website: http://www.am-medicine.com Facebook page : https://www.facebook.com/pages/Am-medicine/207726329406832 Facebook group: https://www.facebook.com/groups/1409138472653811/
- 1. MOB TCDClinical Anatomy of the Back Professor Emeritus Moira
OBrien FRCPI, FFSEM, FFSEM (UK), FTCD Trinity College Dublin
2. MOB TCDProgressTime Goh et al. Clin Biomech 1999;14:439 3.
MOB TCDSpine Consists of Cervical Vertebrae Thoracic Vertebrae
Lumbar Vertebrae Sacrum 4. MOB TCDSpine The strength of the
skeletal column is due to the size and shape of the vertebrae Its
flexibility is due to the many joints that are close together 5.
MOB TCDVertebral Column Lot of stress in variety of sports Cervical
pathology Pain may be referred to upper limb Lumber pathology Lower
limb 6. MOB TCDYoung SpineNormal curvature of infants spineNormal
lumbar curve of toddlers spine 7. MOB TCDLow Back Pain in Sports
70% of population will suffer from back pain at some time 10% - 15%
of sports injuries are spinal injuries 0.6% - 1% have neurological
complications Deyo & Tsui-Wu. Spine 1987;12:264-8 8. MOB TCDLow
Back Pain in Sports Majority of sports injuries to lumbar spine
Soft tissue and many are not reported Fractures Fracture
dislocation Abrasions, bruising Contusions Tall & De Vault.
Clin Sports Med 1993;12:441-8 9. MOB TCDLow Back Pain in Sports
Must know the sport Must understand the biomechanics and stresses
involved in the sport Must examine the spine in the appropriate
position 10. MOB TCDTypical Vertebrae Basic parts Body and neural
arch Which consists of pedicles, lamina and spine The transverse
processes arise from the pedicles Superior and inferior articular
processes 11. MOB TCDLumbar Vertebrae 12. MOB TCDLumbar Vertebrae
Body kidney shaped No articular facets for ribs Inferior facets
face anterolateral Superior facets face posteromedial
Intervertebral notch increase in size Accessory processes base of
transverse process Mammillary process on posterior aspect of
superior articular process 13. MOB TCDLumbar Vertebrae Body is
convex anteriorly Foramina on the posterior aspect are for the
basic vertebral veins, which drain into the internal vertebral
plexus The walls of the veins, which are valve less, have afferent
nerve fibers Secondaries can spread from pelvis, prostate, adrenal
glands lungs and breast 14. MOB TCDLumbar Vertebrae The superior
and inferior surfaces of the body are flat and covered by a thin
layer of hyaline cartilage The body of the vertebra consists of
trabecular or cancellous bone 15. MOB TCDTypical Lumbar Vertebrae
Superior and inferior articular processes Arise from the junction
of the pedicles and lamina Superior face posteromedially With rough
mammillary processes on the posterior border Inferior face
anterolaterally Accessory processes at the base of transverse
process Prevents rotation 16. MOB TCDThe Lumbar Facets Vary from
the sagittal disposition at the first and second, to almost coronal
in the lower Facet tropism is when the facet on one side is in the
sagittal plane and the other is in the coronal plane, which adds to
rotational stress This change may occur in the lower thoracic
vertebrae 17. MOB TCDPars Interarticularis Pars interarticularis
Portion of lamina between superior and inferior articular processes
Site of spondylolysis or spondylolisthesis 18. MOB TCDLumbar Spine
Cancellous bone 50% compressive strength Facet joints 20% in
standing upright position 19. MOB TCDLumbar Vertebrae 20. MOB
TCDLumbar Vertebrae 21. MOB TCDLumbar Spine Cancellous bone 50% of
the compressive strength Facet joints, 20% of the strength in the
standing upright position 22. MOB TCDAnterior Longitudinal Ligament
Attached mainly to the bodies This ligament helps to prevent us
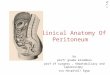
from leaning too far back (hyperextension) 23. MOB TCDPosterior
Longitudinal Ligament Attached mainly to the inter vertebral discs
This ligament helps to restrict forward bending (hyperflexion) 24.
MOB TCDLigamentum Flava Runs between the laminae of the neural
arches Helps to restrict hyperflexion It extends to the capsule of
the facet joint It is highly elastic and ensures that the ligament
does not buckle in extension 25. MOB TCDLigamentum Flava Gives
elasticity to the posterior aspect of the facet joints Helps form
the posterior boundary of the intervertebral foramen The ligamentum
flava is thicker in the lumbar region 26. MOB TCDSpinal Ligaments
Interspinous ligaments Strong supraspinous ligaments The
inter-transverse ligaments join the transverse processes and are
thin and membranous in the lumbar region 27. MOB TCDFifth Lumbar
Vertebrae Larger, superior and inferior articular facets in the
same plane Fifth lumbar vertebrae has large transverse processes
Arise from the body as well as the pedicles 28. MOB TCDArthritis of
Spine Painful Limitation of movement Extra projections Narrowing of
disc spaces 29. MOB TCDVertebral Joints Secondary cartilaginous
joints between the bodies Hyaline cartilage covering bodies Disc of
fibrocartilage in between Synovial plane joints between the facets
30. MOB TCDIntervertebral Discs Annulus fibrosis Concentric lamina
run obliquely Type I collagen at periphery, type II near nucleus
Weakest portion is the postero-lateral and posterior Periphery has
a nerve supply 31. MOB TCDNucleus Pulposus Gelatinous, hydrophilic,
proteoglycan gel in collagen matrix Lies posterior in the disc
There are no nerve endings in a mature disc Nerve endings are found
in the posterior longitudinal ligament and the dura Nutrition of
the disc is by diffusion via the central 40% of the cartilaginous
end plate The discs are thicker in the cervical and lumbar sections
of the vertebral column Where there is more movement. The largest
disc is between L5 S1 32. MOB TCDNucleus Pulposus Hydration of the
annulus and nucleus is proportional to the applied compressional
stress In vivo, there is a loss of 1 cm standing height over the
course of the day A disc loaded in vitro for four hours by 100%
body weight will lose 6% of the fluid from the nucleus and 13% from
the annulus May be due to end plate fracture There is more
rotational stress in the posterior part of the disc 33. MOB
TCDNucleus Pulposus The position of the spine determines where the
compressional forces are greatest The posterior longitudinal
ligament is thin and expanded at the level of the disc High
compressional loading at L4,L5,S1 may be due to end plate fracture
and not to rupture of the annulus End plate failure is a possible
precursor of disc degeneration 34. MOB TCDAxial Load and End-plates
35. MOB TCDEnd-plate Mechanics Functionally, the vertebral
end-plate displays characteristics of a trampoline With the
sub-end-plate trabecular bone acting as springs to sustain and
dissipate axial load Despite the thinness of the vertebral
end-plate The hydraulic nature of marrow and blood vessels within
the vertebral body, act to dampen axial loads, unless the local
point pressure is too high 36. MOB TCDEnd-plate Mechanics End-plate
lesions can be induced experimentally before a disc will prolapse
through the anulus, suggesting a protective mechanism over annular
injury and potentially cord or root compression Excessive loads may
result in perforation of the end-plate, usually in the region of
the nucleus and often in the path of the developmental notchord 37.
MOB TCDEnd-plate SusceptibilityNotochord Schmorl & Junghanns.
The human spine in health and disease. New York: Grune &
Stratton, 1965 38. MOB TCDFacet Joints L1,L2 Facets sagittal plane
Lower joints in coronal plane Synovial plane joints Meniscoid
structures Synovial membrane some contain fat Supplied by medial
branch of dorsal ramus 39. MOB TCDFacet Joints Narrowing of disc
space, results in stress on facet joint Highest pressure during
Combined Extension Rotation Compression 40. MOB TCDFacet Joint
Syndrome Extension and rotation Pain rising from flexion Pain worse
standing Lateral shift in extension Point tenderness over facet
Referred leg pain 41. MOB TCDSegmental RotationSinger et al. J
Musculoskel Res 2001;5: 45-55 42. MOB TCDMovements of Lumbar Spine
Flexion limited by disc problems Lateral flexion Extension limited
by facet joint problems Very little rotation Extension and rotation
affect facet joints 43. MOB TCDNerve Supply Nerve supply Peripheral
annulus Facet joint Nerve is medial branch dorsal ramus 44. MOB
TCDBlood Supply Lumbar arteries Internal venous plexuses External
venous plexuses Basivertebral veins Valveless 45. MOB TCDLumbar
Vertebrae 46. MOB TCDCancellous Bone Cancellous bone 50%
compressive strength Facet joints 20% in standing upright
positionNormal boneOsteoporotic bone 47. MOB TCDAnatomical
Abnormalities Spina Bifida Occulta Facet Tropism Kyphosis Scoliosis
48. MOB TCDAnatomical AbnormalitiesKyphosisScoliosis 49. MOB
TCDAnatomical Abnormalities Hemi-vertebra Spina Bifida Occulta
Facet Tropism Scoliosis Kyphosis 50. MOB TCDAnatomical
Abnormalities Unilateral lumbarisation Unilateral sacralisation 51.
MOB TCDThe Spine in Sports Spine injury epidemiology Contact vs.
non-contact sports Spine injury mechanisms Overuse overload
overlooked Vertebral end-plate injury Disc injury Future issues 52.
MOB TCDEpidemiologyCooke & Lutz. Phys Med Rehab Clinics N Am
2000;11:837 53. MOB TCDEpidemiology Back pain in the community is
60% - 80% Recurrence of back pain is 70% - 90% Progression to
chronic back pain is 5% - 10%Cooke & Lutz. Phys Med Rehab
Clinics N Am 2000;11:837-65 54. MOB TCDLow Back Pain in Sports
Majority of sports injuries are to the lumbar spine Many soft
tissue injuries are not reported Fractures Fracture dislocation
Abrasions, bruising Contusions Tall & De Vault. Clin Sports Med
1993;12:441-8 55. MOB TCDChronic Low Back Pain Local structures
Muscles Ligaments Poor lifting techniques Joints Bones 56. MOB
TCDBack Pain Local structures Muscles, ligaments Joints Referred
pain Abdominal organs Pelvic organs Must out rule Infection Tumours
57. MOB TCDAcute Low Back Pain Non-specific low back pain Usually
settles quickly History Examination Pain relief Stay as active as
possible within limit of pain 58. MOB TCDAcute Low Back Pain Nerve
root pain Leg pain worse than back pain Numbness and pins and
needles Neurological signs Refer to specialist If it does not
resolve in first 4 weeks 59. MOB TCDInvestigate Low Back Pain Under
20 or over 55 years Non-mechanical pain Past history cancer
Thoracic pain Steroids or HIV Unwell, weight loss Widespread
neurology Structural deformity Gait disturbance or sphincter
disturbance 60. MOB TCDChronic Low Back Pain Pain referred
Abdominal organs Pelvic organs Must out rule Infection Tumours 61.
MOB TCDPain Referred 62. MOB TCDYoung Athlete Junior rugby team 15
years of age M. Scheuermann 5 Spina bifida occulta The scrum half
had degenerative facet joint changes 63. MOB TCDSacroiliac Joint
Sciatic Nerve 64. MOB TCDSpinal Stenosis Congenital or acquired
Abnormally short pedicles or lamina Formation of osteophytes
Osteo-arthritis of facet joints Pain aggravated by walking Relieved
by rest 65. MOB TCDSpinal Stenosis 66. MOB TCDPredisposing Factors
Intrinsic factors Anatomical abnormalities Biomechanical Extrinsic
factors Sport Surfaces Equipment Training 67. MOB TCDPredisposing
Factors Back Pain Poor posture Overweight Unfit 68. MOB
TCDPredisposing Factors Poor core stability Weak abdominal muscles
Weak gluteal muscles Muscle imbalance 69. MOB TCDPredisposing
Factors Poor core stability Weak abdominal muscles Weak gluteal
muscles Muscle imbalance Pronated or cavus feet 70. MOB
TCDPredisposing Factors Badly designed furniture No back support
Poor posture at work 71. MOB TCDAcute Low Back Pain 72. MOB
TCDAnnular tears Loaded compression with rotatory component As
little as 3 degrees of high torque rotation Facets protect disc As
annulus fails, facets joints may be injured 73. MOB TCDAnnular
Bulge 74. MOB TCDDisc Lesion 75. MOB TCDYoung Athlete Junior rugby
team 15 years of age M. Scheuermann 5 Spina bifida occulta The
scrum half had degenerative facet joint changes 76. MOB
TCDScheuermanns DiseaseGreene et al. J Pediatr Orthop 1985;5:1 77.
MOB TCDSpondylolisthesis 78. MOB TCDPars Interarticularis Pars
interarticularis, portion of lamina between superior and inferior
articular processes Site of spondylolysis or spondylolisthesis 79.
MOB TCDSpondylolisthesis 80. MOB TCDSpondylolysis and
Spondylolisthesis 81. MOB TCDPars Interarticularis; Facet Joint 82.
MOB TCDSpondylolisthesis Rapid Flexion and Extension Gymnastics,
flips Vaulting Ballet, arabesque Lifting during dance Diving
Butterfly swimming Decathlon Pole vaulting 83. MOB TCDAnkylosing
Spondylitis, Infection 84. 465 Athletes Low Back Pain (M318;F147)
male (39) female(14) Spina Bifida Occulta (SBO) 6.6%(21) 4.1%(6)
Lumbarisation 3.5%(11) 1.4%(2) Sacralisation 2.2% (7) 6.1% (9)
Spondylolisthesis (13) 30% had SBO; 21 of 56 had other pathologyMOB
TCD 85. MOB TCDMechanism of Injuries Compression or weight loading
Torque or rotation Tensile stresses produced by excessive motion of
spine Hyperextension and flexion Watkins & Dillin, 1985 86. MOB
TCDCompression or Weight Loading Sports requiring Massive strength
High body weight Weight lifter Hooker and No 8 Wrestling Line back
American footballWatkins & Dillin, 1985 87. MOB TCDWeight
Lifting 40 % weight lifters have low back pain Greatest stress is
when weight is lifted above the head Dangerous time is shift from
spinal flexion to extension Aggrawal et al. Br J Sports Med
1979;13:58-61 88. MOB TCDAxial Compressive Loading Head on
collisions Motor sports Boating accidents Wrestling Horseback
riding Bicycling Bobsleigh 89. MOB TCDAxial Compressive Loading 90.
MOB TCDAxial Compressive Loading 91. MOB TCDAxial Compressive
Loading 92. MOB TCDCompression Stress 93. MOB TCDRotational Stress
94. MOB TCDRotational Stress 95. MOB TCDSpondylolisthesis Rapid
Flexion and Extension Gymnastics, flips Vaulting Ballet, arabesque
Lifting during dance Diving Butterfly swimming Decathlon Pole
vaulting 96. MOB TCDAustralian Football LeagueSeward & Orchard.
2000 AFL Injury Report, Australian Sports Commission 97. MOB
TCDGolf Highest incidence of back injuries in professional sports
Torsional stress is lessened by spreading the stress over the
entire spine Rigid abdominal control Parallel shoulders and pelvis
Watkins and Dillin, 1985 98. MOB TCDSustained Postures -
Hyperextension 99. MOB TCDSustained Postures - Hyperextension 100.
MOB TCDSustained Postures - Hyperextension 101. MOB TCDSustained
Postures - Flexion 102. MOB TCDScoliosis due to Unilateral Sports
Racquet sports Fencing Sweep rowing Javelin Freestyle unilateral
breathing 103. MOB TCDScoliosis due to Unilateral Sports 104. MOB
TCDRunning Poor posture Poor abdominal Pronated feet Muscle
imbalance Leg length discrepancy Osteoporosis 105. MOB TCDCricket
Bowlers Rotational forces Extension followed by rotation and
flexion 106. MOB TCDThank You 107. BMJ Publishing Group Limited
(BMJ Group) 2012. All rights reserved.