderma
http://www.skinpatientalliance.ca/en/skin-conditions-diseases/connective-tissue-disorders Accessed on 9/20/11

30 of 46
Scleroderma
• Diagnosis:
– Clinical diagnosis
– Skin biopsy
– Autoimmune blood testing
– Swallow study
– Lung testing
– Cardiac echo

31 of 46
Linear Scleroderma
http://bjo.bmj.com/content/91/10/1311/F1.large.jpg Accessed on 9/20/11

32 of 46
Scleroderma
• Treatment:
– Prednisone
– Methotrexate
– NSAID
– Environmental
– Physical therapy

33 of 46
Scleroderma
• Prognosis:
– Chronic and slowly progressive
– Months to years
– Localized vs. systemic
– May stabilize without progression for years

34 of 46
Juvenile Idiopathic Arthritis
• Clinical manifestations: – Fever
– Rash
– Serositis
– Joint involvement pain, swelling, stiffness, limping
– Growth delay/weight loss
– Psoriasis
– Uveitis, eye pain, vision disturbances

35 of 46
Juvenile Idiopathic Arthritis
http://www.google.com/imgres?q=juvenile+idiopathic+arthritis&hl=en&sa=X&rlz=1R2ADFA_enUS410&tbm=isch&prmd=imvnsb&tbnid=27oK6oBuClFabM:&imgrefurl=http://www.isteroids.com/blog/canakinumab-effective-for-systemic-juvenile-
idiopathic-arthritis/&docid=L5cA1hDwO1EF4M&w=200&h=114&ei=gwN5TvKEJ8Watwey0cT2Dw&zoom=1&biw=1440&bih=730&ia
ct=rc&dur=225&page=1&tbnh=91&tbnw=160&start=0&ndsp=20&ved=1t:429,r:12,s:0&tx=89&ty=61)
Accessed on 9/19/11

36 of 46
Juvenile Idiopathic Arthritis
• Diagnosis: – >6 weeks of arthritis
– Less than 16 years of age
– Unknown cause R/O Lyme’s, infection, Kawasaki’s Disease, immunodeficiency
• Epidemiology: – Most common childhood chronic rheumatic
disease
– Incidence: 2-20 cases/100,000
– Prevalence: 16-150/100,000
– 0.07–4.01 per 1,000 children worldwide

37 of 46
Juvenile Idiopathic Arthritis
(ROY—CLARIFY WEBSITE REFERENCE FROM ORIGINAL SLIDE #38)
Accessed on 9/19/11
http://trialx.com/curetalk/wp-content/blogs.dir/7/files/2011/05/diseases/Juvenile_Idiopathic_Arthritis-1.jpg Accessed on 9/20/11

38 of 46
Juvenile Idiopathic Arthritis
Drug Des Devel Ther. 2011; 5:61-70
• Systemic 5-10
• Oligoarthritis 40-50 – Persistent 25-35 – Extended 15-20
• Polyarthritis 30-40 – Rheumatoid factor neg 25-35 – Rheumatoid factor pos 5
• Psoriatic arthritis 5-10
• Other 15-20

39 of 46
Juvenile Idiopathic Arthritis
IMAGE 1: http://images.rheumatology.org/image_dir/album75693/md_99-06-0019.tif.jpg
IMAGE 2: http://www.google.com/imgres?imgurl=http://www.ajronline.org/content/vol185/issue2/images/large/00_04_1385_07a.jpeg&imgrefurl=http://www.ajronline.org/cgi/content-nw/full/185/2/522/FIG17&usg=__M1LQ2tyC2JT86hM8wz41fj-SGpk=&h=1800&w=1037&sz=257&hl=en&start=23&zoom=1&tbnid=aRD8JZwu9_P_6M:&tbnh=150&tbnw=86&ei=e-pfTqadMYi3twf8v6imCw&prev=/search%3Fq%3Djuvenile%2Bidiopathic%2Barthritis%26start%3D21%26hl%3Den%26sa%3DN%26rls%3Dcom.microsoft:en-us%26rlz%3D1I7ADRA_en%26tbm%3Disch%26prmd%3Divnsb&itbs=1)
Accessed on 9/20/11

40 of 46
Juvenile Idiopathic Arthritis
• Pathogenesis:
– Multifactorial autoimmune
– Environmental and genetic factors
– Polygenomic
– European ancestry may be a risk factor

41 of 46
Juvenile Idiopathic Arthritis
• Treatment:
– Non-steroidal
– Steroids
– Disease-modifying anti-rheumatic drugs
• Methotrexate blocks folate interaction so decreased DNA, RNA, proteins
• Sulfasalazine blocks production of proinflammatory prostaglandins
• Leflunamide blocks pyrimidine production, anti-proliferative
– Biological Modifying agents

42 of 46
Juvenile Idiopathic Arthritis
• Biological Modifying agents:
– Etanercept (Enbrel) synthetic protein binds to TNF alpha, prevents TNF from binding to cells
– Infliximab (Remicade) monoclonal antibody to TNF
– Adalimumab (Humira) human monoclonal antibody against TNF
– Abatacept (Orencia) fusion protein blocks stimulation of T cells
– Anakinra (Kineret) interleukin-1 receptor antagonist
– Tocilizumab (Actemra) monoclonal antibody against interleukin-6
– Rituximab (Rituxan) monoclonal antibody against CD20 positive B cells

43 of 46
Juvenile Idiopathic Arthritis
• Prognosis:
– Goal is clinical remission
– Definition of remission: No active
arthritis, fever, rash, serositis,
lymphadenitis, uveitis, normal CRP and
sed rate, no disease activity for 6 months

44 of 46
Long-Term Complications
• Functional limitation
• Osteopenia
• Nutritional deficiencies
• Chronic pain
• Psychological distress
• Infection
• Delayed puberty
• Cancer?
• Death

45 of 46
Conclusion
• Collagen vascular diseases are rare in children
• More common in females than males
• Not contagious
• Etiology largely unknown but genetics and environment may play a role
• New biologic agents may improve the outcome for these patients

46 of 46
Q&A
Thank you for attending!
QUESTIONS?