Embed Size (px)
Citation preview
S
Clinical Decision
Support SystemsRachel Bayles Lacey
Current Research
S Clinical decision support systems for utilization of CT in
the emergency department
S Authors: Ivan K. Ip and Frank S. Drescher
S Imaging in Medicine. 4.6 (Dec. 2012): pg. 605

Primary Question
S How have clinical decision support systems impacted
diagnostic imaging?
S X-rays
S Computed tomography (CT) scans
S Nuclear medicine scans
S Magnetic resonance imaging (MRI) scans
S Ultrasound

Risk of Overutilization
S Increased cost
S US$11.4 billion Medicare beneficiaries (2007)
S Increased radiation exposure
S Estimated 29,000 cancers a year in the U.S. are related to
CT scans
Overdiagnosis
S Unnecessary follow-up imaging
S Additional unnecessary procedures and treatments
S Finding many “false positives” which increase stress for
patient
Non-medical Reasons
S Doctors order more tests to cover their liability (defensive
medicine)
S Financial incentives to order more test and more
procedures (physician self-referral)
S Traditional “symptom” checking not being taught in
medical school
CPOE/CDSS
S Computerized physician order entry (CPOE)
S Provide instructions for patient care
S Embedded clinical decision support system (CDSS)
S Provides alerts and/or reminders
S Wide range of options
S Hard stops that prevent order altogether/require override
S Simply educational
CDSS
S Shown to improve physician performance, safety, and
outcomes
S Improvements
S Diagnosis
S Preventive Care
S Disease management
S Drug dosing and prescribing
Why imaging in ED?
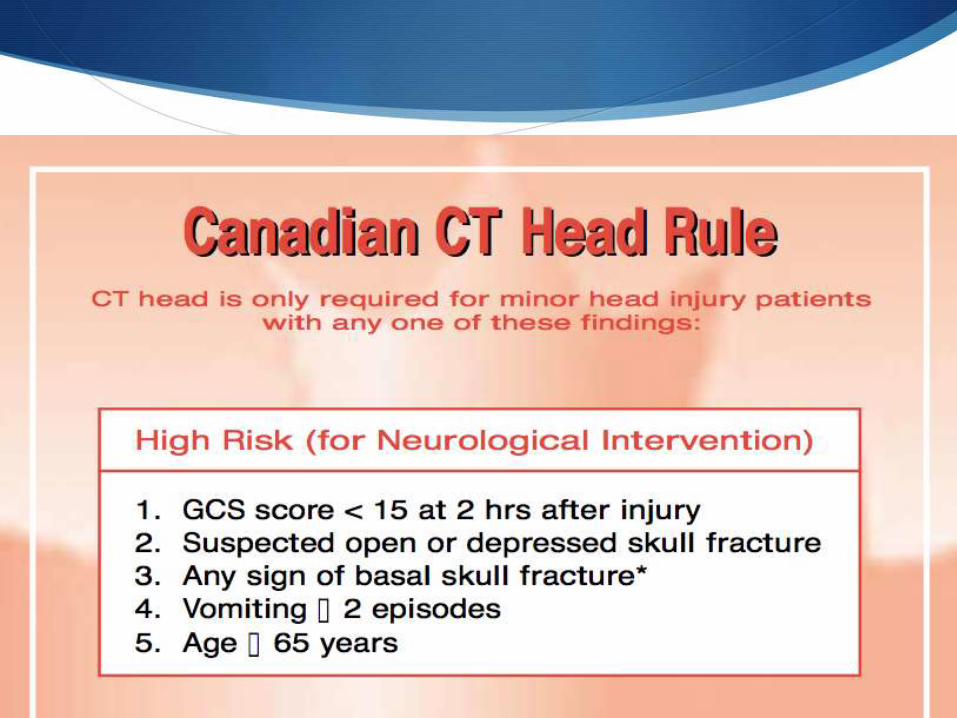
S Many clinical decision rules have been developed and
validated
S Canadian CT head rule
S New Orleans criteria
S Ottawa ankle and knee rules
S NEXUS for cervical spine imaging
S However, policy has not translated well into clinical
practice
Why imaging in ED?
S Increase in medical imaging most evident in emergency
department
S Use of CT/MRI for injury-related conditions
S 6% in 1998
S 15% in 2007
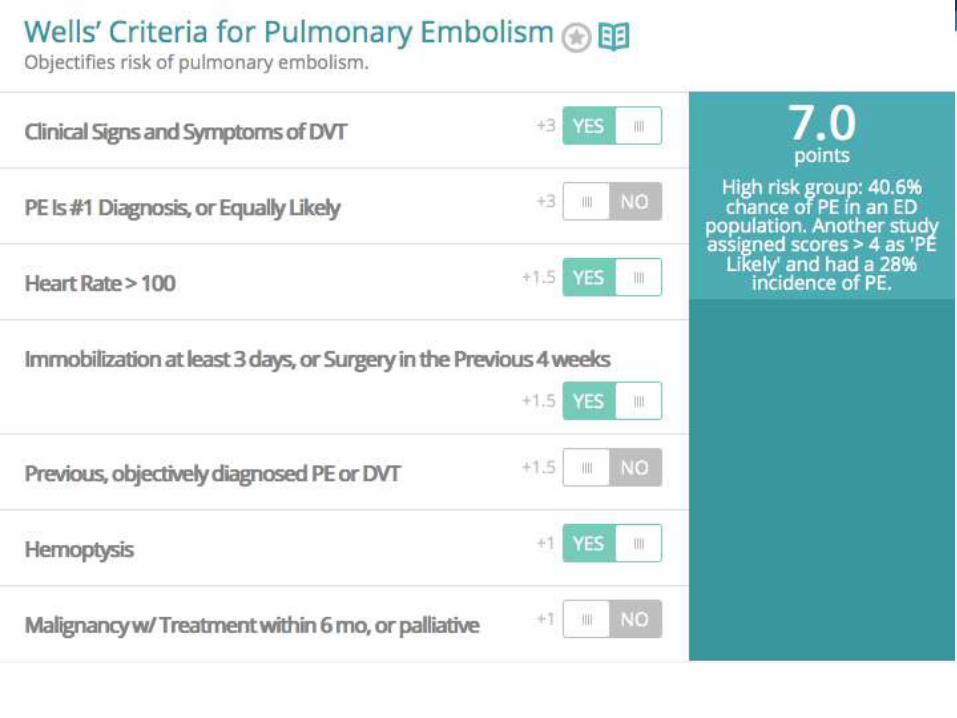
Clinical Prediction Scores
S Need strong evidence
S Translatable to actionable automated decision support
S Wells Criteria
S venous thromboembolism
CDSS Intervention
S Overall reduction in inappropriate diagnostic imaging for
suspected PE
S Pre-intervention
S 35% not adherent to guidelines
S Post-intervention
S 22% not adherent to guidelines
CDSS Intervention
S Before implementation
S Quarterly use of CT rose 82.1%
S 14.5 to 26.4 CT scans/1000 patients
S After implementation
S Quarterly use decreased by 20.1%
S 26.4 to 21.1 CT scans/1000 patients
Study was over a period of six years
Unnecessary radiation
S Passive reminder
S Patient has received more than five CT scans within the
prior 365 days
S Showed no significant change in physician ordering
habits
Effective CDSS
S Speed
S Anticipation of needs and delivery in real time
S Fitting the users’ workflow
S Usability
S Recognition of physician resistance
Effective CDSS
S Altering rather than stopping behavior
S Simplicity
S Minimum amount of information
S Monitoring and maintaining knowledge-based systems
Effective CDSS
S Concise
S Context specific
S Relevant to clinician’s current decision
S Provide a recommendation rather than just an assessment
S Justification of decision support by providing research evidence
S Promotion of action rather than inaction
Most persuasive forms of
evidence
S Peer-reviewed literature; particularly those that include
S Decision-making rule
S Cost-effectiveness analysis
S Practice guidelines
S American College of Radiology Appropriateness Criteria
S American Heart Association Cardiac Imaging Guidelines
S http://www.acr.org/Quality-Safety/Appropriateness-Criteria
S Easily translatable to context-specific actions/not vague reminders
Organizational Culture
S Quality
S Safety
S A clearly stated vision from the highest levels of the
organization
Reasons for lack of high
quality evidence
S Researchers is at intersection of fields
S Outcomes research
S Implementation research
S Systems redesign
S HIT changes at rapid pace
Barriers
S Financial barriers to CDSS implementation
S Physicians' resistance to CDSS
S Interoperability issues
S Fee-for-service provides financial disincentive to
decrease number of imaging procedures
Questions
S Where should the responsibility ultimately lie for making a
decision about image ordering?
S Physicians?
S Patients?
S Hospital Administration?
S Clinical Decision Support System?
S Insurance Providers?
S Taxpayers?
Questions
S Would you personally be more concerned with excess
radiation exposure or with a misdiagnosis?
S For potential tumor?
S For chest pain?
S For leg swelling?