Embed Size (px)
DESCRIPTION
neuro
Citation preview

1
CNS TUMORSCNS TUMORSAlina Valdes, M.D.

2
Devastating effects High mortality rates Benign tumors may be unresectable so
incurable Malignant if cannot be removed completely Incidence increases with advancing age after
childhood, when second most common cancer No environmental agent known to be causative
except for vinyl chloride with gliomas and CNS radiation with several tumors
No evidence supports viral origin

3
ClassificationClassification World Health Organization classification
Primary tumors classified on basis of cell origin Most primary tumors of neuroepithelial origin
From malignant transformation of astrocytes, ependymocytes, and oligodendrocytes
Gliomas most common Arise from astrocytes
Metastases more likely than primary CNS tumor in patient with known systemic malignant disease

4
Clinical ManifestationsClinical Manifestations Symptoms from intracranial tumors
Compression of brain by tumor and presence of associated edema
Infiltration and destruction of brain parenchyma by tumor cells
Rigid cranial cavity so benign and malignant tumors may cause symptoms

5
Symptoms from primary brain tumors slowly progressive
Symptoms from metastatic tumors more acute Grow more rapidly and associated with
edema Hemorrhage into tumor
May present with generalized symptoms from increased intracranial pressure or focal symptoms from areas of compromise

6
Generalized symptoms Headache
Most common generalized symptom and first in ½ of adults
Infrequently from tumor itself but rather from increased intracranial pressure
Changes in mood or personality Decrease in appetite Nausea Projectile vomiting – in children Generalized or focal seizures – in 20% of
patients

7
Focal symptoms Frontal lobe tumors
May be massive before symptoms cause problems
Progressive difficulty with concentration and memory, personality changes, and lack of spontaneity
Urinary incontinence and gait disorderAppearance of primitive reflexes in bifrontal
disease

8
Parietal lobe tumorsSubtle signs or more dramatic like hemianesthesia
Right: spatial disorientation or left homonymous hemianopia
Left: receptive aphasia or right homonymous hemianopia

9
Temporal lobe tumorsPersonality changes, auditory hallucinations, complex partial seizures, and quadrantanopia
Uncal herniation if large enoughMetastatic spread of primary CNS
tumors to sites outside CNS rareSpread to meninges and spinal cord
occurs with most malignant CNS tumors

10
Patient EvaluationPatient Evaluation Careful neuro exam Contrast-enhanced CT scan or MRI
MRI superior More useful in imaging posterior fossa More sensitive in detecting parenchymal invasion
CT scan without contrast not adequate for primary or metastatic tumors
Cerebral angiography only when tumor blood supply needed prior to resection

11
Biopsy Accurate histological diagnosis Detect other disease like abscess Open craniotomy or MRI-guided or CT-
guided stereotactic techniques In 20% of patients with metastatic tumors,
CNS biopsy helpful in identifying primary site Lumbar puncture
Helpful only if suspect leptomeningeal involvement
Contraindicated when intracranial mass lesion present

12
TreatmentTreatment Surgery
Most patients with primary tumors Many patients with solitary brain metastasis May relieve symptoms for many months if debulk
tumor when surgical cure unlikely No extensive resection with brain stem tumors Radical resection not recommended for tumors in
language or sensorimotor areas, basal ganglia, or corpus callosum due to neuro dysfunction
Not recommended for CNS lymphoma: multifocal and respond to chemo and radiation combination

13
Increased intracranial pressure Most patients have brain edema and benefit
from glucocorticoids, usually dexamethasone
In life-threatening edema with signs of herniation, can give mannitol with dexamethasone
Anticonvulsants Given if develop seizures Given if at risk of developing seizures before
performing biopsy or surgery: many patients don’t need postoperatively

14
Radiation1. Conventional – external beam
• Uses direct X-rays to whole-brain or focal area
• Whole-brain radiation associated with long-term toxicity, like dementia and gait disturbance
2. Brachytherapy• Implantation of permanent or temporary
radiation “seeds” within tumor• Allows higher doses to tumor while
preserving normal tissue
3. “Radiosurgery”• Converging more than 200 beams of
radiation onto small, well-defined tumors

15
Chemotherapy Not used as sole therapy Major obstacle is blood-brain barrier CNS tumors often drug resistant Biodegradable wafers impregnated with
nitrosurea BCNU placed into tumor after resection
Oligodendrogliomas unusually sensitive CNS lymphomas treated with combination
chemo and radiation

16
Malignant AstrocytomasMalignant Astrocytomas Group of heterogeneous tumors:
glioblastoma multiforme, anaplastic astrocytoma, and anaplastic oligodendroglioma
Glioblastoma multiforme Worst prognosis with median survival <12
mos. Surgery and radiation to improve symptoms
and quality of life If relapse, benefit of treatment short-lived

17
Anaplastic astrocytoma and anaplastic oligodendrogliomaMedian survival of 4 to 5 yearsOligodendroglioma or mixed benefit
most from chemo after surgeryRecurrent treated same as
glioblastoma multiforme

18
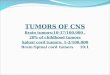
Glioma involving most of the left parietal lobe – seen to the right on this axial CT scan (arrow). The appearance is of a cystic tumor, but biopsy and histological confirmation are necessary to be certain of its nature.

19
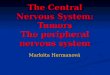
Cystic glioblastoma of the brain stem (arrowed), clearly demonstrated by MRI. The sagittal section shows that the tumor involves the posterior part of the brainstem and extends into the cerebellum.

20
MeningiomasMeningiomas Arise outside brain Generally grow slowly Benign in 90% of cases Complete resection should be attempted Risk of recurrence proportionate to extent
of resection If partial resection, give postop radiation If malignant, radiation given Chemotherapy not used

21
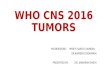
Meningioma in the occipital lobe, as revealed on contrast-enhanced CT scan. The patient presented with a contralateral homonymous hemianopia.

22
CT scan showing a right frontal meningioma with a vascular capsule. The contrast-enhancement technique used in this scan demonstrates the classic appearance of a densely enhancing, sharply marginated tumor, tightly against the dura.

23
MRI picture of a right frontal meningioma (same patient as in slide 21). MRI shows the fissures of the brain more clearly than CT; it shows the tumor well, and parts of its vascular supply appear as hypodense images (arrows).

24
MRI sagitttal view of the patient seen in slides 21 and 22. This view demonstrates the relationship of the meningioma to the dura and skull very clearly, and shows the vascular capsule posteriorly (arrow).

25
CNS LymphomaCNS Lymphoma Increasing in incidence No evidence of lymphoma outside CNS if
primary Most often occur deep in frontal lobe so
less likely to present with seizures than other primary and metastatic CNS neoplasms
Presenting complaints – headache, personality changes, and focal symptoms

26
40% of immunocompetent and nearly 100% of AIDS patients have multifocal lymphoma when diagnosed
>40% of patients have leptomeningeal involvement – rarely symptomatic
20% of patients have involvement of one or both eyes
May be confused with metastatic disease since often multifocal
Surgical resection not indicated

27
Treatment Corticosteroids: cytotoxic effects on
lymphoma cells; not sufficient Combination of systemic chemotherapy
before whole-brain radiation 5-year survival rates with combined
therapy as high as 30% If complete response to chemotherapy,
may defer radiation due to associated late effects

28
Metastatic Tumors to the BrainMetastatic Tumors to the Brain Comprise most of intracranial tumors Common: lung, breast, and melanoma Present with headache, seizures, focal
symptoms, depression, and changes in mental status
Metastases usually multifocal Rapidly growing tumors can cause
massive edema

29
Treatment Corticosteroids – dexamethasone in
brain edema Radiation Surgery possible if solitary or easily
resectable and systemic disease well controlled
Not usually respond to chemotherapy because of blood-brain barrier

30
Multiple cerebral metastases in a patient with carcinoma of the breast, demonstrated on CT scan. Axial ‘cuts’ at other levels in the brain demonstrated further lesions.

31
Spinal Cord TumorsSpinal Cord Tumors Much less common than brain Extradural or intradural
Most extradural are metastasis from other sites
Intradural described as Extramedullary: arising outside spinal cord, e.g.
schwannomas and meningiomas Intramedullary: arising within spinal cord, e.g.
ependymomas and astrocytomas Most common location is thoracic area

32
Symptoms usually from compression of normal structures or compromise of blood supply not invasion of parenchyma
Early symptoms are back pain and distal paresthesias; then loss of sensation and weakness below level of tumor and loss of bowel and bladder control
MRI most useful and mostly replaced myelography
Urgent evaluation if progressive deficits

33
Treatment with surgical resection High-grade astrocytoma followed by
radiation Epidural metastasis treated with high
doses of corticosteroids and surgery or radiation
Surgical decompression if acute onset of symptoms or if pathology not known

34
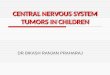
Subdural lipoma demonstrated by MRI in sagittal section. The lipoma (large arrows) is severely compressing the spinal cord (small arrows).