Embed Size (px)
Citation preview

Cairo (40) E-mail: [email protected]
. INTRODUCTION
Osteopenia and Osteoporosis are systemic skeletal disorders characterized by compromised bone strength and mass, with a consequent increase in bone fragility and susceptibility to fracture.
Osteopenia is associated with reduction in the amount of bone in addition to the presence of microarchitectural changes without the occurrence of clinical fracture. Osteoporosis on the other hand is associated with high incidence of clinical fracture.
Cairo Dental Journal (30)Number (1), 1:10January, 2014
CLINICAL EVALUATION OF THE EFFECT OF OMEGA-3 FATTY ACIDS ON OSTEOPOROTIC FEMALES HAVING CHRONIC PERIODONTITIS
Mohamed A. Galal (1); Mushira A. Dahaba, (2); Basma M. Zaki(3) and Hanaa M. Elshenawy (3)
1. Researcher Assistant of Oral Radiology, Department of Oral Medicine & Surgery, National Research Centre, Cairo, Egypt.
2. Professor & Head of Oral Radiology Department, Faculty of Oral & Dental Medicine, Cairo University, Egypt.
3. Researcher of Oral Medicine and Periodontology, Department of Oral Medicine & Surgery, National Research Centre, Cairo, Egypt.
e-mail: [email protected]
. ABSTRACT
The aim of the present study is to assess the effect of Omega-3 fatty acids, as an adjunctive therapy in management of chronic periodontitis in postmenopausal osteoporotic females. Twenty four postmenopausal females having osteopenia or
osteoporosis and chronic periodontitis were included in this study. These patients were divided into two groups: The Omega-3 group (O3) which included 13 subjects. They were given 1gm omega-3 daily, plus Rutin-C and vitamin C (50 mg Rutin + 100 mg vitamin-C) once daily. The second group which is the control group (C): 11 subjects were given Rutin-C and vitamin C once daily. These medications were given for 9 months. Scaling and root planing was done to all patients before starting the medical treatment. Periodontal Indices measured at 6 and 9 months were: Plaque Index (PI), Papillary Bleeding Index (BPI), Pocket depth (PD) and Clinical Attachment Loss (CAL). The results showed that all the periodontal indices improved in both groups after 6 and 9 months intervals, some were significant favoring omega-3 group (PI after 9 months), some were significant favoring control group (PBI after 6 & 9 months, and pocket depth after 9 months), meanwhile, others were non-significant for the two groups (CAL after 6 & 9 months, plaque index and pocket depth after 6 months). It can be concluded that the use of Omega-3 is a beneficial nutritional supplementation in chronic periodontitis cases.
KEYWORDS: Omega-3 Fatty Acids, Rutin-C, Vitamin-C, Osteoporotic/osteopenic females, Periodontal Indices.
مالحظاتصور 4 لونصور 1 لونص األلوانعدد الصفحاتالترقيمرقم املقالة
40

Mohamed A. Galal, et al.(2) C.D.J. Vol. 30. No. (1)
It is characterized by reduction in bone mineral density to below the minimum level required to ensure sufficient mechanical support. There is also deterioration of bone tissues due to imbalance between bone resorption and formation, favoring resorption (Koduganti et al., 2009 and Passos et al., 2010).
Osteoporosis occurs mainly in postmenopausal females; although younger women and men can be also affected. It was estimated that one in four women during menopause and one in three women > 65 years of age are affected by osteoporosis (Passos et al., 2010).
The evaluation of the relationship between osteoporosis and periodontitis is complicated by the fact that both diseases are multifactorial in the etiology. Multiple systemic factors influence the progression of osteoporosis, including age, race, diet, gender, hormone therapy, smoking, genetic factors, exercise, and body weight. Several of these factors are also risk factors for periodontal disease (Al Habashneh et al., 2010).
Several researches support the idea that osteoporosis independently influences alveolar bone height loss. Strategies for reducing osteoporosis risk also may help retard alveolar bone loss, which can be easily fulfilled by meeting dietary intake recommendations (Kaye 2007; Koduganti et al. 2009 and Otomo-Corgel et al. 2012).
Omega-3 fatty acids (FA) are a subset of polyunsaturated fatty acids found in marine sources as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) and in some leafy vegetables, nuts, and oils as α-linolenic acid (ALA) (DeFilippis & Sperling 2006).
Porphyromonas gingivalis (Pg) infected rats treated with omega-3 FA had significantly less alveolar bone resorption. These results demonstrated the effectiveness of omega-3 FA supplemented diet in modulating alveolar bone resorption following Pg infection, and supported that omega-3 FA may
be a useful adjunct in the treatment of periodontal disease (Kesavalu et al. 2006).
Omega-3 fatty acids in another study also slowed the orthodontic incisor separation even after buccal movement of the maxillary first molars, which indicates their effect over bone enforcement (Bartzela et al. 2009).
Another nutritional supplements were also beneficial to periodontal health and affects bone density as well. Rutin and Vitamin C are a common and low-priced combination. Rutin (RT), a quercetin-3-rutinosid or vitamin-P, is considered as one of flavonoid glycosides, which is found in onions, apples, tea and red wine. Rutin is well known to exhibit multiple pharmacological activities including antibacterial, antitumor, anti-inflammatory, anti-diarrheal, antiulcer, anti-mutagenic, vasodilator and immunomodulator. Furthermore, rutin showed an inhibitory effect against membrane lipid peroxidation, as well as antioxidant activities which suggest its protective role in oxidative stress-mediated diseases. Vitamin C is a water-soluble enzyme, abundantly present in different plants and some animals. Ascorbic acid is the most predominant form in the human body and is involved in tissue growth and repair. Ascorbic acid has a potent antioxidant activity and is well known to protect tissues from oxidative injury through efficiently quenching the damaging free radicals produced by many biological processes (Al-Rejaie et al. 2012). Periodontitis is associated with a low concentration of vitamin C in plasma (Pussinen et al. 2003).
The aim of the present study is to assess the effect of omega-3 fatty acids in management of osteoporotic females with chronic periodontitis.
. SUBJECTS AND METHODS
The research was conducted on a selected group of postmenopausal women (≥ 50 years of age) who attended the outpatient clinic in the medical unit of the National Research Center (NRC), Cairo,

CLINICAL EVALUATION OF THE EFFECT OF OMEGA-3 FATTY ACIDS (3)
Egypt for bone densitometry testing in the routine yearly check up. Only women who experienced natural menopause (no menstruation for at least one year) were chosen and invited to participate in this study. They received systemic bone mineral density (BMD) assessment as an initial screening using dual energy x-ray absorptiometry (DXA) of the femur and spine (Norland XR46 version 3.9.6).
Systemic BMD was classified according to the WHO criteria, where osteoporosis was defined as BMD ≥ 2.5 SD (standard deviation) below the optimal mean BMD of young healthy individuals of the same race and gender. Postmenopausal females with BMD T-score less than -2.5 SD, where T-score is the expression of BMD values in terms of standard deviations from the normal value of a female young adult mean were considered osteoporotic and were included in this study. Women with a history of a systemic condition or medication intake that might influence the BMD or periodontal disease severity were excluded i.e., women with a history of diabetes mellitus, thyroid diseases, chronic renal problems, and connective tissue diseases. Postmenopausal females on corticosteroids, chemotherapy, recent peptic or esophageal disorders were also excluded. Exclusion criteria also included postmenopausal females treated with drugs that inhibit gastric acid secretion for more than 2 weeks in the last 6 months; chronic treatment with NSAIDs (non-steroidal anti-inflammatory drugs), hormone replacement therapy or any other drug known to alter bone calcium metabolism were not included. Smoking females were not allowed to participate in the study. All patients were systemically reviewed. The participants were chosen to be of the same socio-economic level. The postmenopausal females who accepted the participation in the study were then referred to the dental clinic at the NRC medical services unit after making prior appointments for evaluation of their oral condition. All participants received further information about the study protocol and objectives at the dental clinic. Participants diagnosed as having chronic periodontitis according to the criteria of the American Academy of
Periodontology (2000) were chosen. Each patient presented with probing depth (PD) ≥ 5 mm in at least three teeth or clinical attachment level (CAL) ≥ 4 to 6 mm and vertical bone loss ≥ 3 mm with no history of periodontal therapy or use of antibiotics in the preceding 6 months was selected to be part of the study. The study included forty non-smoking females, 50-65 years old, who were at least one year postmenopausal, osteopenic or osteoporotic and have not undergone hysterectomy or ovariectomy. All patients were also diagnosed as having chronic periodontitis.
Twenty four postmenopausal osteoporotic or osteopenic females with age ≥50 years were included in the study. Subjects were age-matched into 2 groups:
The Control Group (C); this group comprised eleven patients who were given Rutin C (Rutin 100 mg + Vitamin C 50 mg) once daily, for nine months.
The Omega-3 group (O); this group comprised thirteen patients who underwent took fish-oil gelati-nous capsules rich in omega-3 fatty acids for nine months twice daily (A daily dose of 1000mg Ome-ga-3 PUFA), in addition to Rutin-C ( Rutin 100 mg + Vitamin C 50 mg) once daily as a common medi-cation between Control group and Omega-3 group.
For both groups detailed oral hygiene instructions were given and full mouth scaling and root planing (initial therapy) using ultrasonic scalers and periodontal curettes under local anesthesia completed before starting the dietary supplementations. Scaling and root planing was performed for each patient in two sessions, one session for half and completed over one week. Occlusal adjustment was done whenever indicated.
Periodontal Assessment
Periodontal assessment was carried out at baseline before starting the initial therapy and the dietary supplementations, at 6 and 9 months intervals.

Mohamed A. Galal, et al.(4) C.D.J. Vol. 30. No. (1)
At the baseline evaluation, all clinical parameters were measured and mechanical treatment including removal of all supra and subgingival calcified deposits to obtain a smooth, hard surface was done. Scaling and root planing was carried out by one of the investigators in two successive sessions. Patients were taught and encouraged to maintain their dental health and plaque control through brushing and flossing. All assessment measurements were taken by the same investigator. The condition of all teeth was assessed and recorded. The mean was taken for the following measurements:
Plaque index (PI) according to Silness & Loe (1964) and gingival index (GI) according to Loe and Sillness (1963). Whole mouth probing depth and clinical attachment level and Pocket depth (PD) was measured according to the standard procedure described by Glavind and Loe, 1967 using a periodontal probe with Williams’ calibrations at the free gingival margin and recorded at six locations (mesiobuccal, distobuccal, midbuccal, mesiolingual, distolingual and midlingual) on each tooth parallel to the long axis of the examined tooth. The total of the mean probing depth at the six locations on each tooth for each patient was calculated in millimeters. The distance from the cemento-enamel junction (CEJ) to the free gingival margin and the distance from the free gingival margin to the bottom of the pocket/sulcus were measured at the mesiobuccal and
mid-buccal surfaces using also a calibrated probe. From these two measurements, individual subject mean attachment level (the distance from the CEJ to the bottom of the pocket or sulcus) was calculated in millimeters. All the measurements were taken at baseline, 6 and 9 months intervals.
Ethical Consent:
The study protocol was approved by Medical Research Ethical Committee (MREC) at the National Research Center. A written informed consent was signed by all subjects participating in the study.
Statistical Analysis:
Data were presented as mean and standard deviation (SD) values. Improvements after 6 months and after 9 months were also calculated, and presented as mean and (SD) values as well. T-test were done to compare between the improvements after 6 months of the two groups (Group O) & (Group C), and to compare between the improvements after 9 months of the two groups. The significance level was set at P ≤ 0.05. Statistical analysis was performed with Microsoft Excel 2007 for Windows.
. RESULTS
All Periodontal Indices improved in all groups with different criteria. In Plaque Index Omega-3
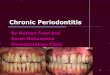
Fig. (1): Sheet of Periodontal Chart used in the experiment.

CLINICAL EVALUATION OF THE EFFECT OF OMEGA-3 FATTY ACIDS (5)
improvement was less than Control improvement at the two intervals, while in the latter indices; Gingival Index, Pocket depth & Clinical Attachment Loss CAL; Control improvement was less than Omega-3 improvement at the two intervals. These improvements were related by t-test at 6 months and 9 months. For Plaque Index the p-values at 6 months and 9 months respectively = 0.09513 & 0.03121*, which is only a significant difference between the two groups at 9 months interval. For Gingival Index, the p-values at 6 months and 9 months respectively = 0.00605* & 0.00119*, which
is a significant difference between the two groups at 6 months and at 9 months intervals, with a favor to control group. For Pocket depth the p-values at 6 months and 9 months respectively = 0.11065 & 0.0245*, which is only a significant difference between the two groups at 9 months interval, with a favor also to control group. Finally, for CAL, the p-values at 6 months and 9 months respectively = 0.27183 & 0.12036, which are non-significant difference between the two groups at 6 months and at 9 months intervals. (Significant at P ≤ 0.05). See Table (1) & Fig (2).
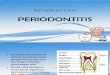
Fig. (2): Improvement in Plaque Index, Gingival Index, Pocket Depth and CAL (means) in 2 groups with time at 6 months and 9 months
TABLE (1): Means and SDs of improvements of all the results after 6 months and after 9 months, and P- value of T-Tests between the two groups:
Index ChangeControl Group Omega-3 Group
P-valueMean SD Mean SD
Plaque Index
After 6 months 0.24 0.17 0.33 0.15 0.09513
After 9 months 0.30 0.19 0.46 0.19 0.03121*
Gingival IndexAfter 6 months 0.286 0.22 0.075 0.11 0.00605*
After 9 months 0.399 0.27 0.068 0.095 0.00119*
Pocket DepthAfter 6 months 0.41 0.32 0.27 0.21 0.11065
After 9 months 0.51 0.27 0.31 0.2 0.0245*
CALAfter 6 months 0.43 0.34 0.34 0.39 0.27183
After 9 months 0.54 0.27 0.39 0.34 0.12036
CAL=Clinical Attachment Loss. *: Significant at P ≤ 0.05

Mohamed A. Galal, et al.(6) C.D.J. Vol. 30. No. (1)
. DISCUSSION
Women are more susceptible to certain chron-ic diseases as they age, which may be affect their periodontal health (Hughes 2010). Osteoporosis is three times more common in women than in men, and bone loss occurs as levels decline, usually from around the age of 50 years (WHO Scientific Group 2003). Consequently, the study sample in our study included postmenopausal female subjects 50 years and older, suffering from osteoporosis, or osteope-nia and chronic periodontitis. In the present work, twenty four subjects were included, and divided ran-domly into two groups: Group O: taking omega-3 supplements twice daily (500 mg) as well as one Rutin-C daily (Rutin 50mg + ascorbic acid (vitamin C) 100 mg), while the control group: (group C) was taking only a single dose of Rutin-C daily.
In the GISSI Prevenzione study 1999 (a large intervention trial of secondary prevention after myocardial infarction) researchers identified a substantial reduction in all-cause and cardiovascular mortality with 1 g per day of n-3 PUFA supplementation. In our study, the same dose was used to test its efficacy in improving alterations in alveolar bone density due to osteoporosis and chronic periodontitis. The same dose was previously recommended by Saravanan et al. 2010.
Salari Sharif et al. 2010 and McMahon 2012 who evaluated the effect of Omega-3 FA on bone biomarkers in osteoporotic postmenopausal women ingesting 900 mg of Omega-3 FA per day for 6 months. Tartibian et al. 2011 examined the effects of long-term aerobic exercise and Omega-3 (O3) supplementation on serum inflammatory markers, bone mineral density (BMD), and bone biomarkers in postmenopausal women. Subjects taking O3 supplementations consumed 1000 mg/d for 24 weeks, similar to the dose applied in our work.
Several researchers suggested increase of this dose especially in chronic periodontitis; as Martinez et al. 2013 constructed their study by
selecting a test group composed of 10 patients with generalized chronic periodontitis (mean age 44 ± 6.4 years) treated with scaling and root planing associated with 4 months of ω-3 supplementation Eicosapentaenoic acid (EPA) + Docosahexaenoic acid (DHA), 3 g/d. Rosenstein et al. 2003 made a clinical trial on thirty adult human subjects with periodontitis who were administered either fish oil 3000 mg daily; borage oil 3000 mg daily; fish oil 1500 and borage oil 1500 mg daily, or placebo. The gingival index, the plaque index (PI), periodontal probing depths and beta-glucuronidase levels in gingival crevicular fluid were measured at baseline and after 12 weeks of treatment.
Vanlint & Ried in 2012 studied BMD and bone turnover at baseline and 12 months, of 40 osteopenic patients, who were randomized to either algal oil containing 400mg docosahexanoic acid (DHA) daily or placebo.
In accordance with these doses and follow-up periods, the participants in the current work were given 1000 mg/d of omega-3 supplements and were followed- up after 6 and 9 months from administration period.
Rutin-C (Rutin 50 mg +Ascorbic acid 100 mg) was applied in our work. Rutin is a common medication for decreasing capillaries fragility and gingivitis in the dental field. Ascorbic acid is Vitamin C with good properties on gingival tissues. McAnulty et al. 2011 recommended its use in a study which examined the effects of 1,000 mg quercetin + 1,000 mg vitamin C, and 400 mg O3 fatty acids ; taken each day for 2 weeks before and during 3 days of cycling at 57% Wmax (Maximal Power Output) for 3 hours on plasma antioxidant capacity, oxygen-radical absorbance capacity (ORAC), plasma oxidative stress, and plasma quercetin and vitamin C levels.
Since periodontal probing is such an important aspect of the periodontal examination, the technique must be systematic and consistent. Bleeding at the gingival margin or sulcus is often

CLINICAL EVALUATION OF THE EFFECT OF OMEGA-3 FATTY ACIDS (7)
the first indicator of gingivitis or periodontitis. Bleeding, pocket depths, and radiographs are used together to determine periodontal condition. These measurements are significant for two different types of periodontal disease and their future treatment. Gingival recession is important to the periodontal examination because it accurately indicates the total amount of attachment loss. Attachment loss can vary from tooth to tooth. Any tooth can have attachment loss without having a pocket. All these indices are established in the literature for diagnosing existing disease, determine the prognosis of individual teeth, and monitor disease progression that tends to be episodic and specific to the tooth and site (ADAA Council on Education 2011).
Hence, in our study we performed a comprehensive clinical examination and measured four parameters or indices of periodontitis which are: plaque index (PI), gingival Index (GI), pocket depth (PD) and clinical attachment loss (CAL) to assure accuracy of collected data in proving the outcome of the proposed medication.
Many experimental studies were done to detect Omega-3 effect on periodontitis and alveolar bone loss. Dietary supplementation with high dose docosahexanoic acid tuna oil caused a marked elevation of O-3 FA levels in oral soft tissues. This diet reduced the amount of alveolar bone loss in a murine experimental periodontitis model compared to a control diet containing no Omega-3 FAs (by an average of 54-72% less alveolar bone resorption in response to the different bacterial infections was detected) (Bendyk 2008).
Indahyani et al. 2008, tested the hypothesis that fish oil alters lipopolysaccharide (LPS)-induced hydroxyapatite loss in rat alveolar bone, and found that the hydroxyapatite contents of alveolar bone in rats treated with fish oil at the same day with or before LPS injection were significantly higher than those in rats injected with LPS alone, but still lower than those in untreated animals.
Kesavalu et al. 2006 have done a study on rats. Rats were fed fish oil (O3 FA) or corn oil diets for 22 weeks and were infected with Pg. Rats on the O3 FA diet exhibited elevated serum levels of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), documenting diet-induced changes. Pg-infected rats treated with O3 FA had significantly less alveolar bone resorption. These results demonstrated the effectiveness of an O3 FA-supplemented diet in modulating alveolar bone resorption following Pg infection, and supported that O3 FA may be a useful adjunct in the treatment of periodontal disease.
These experimental animal studies are in line with our results that proved that partial improvement occurred due to omega-3 FA in chronic periodontitis patients.
Dietary human surveys were done to confirm this relation. “To date, the treatment of periodontitis has primarily involved mechanical cleaning and local antibiotic application. Thus, a dietary therapy, if effective, might be a less expensive and safer method for the prevention and treatment of periodontitis” (Naqvi et al. 2010 and Snider 2010).
Using data from the National Health and Nutrition Examination Survey (NHANES), investigators from Harvard Medical School and Harvard School of Public Health, Boston, found that dietary intake of docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) was associated with a decreased prevalence of periodontitis (by 20%), but linolenic acid (LNA) did not exhibit this association. The cross-sectional study involved more than 9,000 adults between 1999 and 2004 (Naqvi et al. 2010 and Snider 2010).
Iwasaki et al. 2011 studied the longitudinal relationship between two types of O3 dietary intake in presence of periodontal disease in 235 Japanese subjects for whom data were available for the years 2003–2006. O3 intake was assessed at baseline with a brief-type self-administered diet history

Mohamed A. Galal, et al.(8) C.D.J. Vol. 30. No. (1)
questionnaire. Full-mouth periodontal status, measured as the clinical attachment level (CAL), was recorded at baseline and once a year for 3 years.
Still we need confirmation from human clinical trials which are very little in the literature; up to our knowledge.
On the other hand in a very recent study by Martinez et al. 2013 who constructed the methodology of their study that the test group was composed of 10 patients with generalized chronic periodontitis (mean age 44 ± 6.4 years) treated with scaling and root planing associated with 4 months of O3 supplementation eicosapetaenoic acid (EPA) plus docosahexaenoic acid (DHA), 3 g/d. The placebo group was composed of 11 patients (47.9 ± 10.5 years) that received scaling and root planing plus placebo. The periodontal examination included probing depth, clinical attachment level, bleeding on probing and plaque index. They presented that the O3 dietary supplementation had no effect on clinical outcome of treatment.
In our study only little clinical outcome was significant regarding the effect of Omega-3 in comparison to control group since PI improvement was the only significant outcome reported after 9 months in Omega-3 medicated cases. Periodontal indices improved in the current work in both groups after 6 and 9 months, some were significant favoring Omega-3 group (PI after 9 months), others were significant favoring control group (GI after 6 & 9 months, PD after 9 months), and others were non-significant for the two groups (CAL after 6 & 9 months, PI and PD after 6 months).
Also in contrary to our results, Rosenstein et al. 2003 performed a clinical trial on thirty adult human subjects with periodontitis who were administered either fish oil 3000 mg daily; borage oil 3000 mg daily; fish oil 1500 and borage oil 1500 mg daily, or placebo. The modified GI, the (PI), periodontal PD and beta-glucuronidase levels in gingival crevicular
fluid were measured at baseline and after 12 weeks of treatment. Improvement in gingival inflammation was observed in subjects treated with borage oil, with a trend apparent in subjects treated with fish oil or a combination of both. There was no statistically significant improvement in PI, although a trend was apparent in those receiving borage oil. Improvement in PD was seen in those subjects treated with either fish oil alone or borage oil alone, but statistical significance was only seen for the comparison of borage oil and placebo.
Other studies combined Omega-3 with other NSAIDs, for antagonism as the study done by El-Sharkawy et al. 2010 who tried to test their innovative strategy for periodontal treatment using Omega-3 and low dose aspirin. Eighty healthy subjects with advanced chronic periodontitis were enrolled in Mansoura, Egypt, in a parallel-design, double-masked clinical study. The control group was treated with (SRP) and a placebo, whereas the O3 group was treated with SRP followed by dietary supplementation of fish oil (900 mg EPA + DHA) and 81 mg aspirin daily. Statistical analysis demonstrated a significant reduction in PD and a significant attachment gain after 3 and 6 months in the O3 group compared to baseline and the control group. The results of this preliminary clinical study suggested that dietary supplementation with O3 FAs and 81 mg aspirin may provide a sustainable, low-cost intervention to augment periodontal therapy.
Vardar et al. 2005 used another NSAID; i.e. Celecoxib. The results of the that study indicated that celecoxib and Omega-3 fatty acid, when used individually, show a rather partial effect on the control of the analyzed mediators, but when combined they show a synergic effect and provide significant reductions in the gingival tissue levels of prostaglandin E2 (PGE2), prostaglandin F2α (PGF2α), leukotriene
B4 (LTB4), and platelet activating factor (PAF) in LPS-induced experimental periodontitis

CLINICAL EVALUATION OF THE EFFECT OF OMEGA-3 FATTY ACIDS (9)
(Experimental periodontitis was induced by repeated injection of Escherichia coli endotoxin). These findings may pioneer further clinical human studies investigating the possible place of celecoxib and Omega-3 fatty acid in periodontal treatment.
This is in line with our study results which proved that Omega-3 supplemental medications have a positive impact on treatment of chronic periodontitis, but with a weak relation clinically (not all indices improved significantly), and this relation even with the high dose given in these studies (3gm – 6 gm /day), suggest that Omega-3 when used individually is not effective.
Many of these studies focused on cellular factors more than clinical indices, which makes Omega-3 in such ways preventive more than being therapeutic, rendering it of low grade importance in periodontitis if compared to antibiotics.
. REFERENCES
1. ADAA Council on Education. Gingival Health - Periodontal Assessment. Crest® Oral-B® at dentalcare.com Continuing Education Course, Revised August 17, 2011.
2. Al Habashneh R., Alchalabi H., Khader Y. S., Hazza’a A.M., Odat Z, and Johnson G.K. : Association Between Periodontal Disease and Osteoporosis in Postmenopausal Women in Jordan. J Periodontol., 2010; 81:1613-1621.
3. Al-Rejaie SS, Abuohashish HM, Alkhamees OA, Aleisa AM and Alroujayee AS. Gender difference following high cholesterol diet induced renal injury and the protective role of rutin and ascorbic acid combination in Wistar albino rats. Lipids in Health and Disease 2012, 11:41.
4. Bartzela T, Türp JC, Motschall E and Maltha JC. Medication effects on the rate of orthodontic tooth movement: A systematic literature review. Am J Orthod Dentofacial Orthop. 2009 Jan;135(1):16-26.
5. Bendyk A. The effect of dietary Omega-3 polyunsaturated fatty acids on experimental periodontitis lesions in the mouse. Doctorate Thesis of clinical dentistry (Periodontics) submitted to the University of Adelaide. Australia. 2008.
6. DeFilippis AP and Sperling LS. Understanding omega-3’s.
Am Heart J 2006 Mar;151(3):564- 70.
7. El-Sharkawy, H, Aboelsaad N, Eliwa M, Darweesh M, Alshahat M, Kantarci A, Hasturk H and Van Dyke TE. Adjunctive Treatment of Chronic Periodontitis with Daily Dietary Supplementation with Omega-3 Fatty Acids and Low-Dose Aspirin. Journal of Periodontology. November 2010, Vol. 81, No. 11, Pages 1635-1643.
8. GISSI-Prevenzione Investigators (Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico). Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Lancet 1999; 354: 447–55.
9. Hughes P. Aging, Systemic Disease and Oral Health: Implications for Women Worldwide (Part I). Crest® Oral-B® at dentalcare.com Continuing Education Course, Revised December 9, 2010.
10. Indahyani DE, Santoso ALS, Utoro T, Soesatyo MHNE and Sosroseno W. Effect of fish oil on lipopolysaccharideinduced hydroxyapatite loss in rat alveolar bone: A Preliminary Study. Online J Health Allied Scs. 2008;7(4):7.
11. Iwasaki, M, Taylor GW, Moynihan P, Yoshihara A, Muramatsu K, Watanabe R and Miyazaki H. Dietary ratio of n-6 to n-3 polyunsaturated fatty acids and periodontal disease in community-based older Japanese: A 3-year follow-up study. Prostaglandins, Leukotrienes and Essential Fatty Acids 85 (2011) 107–112.
12. Kaye EK. Bone health and oral health. J Am Dent Assoc. 2007 May;138(5):616-9.
13. Kesavalu L, Vasudevan B, Raghu B, Browning E, Dawson D, Novak JM, Correll MC, Steffen MJ, Bhattacharya A, Fernandes G and Ebersole JL. Omega-3 Fatty Acid Effect on Alveolar Bone Loss in Rats. J Dent Res. 2006 Jul;85(7):648-52.
14. Koduganti RR, Gorthi C, Reddy PV and Sandeep N. Osteoporosis: “A risk factor for periodontitis”. J Indian Soc Periodontol. 2009 Sept;13(2):90-6.
15. Martinez GL, Koury JC, Brito F, Fischer RG, Gustafsson A and Figueredo CM. The impact of non-surgical periodontal treatment on serum levels of long chain-polyunsaturated fatty acids: a pilot randomized clinical trial. J Periodontal Res. 2013 May 31.
16. McAnulty SR, Nieman DC, McAnulty LS, Lynch WS, Jin F and Henson DA. Effect of mixed flavonoids, n-3 fatty

Mohamed A. Galal, et al.(10) C.D.J. Vol. 30. No. (1)
acids, and vitamin C on oxidative stress and antioxidant capacity before and after intense cycling. International Journal of Sport Nutrition and Exercise Metabolism;2011, 21(4):328-337.
17. McMahon MS. Beneficial Effect of Omega-3 Fatty Acids on Bone Metabolism. Sept. 2012, Vol. 35, No. 9:735 -6.
18. Naqvi AZ, Buettner C, Phillips RS, Davis RB and Mukamal KJ. N-3 Fatty Acids and Periodontitis in US Adults. J Am Diet Assoc. 2010;110:1669-1675.
19. Otomo-Corgel J, Pucher JJ, Rethman MP, Reynolds MA. State of the Science: Chronic Periodontitis and Systemic Health. J Evid Base Dent Pract 2012:S1:[20-28]
20. Passos J. D., Gomes-Filho I. S., Vianna M. I. P., da Cruz S.S., Barreto M. L., Oliveira T. J., Borges L. D., and Monteiroi F.M. Outcome Measurements in Studies on the Association between Osteoporosis and Periodontal Disease. J Periodontol., 2010; 81:1773-1780.
21. Pussinen PJ, Laatikainen T, Alfthan G, Asikainen S and Jousilahti P. Periodontitis Is Associated with a Low Concentration of Vitamin C in Plasma. Clinical and Diagnostic Laboratory Immunology, Sept. 2003, Vol. 10, No. 5: p. 897–902.
22. Rosenstein ED, Kushner LJ, Kramer N, Kazandjian G. Pilot study of dietary fatty acid supplementation in the treatment of adult periodontitis. Prostaglandins Leukot Essent Fatty Acids. 2003 Mar;68(3):213-8.
23. Salari Sharif P, Asalforoush M, Ameri F, Larijani B, Abdollahi M. The effect of n-3 fatty acids on bone biomarkers in Iranian postmenopausal osteoporotic women: a randomized clinical trial. Age (Dordr). 2010; 32(2):179-186.
24. Saravanan P, Davidson NC, Schmidt EB, Calder PC. Cardiovascular effects of marine omega-3 fatty acids. www.thelancet.com Published online July 16, 2010.
25. Snider J. Polyunsaturated fatty acids may help treat, prevent periodontitis, study finds. JADA 2010;141(12):1418.
26. Tartibian B, Maleki BH, Kanaley J, Sadeghi K. Long-term aerobic exercise and omega-3 supplementation modulate osteoporosis through inflammatory mechanisms in post-menopausal women: a randomized, repeated measures study. Nutrition & Metabolism 2011, 8:71.
27. Vanlint SJ and Ried K. Efficacy and tolerability of calcium, vitamin D and a plant-based omega-3 oil for osteopenia: A pilot RCT. Maturitas 2012;71:44-48.
28. Vardar, S, Buduneli E, Baylas H, Berdeli AH, Buduneli N and Atilla G. Individual and Combined Effects of Selective Cyclooxygenase-2 Inhibitor and Omega-3 Fatty Acid on Endotoxin-Induced Periodontitis in Rats. J Periodontol 2005;76:99-106.
29. WHO Scientific Group on the Prevention and Management of Osteoporosis (2000: Geneva, Switzerland). Prevention and management of osteoporosis: report of a WHO scientific group. (WHO technical report series; 921), 2003.