Embed Size (px)
Citation preview
CLASSIFICATION OF ARTERIAL DISEASE and
INVSTIGATIONS
DR SUMER YADAV
MCh - PLASTIC SURGEON
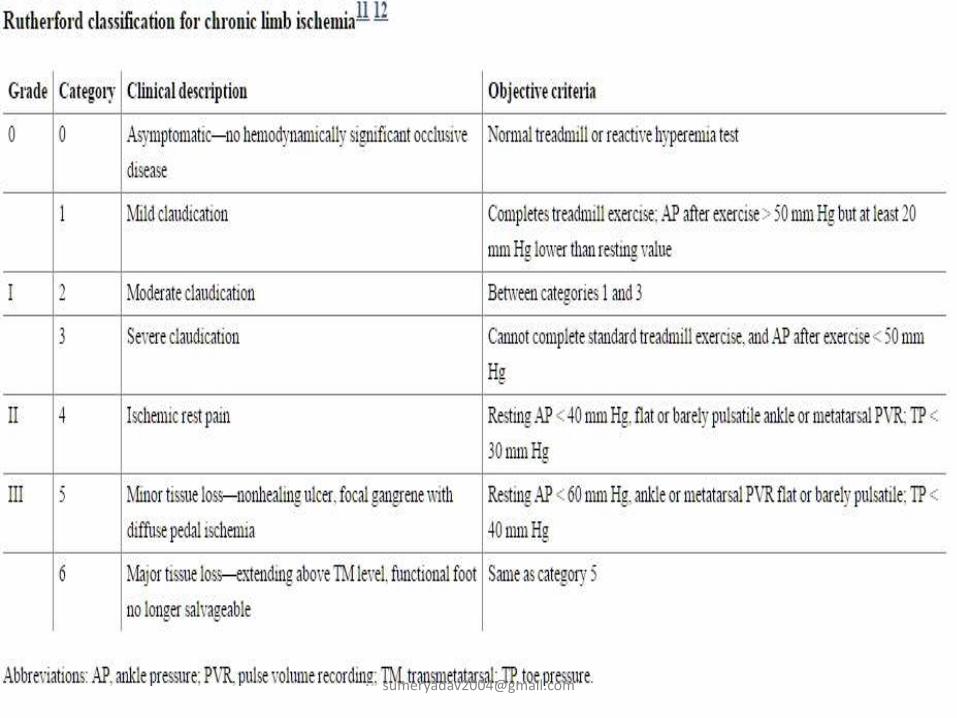
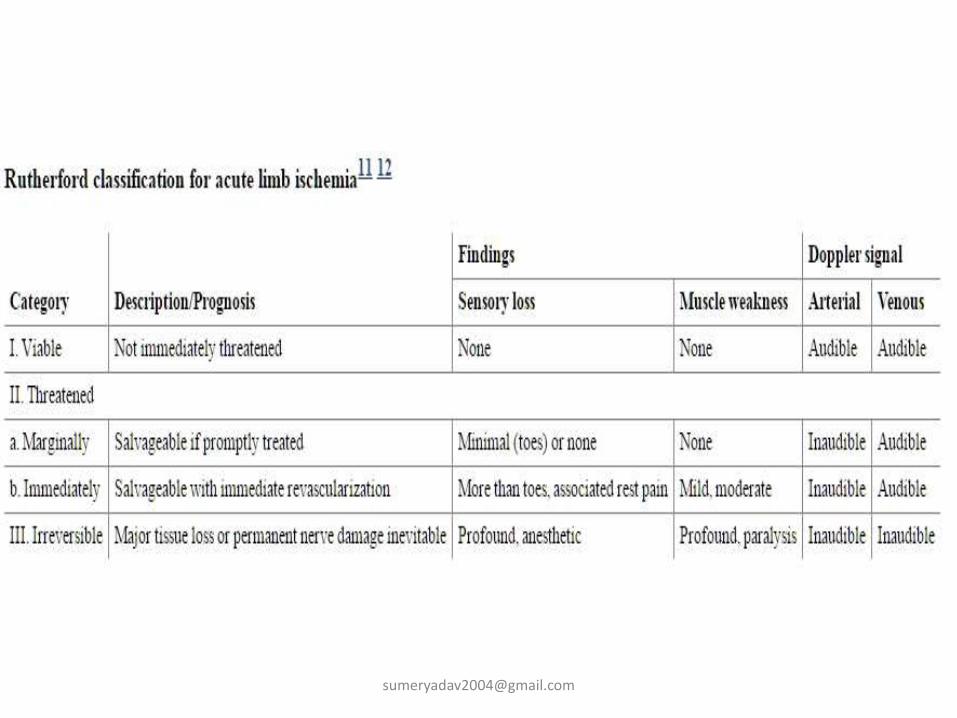
limb ischemia
Acute acute embolismtraumaaneurysm
ChronicatherosclerosisTAOCollagen vascular diseasediabetes
Features of lower limb arterial stenosisor occlusion
• Intermittent claudication• Rest pain• Cold, numb, paraesthesia, colour change• Ulceration• Gangrene• Decreased temperature• Sensation decreased• Movement diminished or lost• Arterial pulsation diminished or absent• Arterial bruit• Slow venous [email protected]
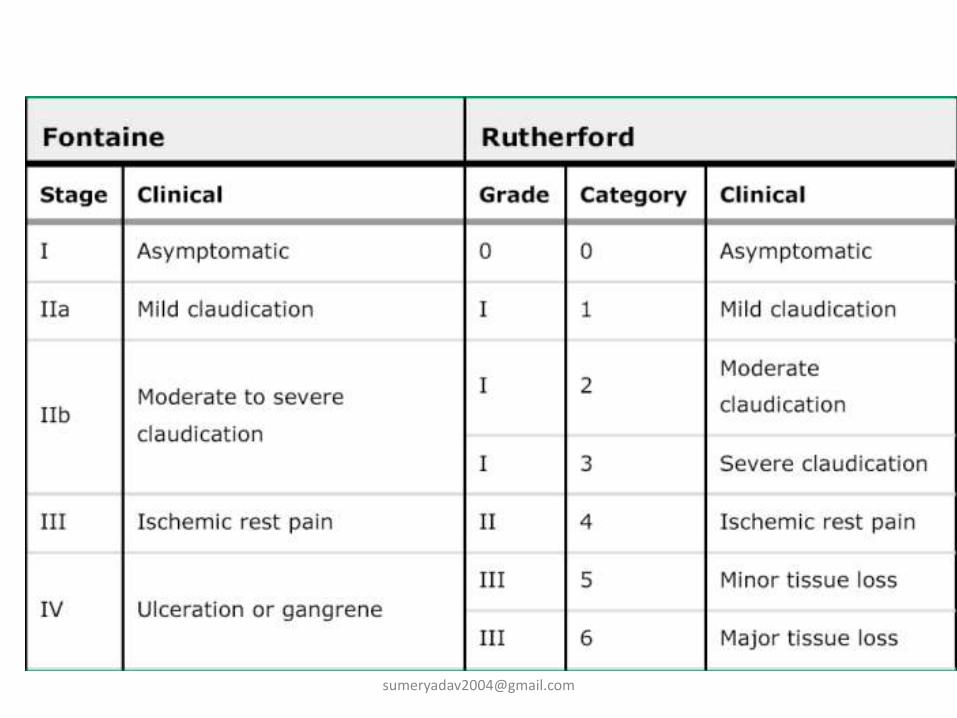
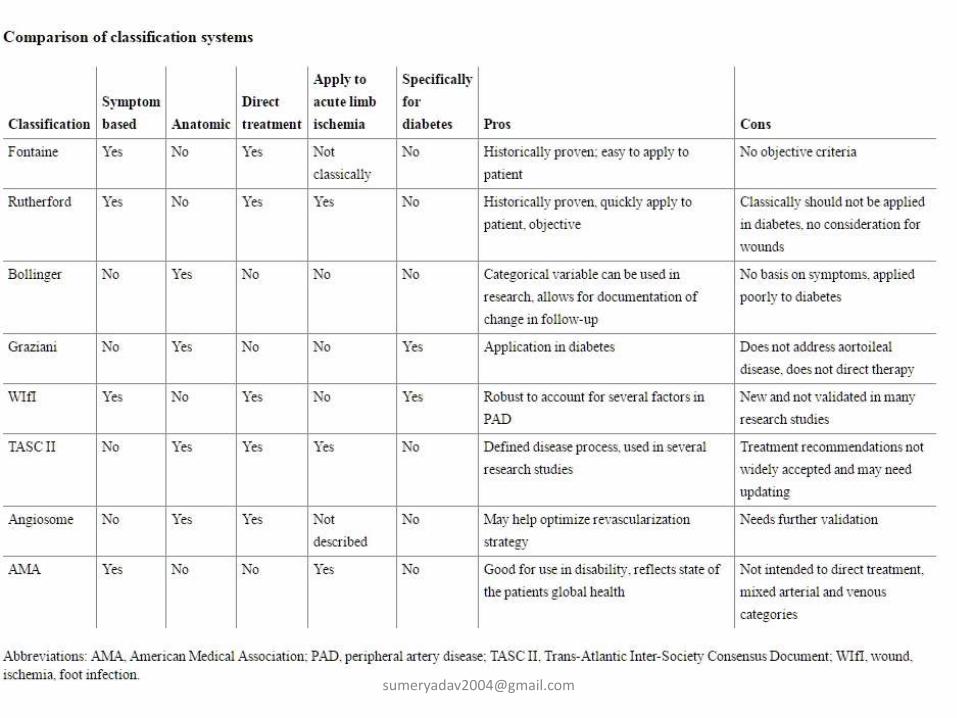
Fontaine classification
• Stage I Asymptomatic,
• Stage II - Mild claudication pain in limb
Stage IIA -Claudication at a distance > 200 m
Stage IIB -Claudication at a distance < 200 m
• Stage III - Rest pain, mostly in the feet
• Stage IV -Necrosis and/or gangrene of the limb
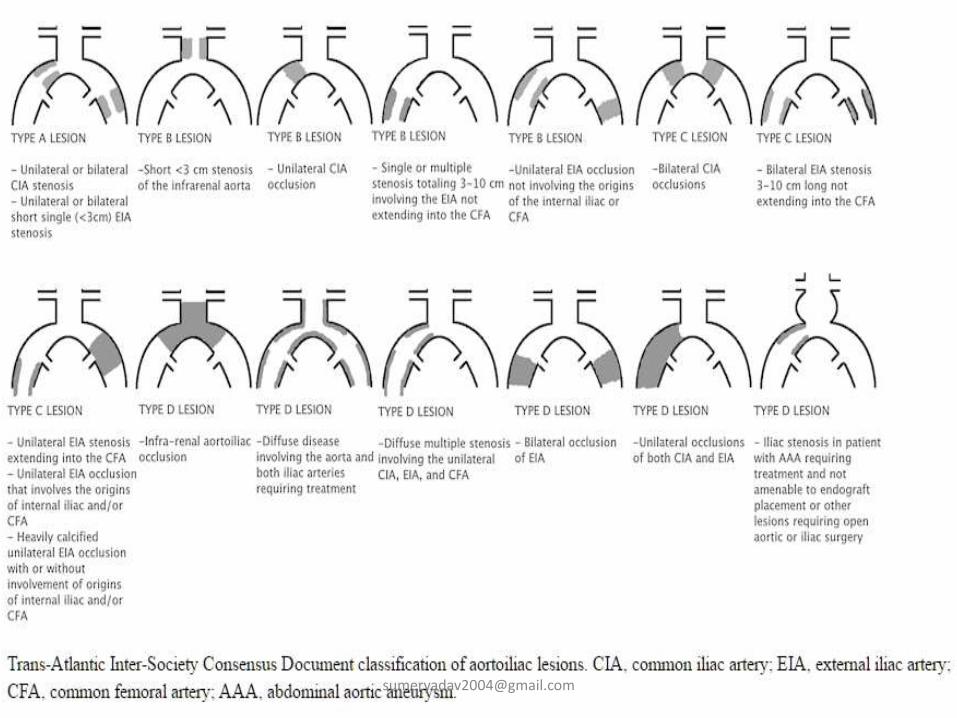
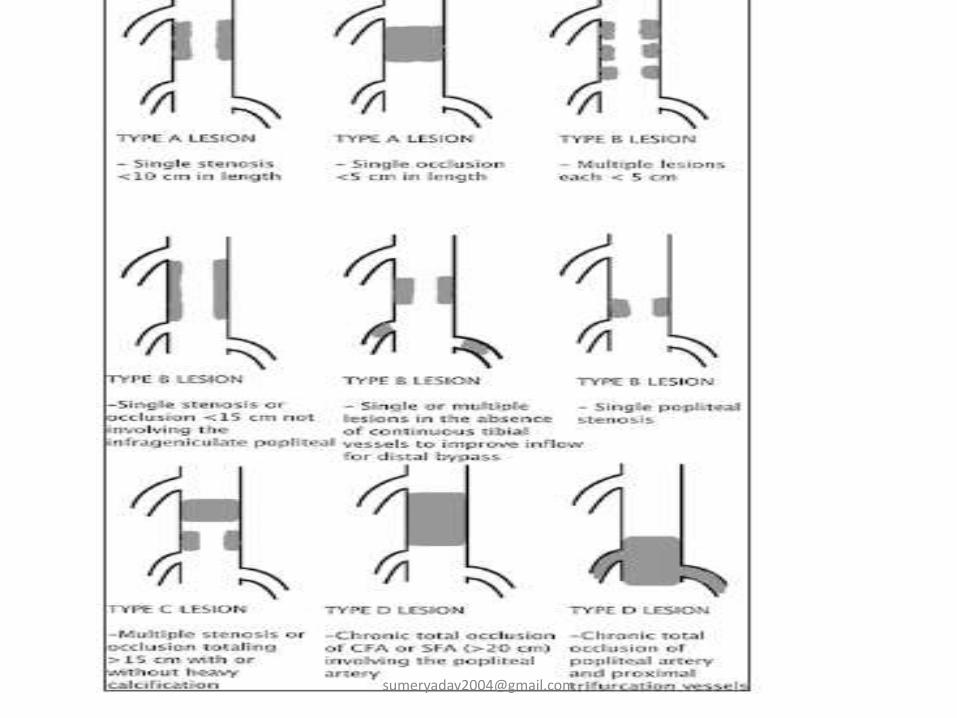
TASC 2
• TASC A - excellent results from endovascular management alone.
• TASC B - good results from endovascular management, and endoluminal interventions should be the first treatment approach.
• TASC C lesions - surgical management provides superior long-term results and endovascular techniques should be reserved for patients who are surgically high risk.
• TASC D lesions- should be treated by open surgery.
General investigation
• Tests relevant to diabetes, abnormal lipid metabolism, anaemia
• conditions causing high blood viscosity (e.g. polycythaemia and thrombocythaemia) include a full blood count (including platelets), plasma fibrinogen, blood and urine glucose, and a blood lipid profile (triglycerides, total cholesterol, and high- and low-density lipoprotein cholesterol).
• Cardiac failure, myocardial ischaemia, hypertension and age-related diseases such as chronic obstructive pulmonary disease and neoplasia – related to these
• ECG• echocardiography• chest radiograph• pulmonary function tests.• Tests for renal function (serum creatinine) required, especially if
contrast agents are to be used at [email protected]
Treadmill
• Patients themselves are poor at assessing claudicating distance and it might be thought that a treadmill assessment would provide a useful objective measurement of distance to onset of pain.
• a simple measured walk along a hospital corridor
is even more reliable.
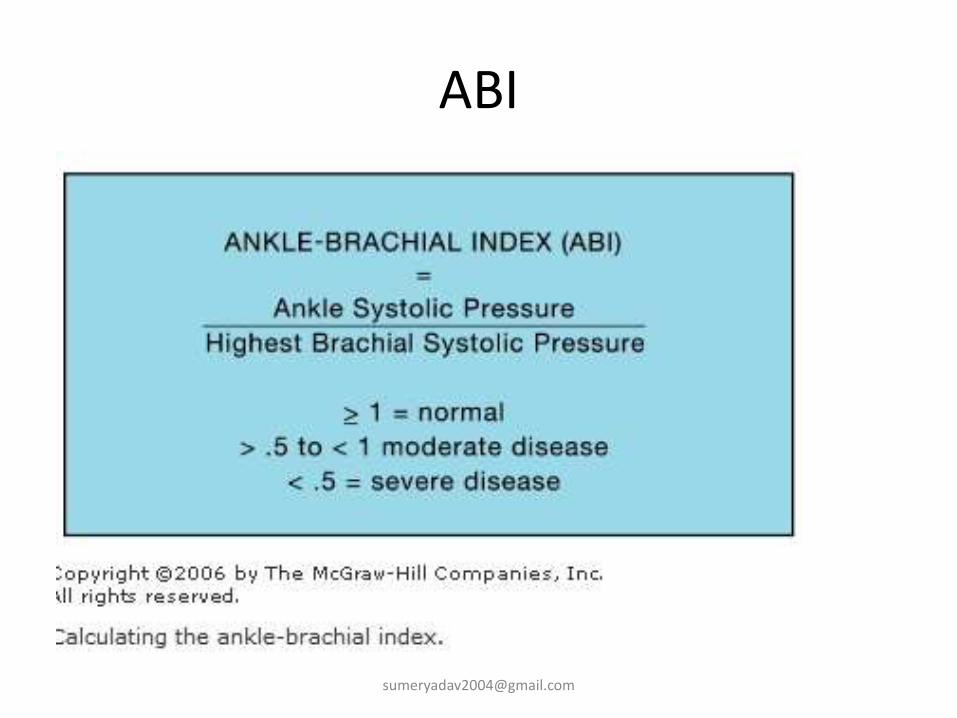
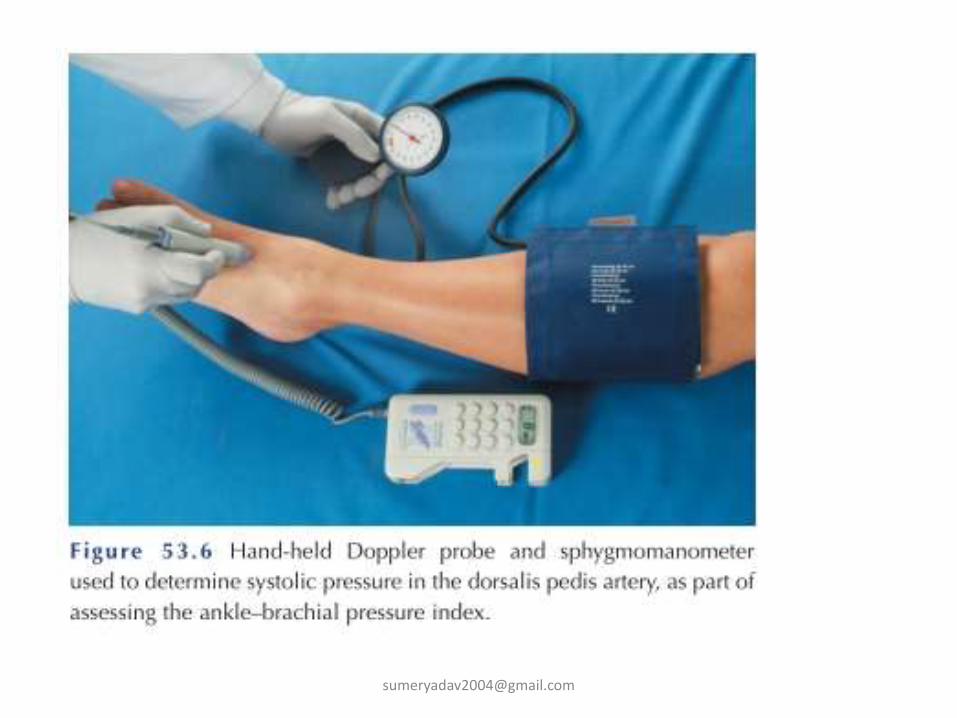
A good use for the treadmill (with a slight incline) is the detection of a fall in ABPI after exercise, indicating occult arterial stenosis
Tonoscillography
• one of the earliest methods used to investigate intermittent claudication.
• measuring the amplitude of the pressure wave in arteries at different levels in the leg.
• strain gauge plethysmography is still often used as a standard for measuring limb blood flow when new methods are being evaluated.
Plethysmography
• used in the assessment of limb blood flow
• Plethysmographic methods are by their nature quantitative, do not yield specific information about the sites of arterial occlusions
• tend to involve the use of cumbersome equipment which is not easy to use.
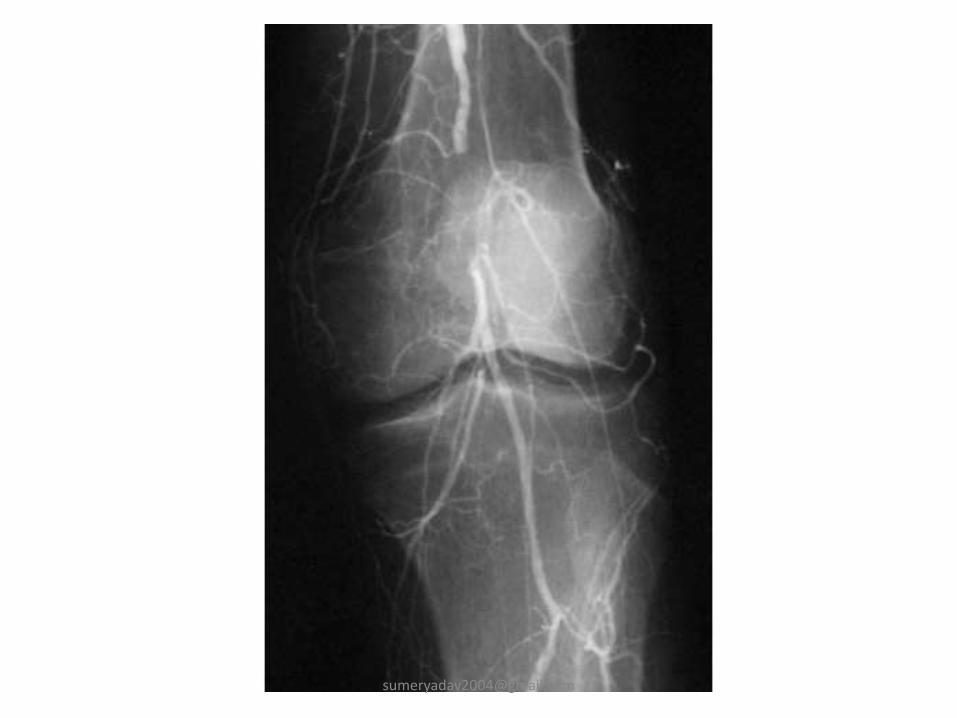
Arteriography
• The investigation of choice for the anatomical definition of peripheral vascular disease
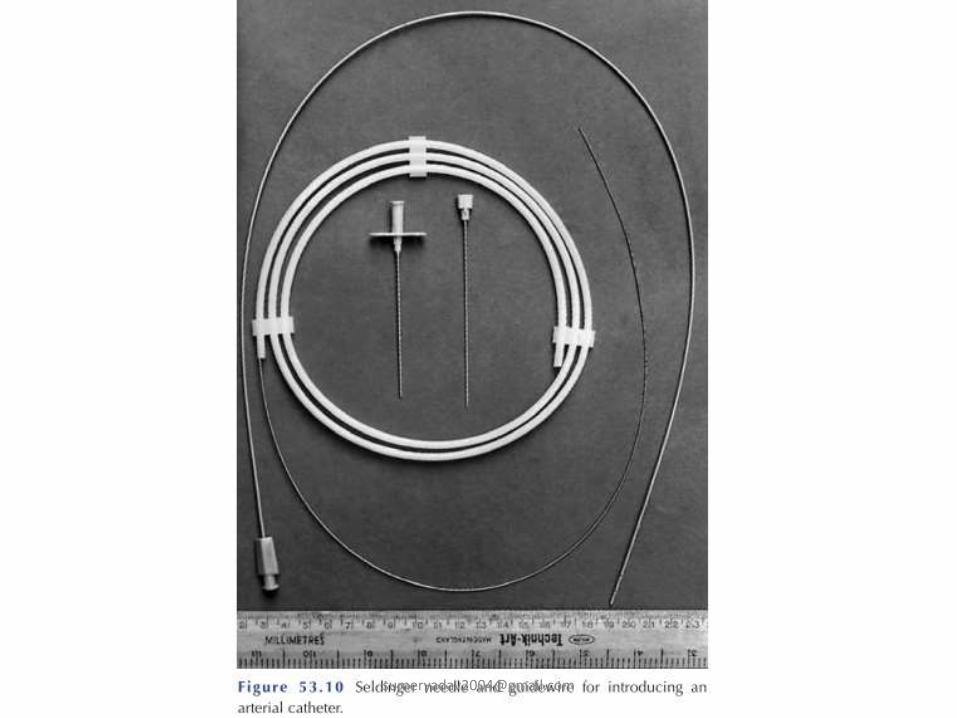
• Seldinger described his percutaneoustechnique for catheter placement. which is now universal.
• biplanar views solve the problem of superimposition
arteriography
• Sodium diatrizoate (Urografin, Hypaque)
• Sodium metrizoate (Triosil)
• On-table arteriography has an established place in the performance of femorodistalbypass.
Arteriography – seldingers technique• right femoral artery is most commonly accessed.• 18-gauge Seldinger needle. • Good pulsatile flow confirms arterial access. • wire is then inserted up into the aorta under fluoroscopic guidance. • After removing the needle, a catheter is inserted over the wire.• The catheter and wire can be steered to the target vascular bed • dye injected to opacify the vessels. • Contrast angiography provides a lumenogram, so thrombus-filled
aneurysms can be easily missed. • Digital subtraction angiography (where bony landmarks are
electronically removed) provides the best delineation of vascular pathology.
• Once the procedure is complete, the catheter is removed from the femoral artery and pressure applied.
• This technique forms the basis for all interventional procedures.
Complication• Hematoma • Occlusion • Pseudoaneurysm• arteriovenous fistula • Catheter-induced complications
Arterial dissectionSubintimal injection
• Cerebral arteriographyneurologic complicationPermanent neurologic complications
• Contrast reactions Major reactions Contrast-induced renal failure
Digital subtraction angiography
• The increased contrast detection and subtracting the preinjection ’mask’ image.
• The advantages of an intravenous injection
• decreased patient discomfort.
• However, problems persist. The quality of image is inferior to that produced by a conventional angiogram.
Ultrasound and Doppler flow meas-urement
• frequency of reflected ultrasound waves is dependent on the speed of flow of the blood from which the waves have been reflected.
• pulsed Doppler flow meter, allowed ’ultrasonic arteriography’ to become a reality. This is because it allows the depth from which the returning ultrasound waves are reflected to be measured.
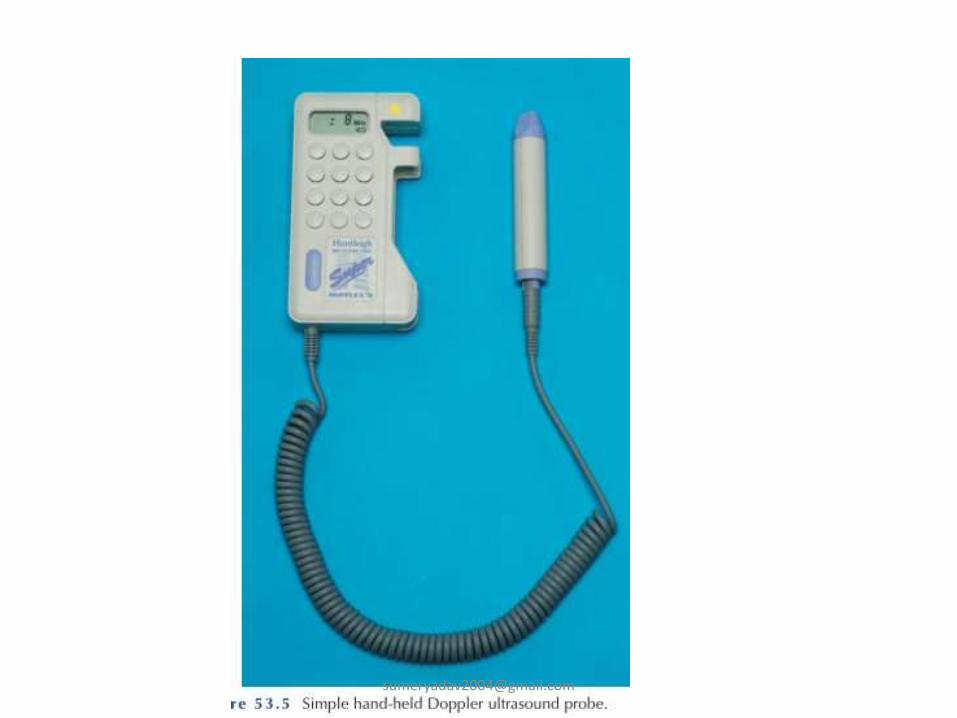
• The simplest use of Doppler ultrasound lies in the hand-held pencil probe used clinically for the detection of the presence or absence of flow in a vessel.
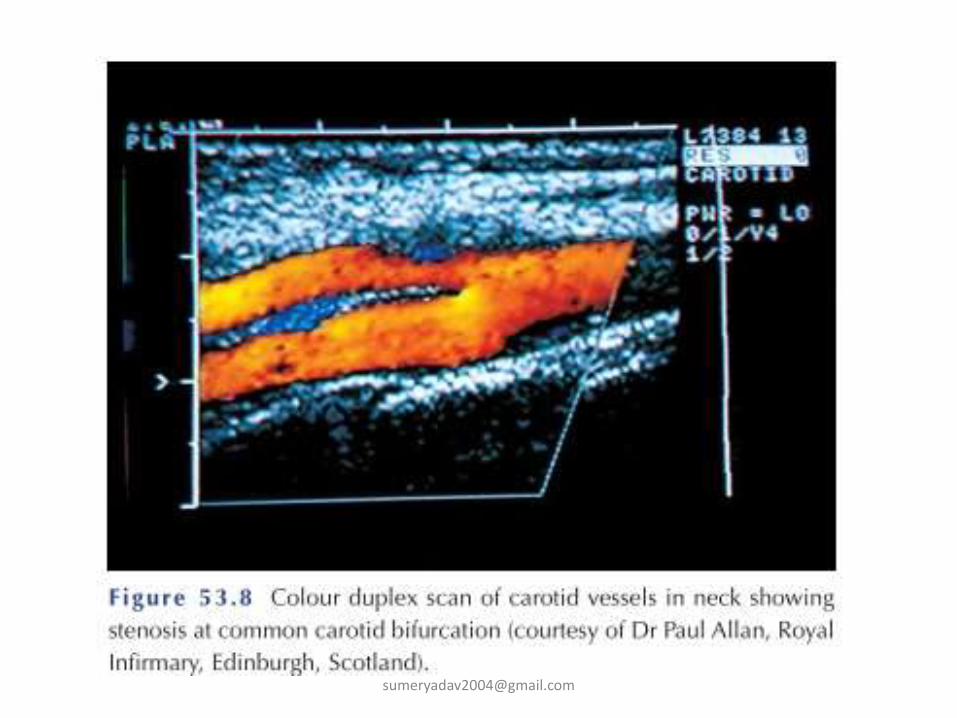
• Duplex scanning is a more recent innovation, combining real time ultrasonic imaging with Doppler flow measurements which have undergone sound spectrum analysis for visual display. It gives precise information about the functional significance of any arterial stenosesvisualized.
• The advent of Colour Duplex scanning, in which flow is represented on the real time image by a colour scale, has made the detection of local flow disturbances even easier.
DUPLEX SCAN
• create a gray-scale anatomic image, Doppler ultrasound B MODE/ 2D MODE (brightness)
• B MODE+ PULSE WAVE DOPPLER + COLOUR DOPPLER = ACTUALLY TRIPLEX = colour duplex scan
• permits measurement of peak systolic velocity and end-diastolic velocity
• Velocity therefore is proportional to the degree of narrowing of the vessel under investigation
• Although surgeons largely depend upon flow velocities in the arterial system, they rely even more on the anatomic appearance of the vessel when examining for thrombosis in the venous system. An occluded vein typically is larger than normal, not completely compressible, lacks respiratory variation, does not show flow augmentation with calf compression, and may have collateral flow.
portable scanners
• has led to the increased use of imaging in the vascular surgeon's office for diagnosis of
• pseudoaneurysms,
• mapping of veins for arteriovenous fistulas
• evaluation of patency of lower extremity bypass grafts.
• In the operating room, duplex scanning is helpful in image-guided venous access and completion ultrasound scanning
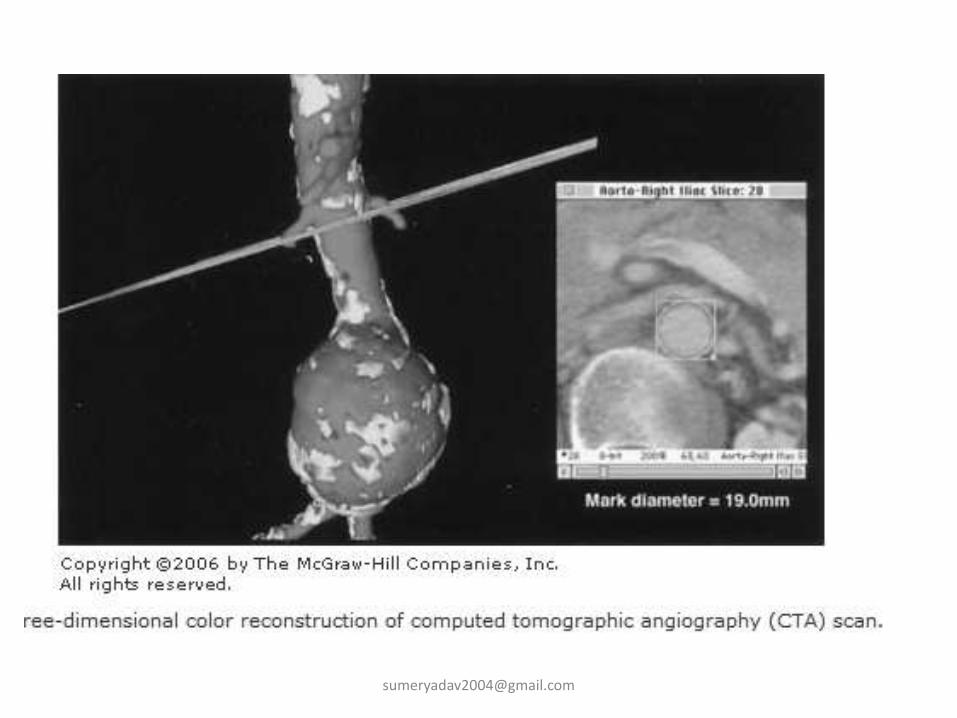
Computed Tomographic Angiography
• Noninvasive, • Contrast-dependent method for imaging the arterial
system.• The IODINATED contrast-filled vessels can be extracted
from the slices and rendered in three-dimensional format
• The extracted image can be rotated and viewed from several different directions.
• CTA is increasingly being used for imaging the carotid bifurcation, and as computing power increases, the speed of image acquisition and image resolution will continue to increase.
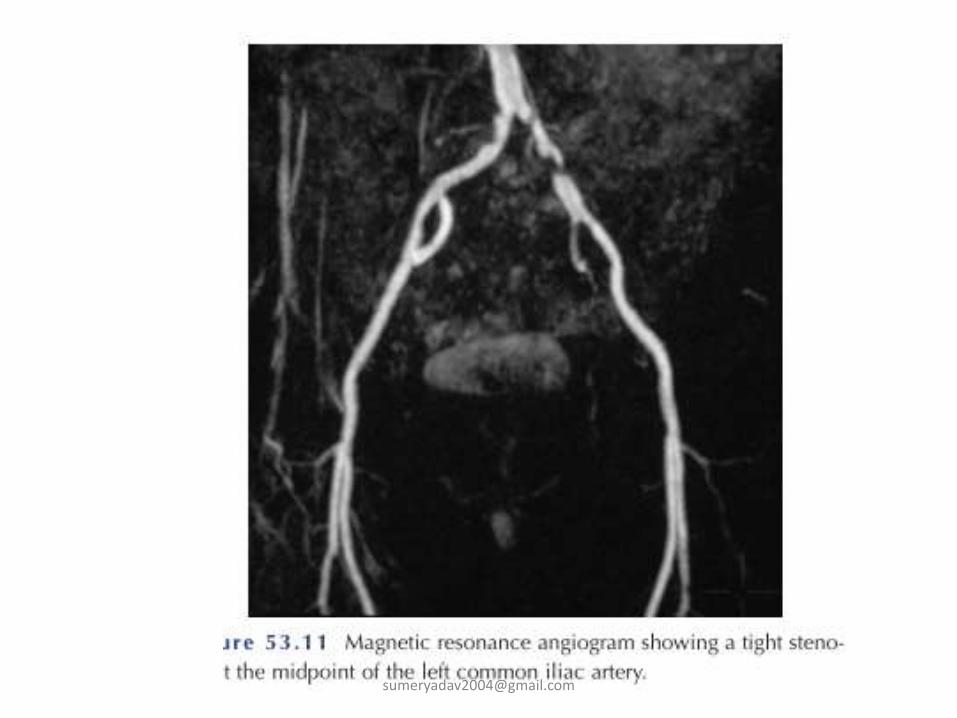
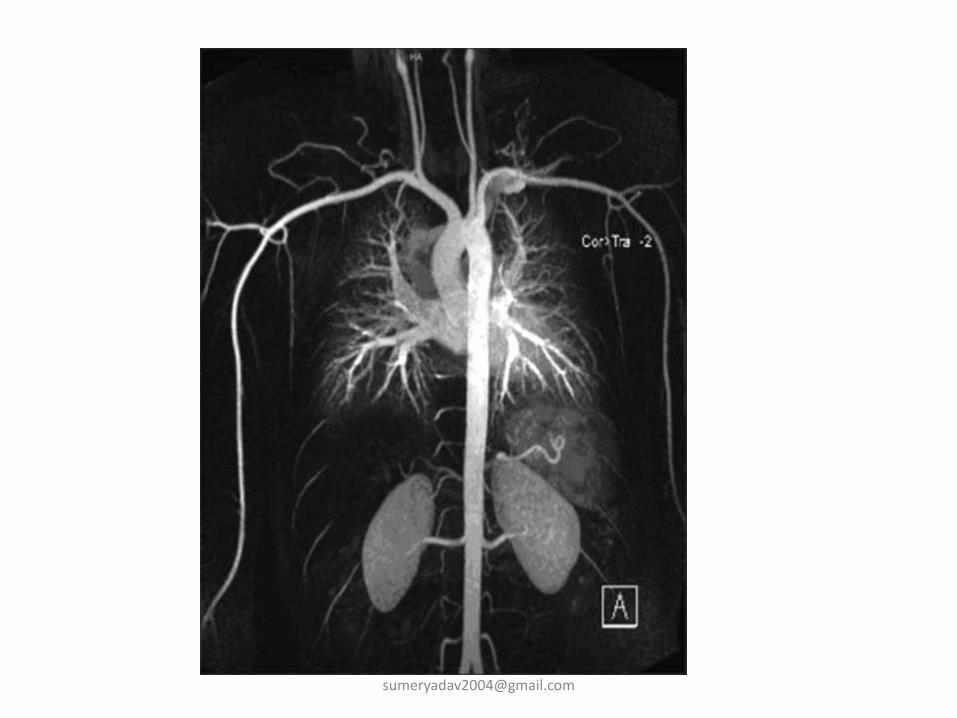
Magnetic Resonance Angiography
• MRA has the advantage of not requiring iodinated contrast agents to provide vessel opacification .
• Gadolinium is used as a contrast agent for MRA studies, and as it is generally not nephrotoxic, it can be used in patients with elevated creatinine.
• As with other MR tests, it is contraindicated in patients with pacemakers, severe claustrophobia, and most metallic foreign bodies.
• MRA tests are, however, relatively slow and very expensive.
• Like CTA, MRA is being increasingly used for imaging of the lower extremity vasculature, the carotid bifurcation, and the aorta and its branches.