Embed Size (px)
Citation preview

Chronic Granulomatous disease
Jintana Chataroopwijit10 Feb 2017
Content
• Introduction• Function of NADPH oxidase• Molecular genetic aspect• Clinical manifestation• Diagnosis and investigation• Treatment

Introduction
• First described in the 1950s• Disorder of phagocytic cells leading to
recurrent infections• Deficient superoxide (O2–) generation
via the phagocyte nicotinamide adenine dinucleotide phosphate (NADPH) oxidase system
• Incidence : 1/200,000–250,000 live births in USA and Europe
Clinical Immunology: Principles and practices 2008
Pediatr Allergy Immunol 2016: 27: 242–253.
Introduction
• Inherited in X-linked and autosomal recessive patterns
• Common organisms : catalase-positive bacteria and fungi
• Presentation : pneumonia, liver abscess, skin infections, lymphadenitis or osteomyelitis, bacteremia(uncommon)
Clinical Immunology: Principles and practices 2008
NADPH oxidase : function and disease
• NADPH oxidase : multicomponent enzyme complex containing both cytosolic and membrane-bound proteins
• To produce reactive oxygen species (ROS) in activated phagocytes (neutrophils, monocytes, and macrophages)
Pediatr Allergy Immunol 2016: 27: 242–253.

Schematic representation of the NADPH oxidase system. Chemoattractants interact with their receptors on the neutrophil surface, leading to an increase in intracellular calcium concentration. This activation results in the assembly
of the NADPH oxidase complex following phosphorylation of cytosolic factors. This is turn leads to superoxide production. DAG, diacylglycerol; PIP2, phosphatidylinositol bisphosphate; IP3, inositol triphosphate; α, β, γ, subunits of the GTP-
coupled receptors.Clinical Immunology: Principles and practices
2008
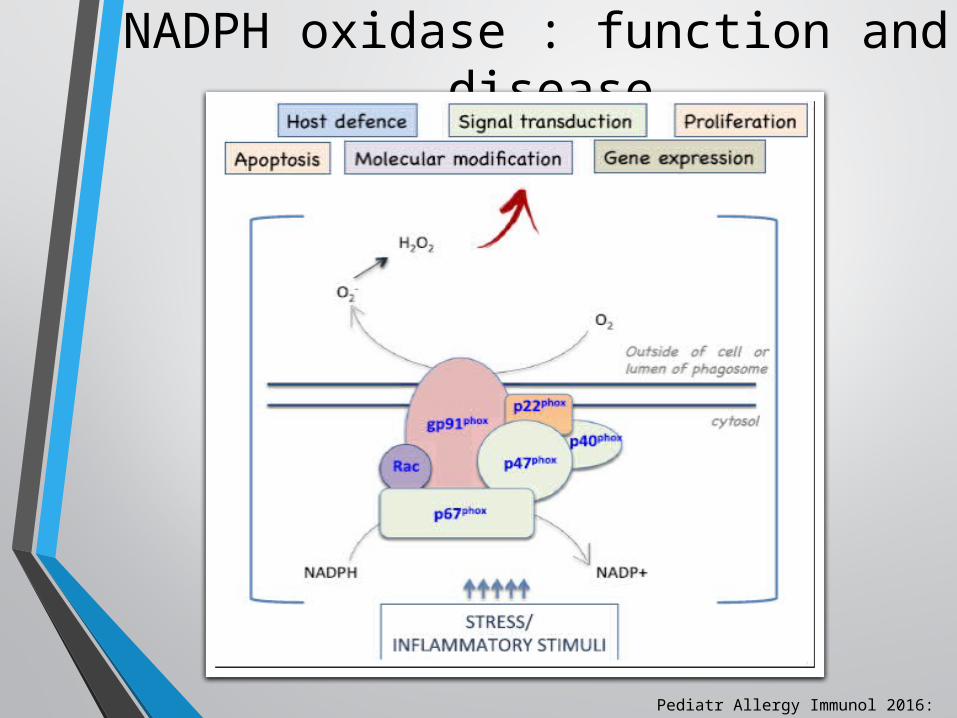
NADPH oxidase : function and disease
Pediatr Allergy Immunol 2016: 27: 242–253.

Phagocytosis and killing of microorganisms by phagocytic leukocytesBritish Medical Bulletin, 2016, 118:53–
66
NADPH oxidase : function and disease
• Catalytic core of phagocytic NADPH oxidase consists of flavo-cytochrome b558 (transmembrane protein) 1. Catalytic glycosylated gp91phox : cell
membrane was stabilized by p22phox2. Nonglycosylated p22phox
• Attachment of cytosolic components of the NADPH oxidase: p47phox, p67phox, p40phox, and GTPase-Rac
Pediatr Allergy Immunol 2016: 27: 242–253.

NADPH oxidase : function and disease
• During the phagocytic NADPH oxidase activation • phosphorylation of p47phox leads to
conformational changes --> allowing interaction with p22phox
• resultant membrane translocation of p47phox with the activation of GTPase-Rac assembles the other cytoplasmic subunits p40phox and p67phox to form the active oxidase complex
Pediatr Allergy Immunol 2016: 27: 242–253.
NADPH oxidase : function and disease
• Extracellular superoxide anions (O2 ) and hydrogen peroxide (H2O2) are produced in the phagolysosome (respiratory burst)
• ROS and proteins from granules mediate together the killing of microorganisms
Pediatr Allergy Immunol 2016: 27: 242–253.
NADPH oxidase : function and disease
• Underlying mechanisms of hyperinflammation• defective neutrophil apoptosis • skewed nuclear factor-kB signaling • upregulation of tumor necrosis factor alfa, interleukin
(IL)-17, IL-6, and granulocyte colony-stimulating factor • prolonged IL-8 messenger RNA activation• impaired activation of Nrf2 • decreased autophagy• increased inflammasome activation
Pediatr Allergy Immunol 2016: 27: 242–253.

Hyperinflammation
• Deficient autophagic antimicrobial defence --> excessive IL-1beta release
• Deficient regulation of autoreactive T cells
Brazilian Journal of Medical and Biological Research (2014) 47(11): 924-928,
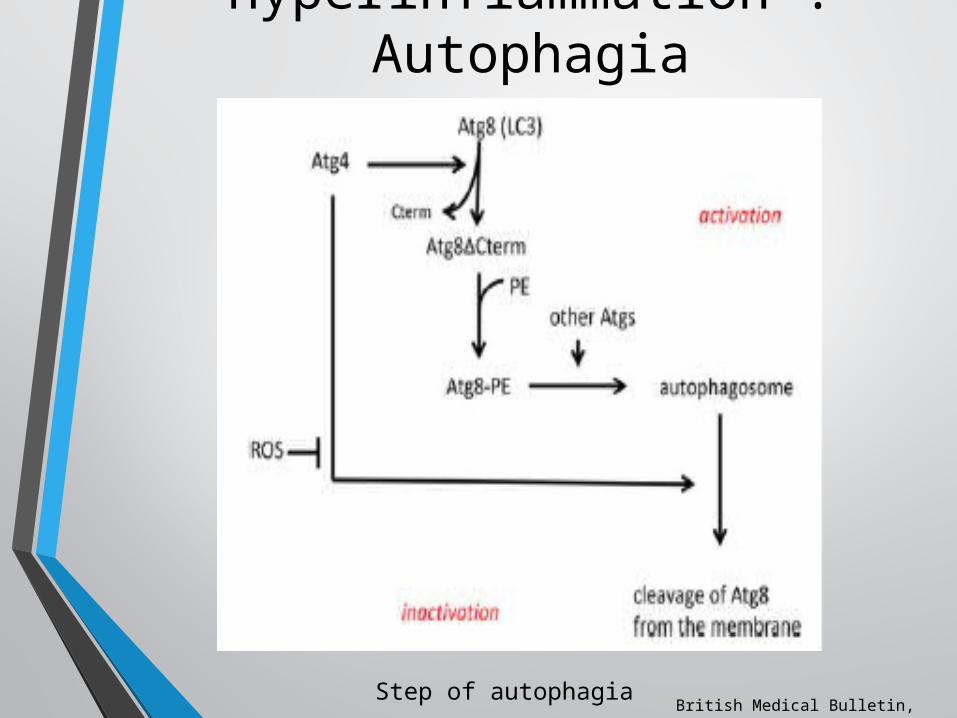
Hyperinflammation : Autophagia
British Medical Bulletin, 2016, 118:53–66
Step of autophagia

Hyperinflammation : Autophagia
British Medical Bulletin, 2016, 118:53–66
Reciprocal effects of autophagy on inflammasome activity

T cell activation
• Defect in regulation of T-lymphocyte activity• P47phox knock-out mice develop more severe
arthritis than wild type animals when challenge with collagen-specific T cells
British Medical Bulletin, 2016, 118:53–66
NADPH oxidase : function and disease
• Neutrophil extracellular traps (NETs) • externalized chromatin (DNA and histones)• cytosolic/granular proteins and may
• Bind bacteria and fungi and expose antimicrobial molecule --> control bacterial and fungal infection
• No direct link between ROS produced by NADPH oxidase and NET formation
Pediatr Allergy Immunol 2016: 27: 242–253.
Journal of infection 2014: 69:s32-s35
NADPH oxidase : function and disease
• Bustamante et al. : germline mutations in the gp91phox-encoding gene (CYBB) conferring the phenotype of X-linked recessive mendelian susceptibility to mycobacterial disease type 2 (XRMSMD) syndrome, but not XR-CGD
• XR-MSMD selectively affects the monocyte derived macrophages and B cells, but not monocytes or granulocytes
Pediatr Allergy Immunol 2016: 27: 242–253.

NADPH oxidase : function and disease
• May be some relation between the gp91phox protein and MSMD, indicating that the macrophage respiratory burst is involved in protection against mycobacterial infections
• Low levels of proinflammatory cytokines, particularly interferon gamma (INF-c), probably induce a defect in the IL-12/INF-c axis, which has a crucial role in protective immunity to mycobacteria
Pediatr Allergy Immunol 2016: 27: 242–253.
Molecular genetic aspects of CGD
• Reports from Europe, USA and Japan : XR-CGD most common form (60%)
• 30% of AR-CGD : p47phox deficiency
• 10% p22phox and p67phox deficiency (each about 5%)
• Iranian and Turkish cohorts : AR predominance (consanguineous marriages)
Pediatr Allergy Immunol 2016: 27: 242–253.
Molecular genetic aspects of CGD
• Mutations : small intragenic deletions/insertions, missense, non-sense, and splice-site mutations easily detected by sequencing
• Uncommon genetic mutation : large deletions and duplications (difficulty to detect multiple exon deletions/insertions with conventional methods )
Pediatr Allergy Immunol 2016: 27: 242–253.
Molecular genetic aspects of CGD
• Conventional methods : sequencing, PCR-SSCP, Southern blot
• Recently • Array Comparative Genomic Hybridization (array CGH) • Multiplex ligation dependent probe amplification
Pediatr Allergy Immunol 2016: 27: 242–253.

Molecular genetic aspects of CGD
• Stasia et al : 2 interesting cases of male XR-CGD• 5.7-kb duplication spanning exons 6 and 8 of CYBB gene • deletion of the same region
• Both mutations : probably caused by a single event of nonhomologous meiotic or mitotic crossing-over between two high-similarity short-tandem-gene therapy (GT) repeats of introns 5 and 8
Pediatr Allergy Immunol 2016: 27: 242–253.
X-linked CGD
• The most common : mutations in the gene encoding gp91phox (CYBB) at Xp21.1
• Mutation : frame shifts, nonsense mutations, missense mutations, splice region mutations, large and small deletions and regulatory region mutations
• Patients with large interstitial deletions, adjacent genes are affected —> McLeod syndrome, Duchenne muscular dystrophy, or X-linked retinitis pigmentosa
Clinical Immunology: Principles and practices 2008
X-linked CGD
• Clinical phenotype of McLeod syndrome • Compensated hemolysis• Acanthosis• Progressive neurodegenerative symptoms :
areflexia, dystonia and choreiform movements
• Absent erythrocyte Kx protein and diminished levels of Kell blood group antigens all X-linked CGD patients should be carefully screened for Kell blood groups
Clinical Immunology: Principles and practices 2008
Autosomal dominant CGD
• 35% of all cases
• 25% Mutations in gene for p47phox (NCF1, located at 7q11.23)
• 6% Mutations in the gene encoding p22phox (CYBA), located at 16q24
• <5% Mutation in the gene for p67phox (NCF2, located at 1q25)
Clinical Immunology: Principles and practices 2008
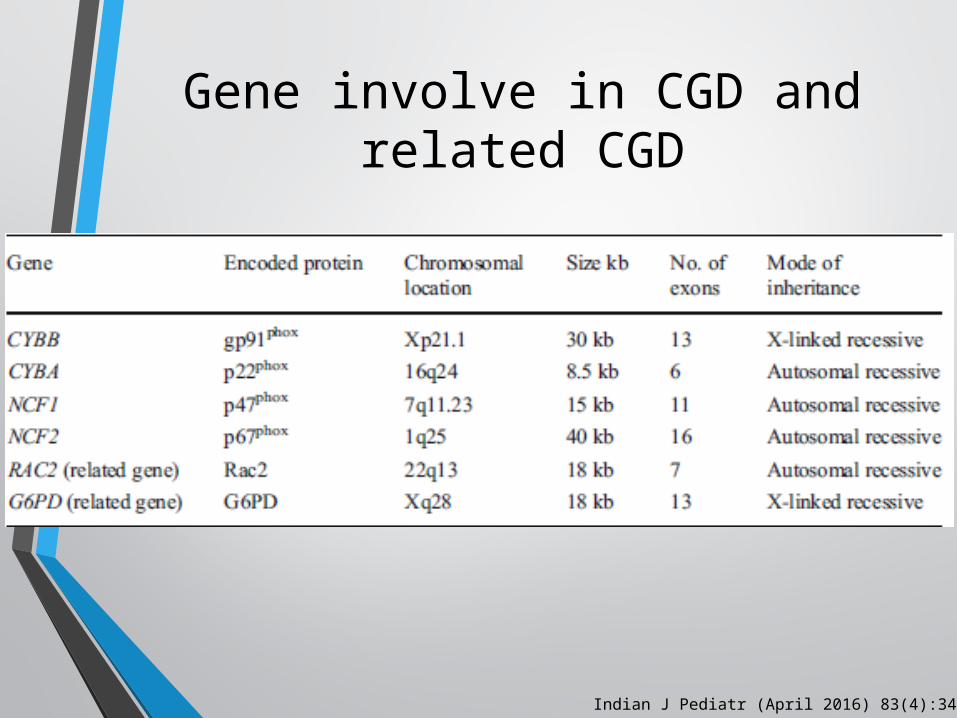
Gene involve in CGD and related CGD
Indian J Pediatr (April 2016) 83(4):345–353
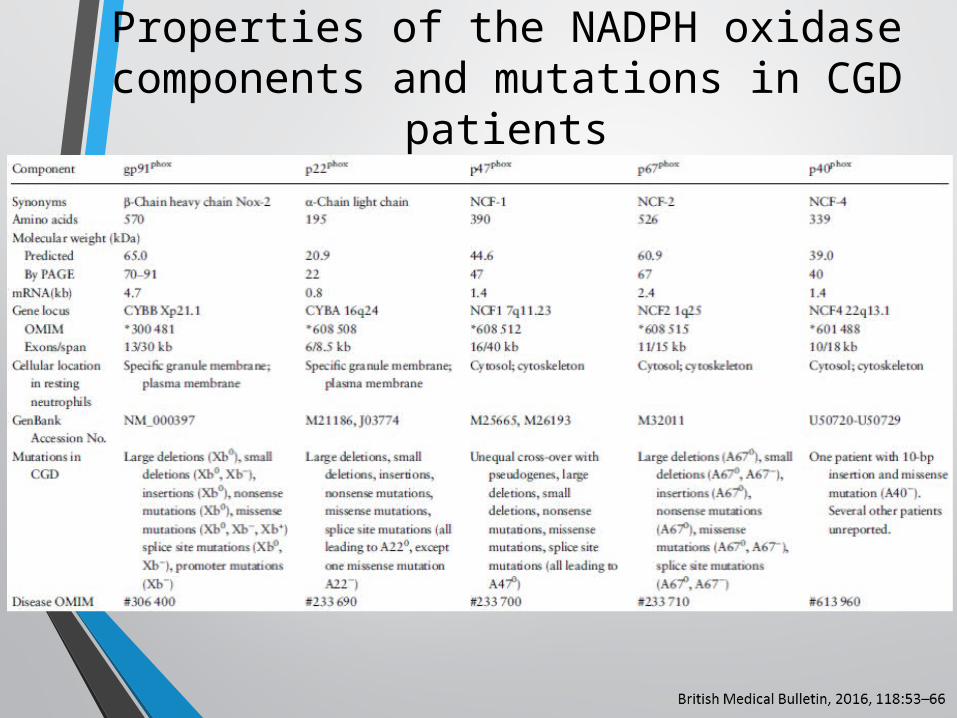
Properties of the NADPH oxidase components and mutations in CGD
patients

Carrier and genetic counseling
• Prenatal diagnosis : sequencing on fetus mutation
• Recently, preimplantation genetic diagnosis combined with HLA typing
Pediatr Allergy Immunol 2016: 27: 242–253.
Clinical manifestation
• Infection • Inflammatory complication
Pediatr Allergy Immunol 2016: 27: 242–253.

Clinical manifestation : infection
• Bacterial infection : catalase positive• Staphylococcus aereus• Burkholderia cepacia• Serratia marcescensu• Chromobacterium violaceum• Granulobacter bethesdensis
• Fungal infection : Aspergillosis• Tuberculosis and atypical mycobacterial
infection
Indian J Pediatr (April 2016) 83(4):345–353Clinical Immunology: Principles and practices
2008
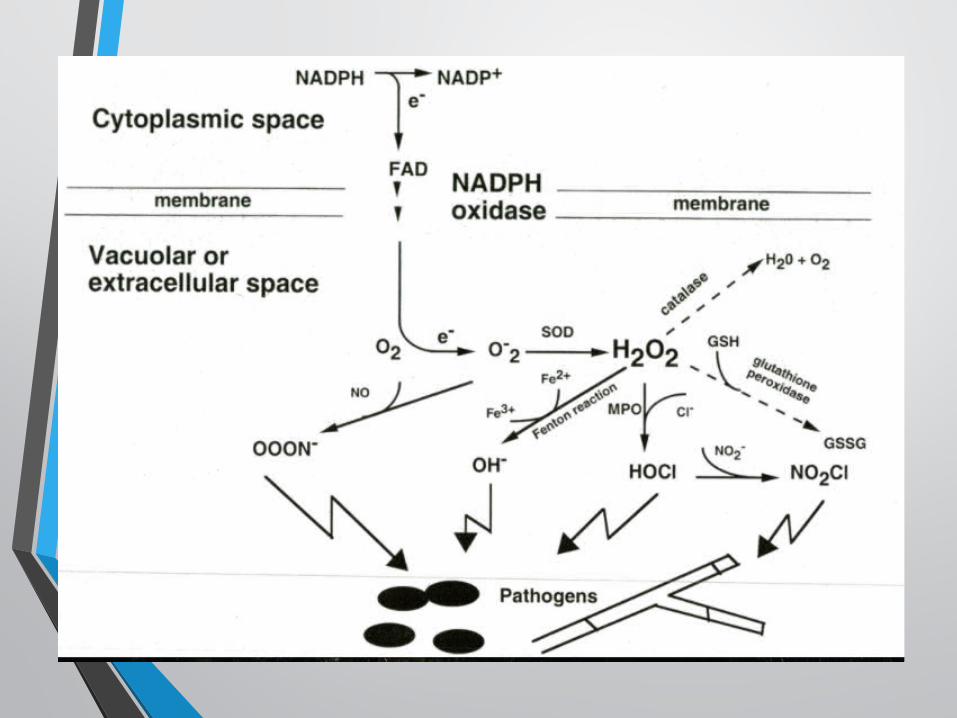
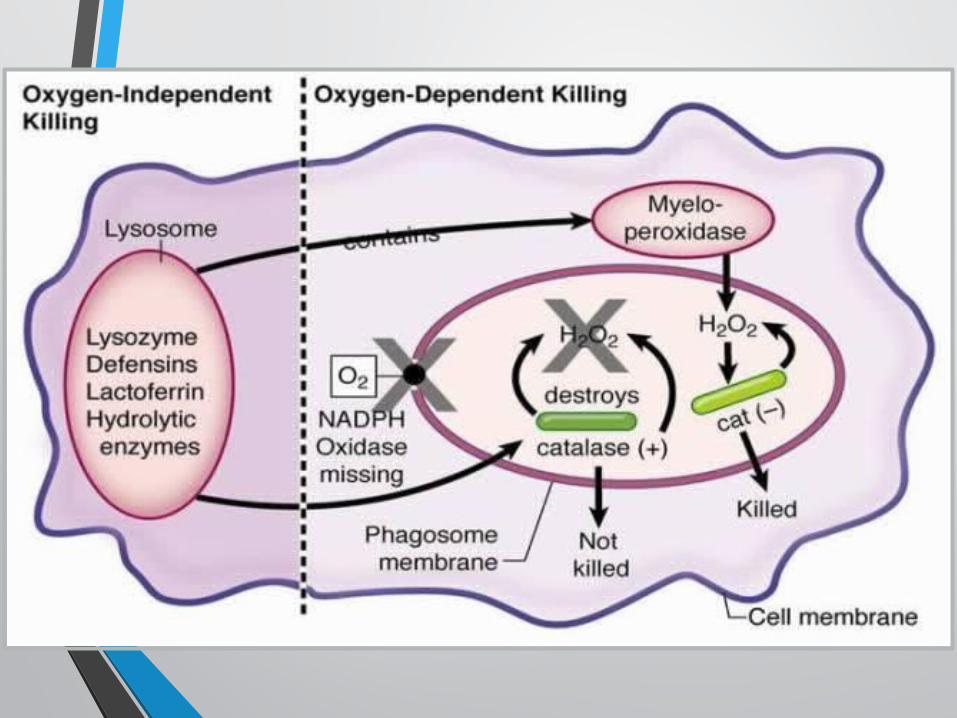

catalase positive organism and respiratory burst
• Bacteria can produce H₂O₂ by itself • H₂O₂ can then be converted in to HOCl by MPO arm to
kill catalase +ve organisms• NADPH oxidase & Myeloperoxidase function : get rid of
H2O2 which categorized under reactive oxidative species (ROS)
• Catalase degrades H2O2 into H2O and O2
Mechanism of respiratory burst
NADPH oxidase• O2 ----------------------> O2-( superoxide inoin)
Superixide dismutase(SOS) • O2- ---------------------------------> H2O2 (Hydrogen peroxide)
Myeloperoxidase• H2O2 -----------------------> HOCL (highly toxic to bacteria)
Clinical manifestation : fungal infection
• Aspergillus spp• A. fumigatus• A. flavus• A. niger• A. nidulans
• Norcardia spp.
Indian J Pediatr (April 2016) 83(4):345–35Clinical Immunology: Principles and practices
2008
• Site of infection• Pneumonia• Liver : abscess• Skin infections/abcess• Lymph node • Bone : osteomyelitis • Bacteremia : uncommon
Clinical manifestation : infection
Clinical Immunology: Principles and practices 2008

Clinical manifestationUSA
2000European
2009Indian
2014
Pneumonia 79% 66% 82%Lymphadinitis
Lymphadinitis 53% 50%
Cutaneous infection
52%Subcutaneous
abcess
53% 47%
GI involvement 48% 23%Hepatic abcess

Clinical manifestation : autoimmunity and inflammatory
complication
• Hyperinflammatory condition• Granulomas : obstruction• Colitis/enteritis : abdominal pain, diarrhea, rectal
bleeding• Non-infectious arthritis : Rheumatoid arthritis• Other autoimmune disease
Indian J Pediatr (April 2016) 83(4):345–35British Medical Bulletin, 2016, 118:53–66
Clinical manifestation : autoimmunity and inflammatory
complication• Other autoimmune disease
• Discoid lupus• SLE• Dermatomyositis• Sacroiliitis• Idiopathic thrombocytopenia• Autoimmune hepatitis
• Hemophagocytic lymphohistiocytosis (HLH) : Burkholderia cepasia and Leishmania
Indian J Pediatr (April 2016) 83(4):345–35British Medical Bulletin, 2016, 118:53–66
Diagnosis
• History of severe infection• Absence of respiratory burst• Inability of neutrophils to reduce nitroblue
tetrazolium dye or to oxidize dihydrorhodamine
Clinical Immunology: Principles and practices 2008
NBT Reduction Test• In 1967, Baehner and Nathan : leukocytes in patients
with CGD failed to reduce NBT dye due to defective oxidase --> unable to utilize oxygen and produce reactive species
• NBT : yellow dye ----- > blue formazan
• CGD patients fail to reduce NBT : remain yellow
• X-linked carriers : demonstrate both colors (two populations of cells) are present
Indian J Pediatr (April 2016) 83(4):345–353
Reduction

NBT reduction test
Clinical Immunology: Principles and practices 2008
Dihydrorhodamine (DHR) Test
• Neutrophils are stimulated with Phorbol-12-Myristate-13 Acetate (PMA) to produce reactive oxygen species such as hydrogen peroxide
superoxide• Dihydrorhodamine ———————-> rhodamine 123
• Change in fluorescence intensity : flow cytometer
Indian J Pediatr (April 2016) 83(4):345–353
• Reliable diagnosis : cases and carriers of X-linked• Carriers of autosomal recessive forms of CGD cannot be
detected by DHR as one normal allele is sufficient for adequate function
• Expression of protein subunits of NADPH oxidase on neutrophils can be studied by flow cytometry : classifying the type of CGD
• Accepted worldwide as the screening test of choice for CGD
Indian J Pediatr (April 2016) 83(4):345–353
Dihydrorhodamine (DHR) Test

Dihydrorhodamine (DHR) Testhistogram, stimulation index
Indian J Pediatr (April 2016) 83(4):345–353X : fluorescence intensity
Y : number of cell

Treatment
Pediatr Allergy Immunol 2016: 27: 242–253.

Curative treatment
• Hematopoietic stem cell transplantation• Gene therapy
Indian J Pediatr (April 2016) 83(4):345–353
Hematopoietic stem cell transplantation
• First bone marrow transplant was performed in CGD in 1973• Since the beginning of the 21st century : HSCT can cure CGD
and reverse organ dysfunction
• Keypoint 1)Age and indication : NADPH oxidase activity 2)Kind of donor to select3)Conditioning regimen : myeloablative conditioning, reduced-
intensity conditioning regimens
Indian J Pediatr (April 2016) 83(4):345–353
Hematopoietic stem cell transplantation
• Indication• one or more life-threatening infections• non-compliance with antimicrobial prophylaxis• steroid-dependent autoinflammation• In adolescensce: no organ dysfunction
Indian J Pediatr (April 2016) 83(4):345–353

• In 2014, Gungor et al. • Large prospective multicenter study : 56 patients, aged 0–
40 years (median age: 13 years)• 42/56 high risk patients, not be candidates for
myeloablative HSCT• Using a reduced conditioning protocol• Results : 2-year overall survival of 96% and event-free
survival of 91%• The cumulative incidence
• severe acute GVHD grades III–IV : 4% • chronic GVHD was 7%
• Stable myeloid donor chimerism was found in 93% of surviving patients
• 2 adult patients able to have children : preserve fertility
Pediatr Allergy Immunol 2016: 27: 242–253.
Hematopoietic stem cell transplantation

• Best donors : matched sibling bone marrow (MSD) but low incidence
• Other : perfectly HLA-matched unrelated donors (MUD) are almost comparable with those using HLA-MSDs
• Umbilical cord blood could be an option for these patients but available results concerning CGD patients are limited
• At present : all patients with XR-CGD or AR-CGD with no residual oxidase activity should be offered HSCT as early as possible, with either an MSD or MUD
Pediatr Allergy Immunol 2016: 27: 242–253.
Hematopoietic stem cell transplantation
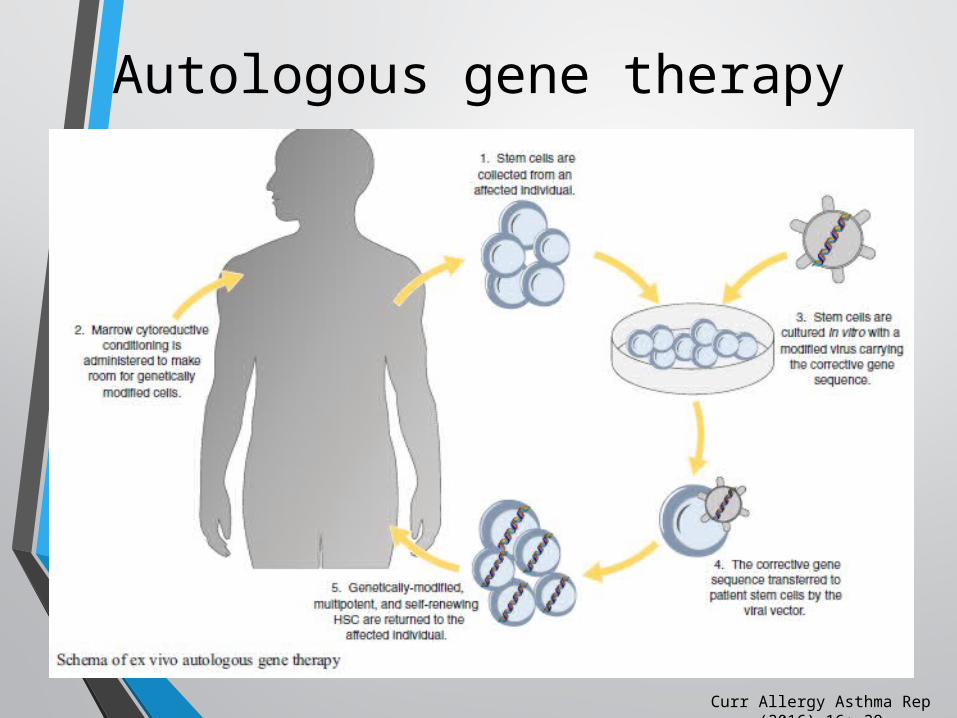
Autologous gene therapy
Curr Allergy Asthma Rep (2016) 16: 39
Gene Therapy for X-Linked Chronic Granulomatous Disease (X-CGD)
• First clinical trial : National Institutes of Health and Indiana University
• Gamma retroviral vectors to deliver normal human gp91phox
• No severe adverse events and gene-marked cells were detectable at low levels for months after treatment
• Superoxide levels were not sufficient to produce significant clinical improvement
Curr Allergy Asthma Rep (2016) 16: 39

Gene Therapy for X-Linked Chronic Granulomatous Disease (X-CGD)
• Three patients were treated at the NIH using reduced intensity conditioning prior to infusion of gp91phox vector-treated HSCs
• Functionally corrected cells dropped from 24 to 1.1 % at 34 months post therapy
• Resolution of infections at this low level of transgene expression
• Small amount of normal superoxide production may have protective clinical outcomes
• Levels were 0.03 % in a second patient who had partial control of infections at 11 months follow-up and undetectable in the third who died of invasive fungal infection 6 months post treatment
Curr Allergy Asthma Rep (2016) 16: 39
Gene Therapy for X-Linked Chronic Granulomatous Disease
(X-CGD)
• 9 X-CGD patients (Frankfurt, Zurich, London, and Seoul)with similar gamma-retroviral vectors and reduced intensity conditioning
• Clinical benefit in all of these patients• Over expression of EVI1 led to the development of
myelodysplasia with monosomy seven in two patients• Gradual loss of functional gene-marked cells at around 8
months after gene therapy due to epigenetic inactivation of the retroviral promoter with no leukemogenic events, there was also no significant engraftment after 3 months post gene therapy
Curr Allergy Asthma Rep (2016) 16: 39

Gene Therapy for X-Linked Chronic Granulomatous Disease
(X-CGD)
• Two parallel gene therapy trials in Europe and the USA based on these rationales with safer lentiviral vectors
• 1 child with significant disease burden (invasive liver, brain, abdominal, and pulmonary infections, and inflammatory complications) treated in Europe
• He was stable until around 3 months post gene therapy, but then died from respiratory complicationsdue to pre-existing conditions
• The US trial is currently open and is anticipating treatment of the first patient by the end of 2015
Curr Allergy Asthma Rep (2016) 16: 39
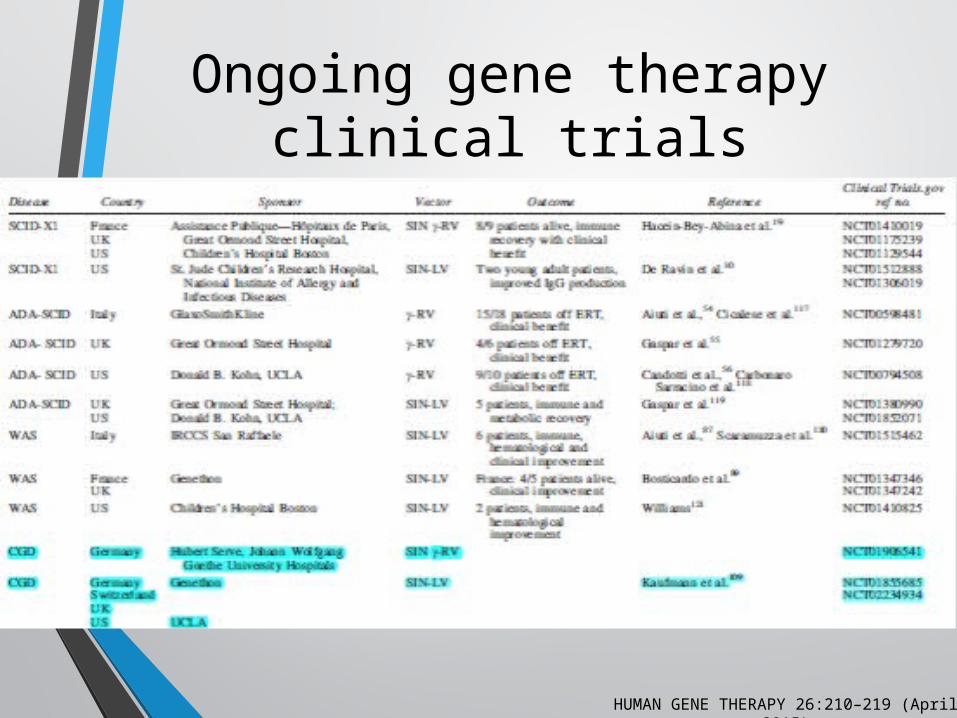
Ongoing gene therapy clinical trials
HUMAN GENE THERAPY 26:210–219 (April 2015)

Gene therapy
Curr Allergy Asthma Rep (2016) 16: 39
Gene therapy
• Several researchers are involved in gene therapy trials in CGD world over and this is an active field of research
• Therapy in CGD patients as genes involved in NADPH oxidase are metabolic genes and are not involved in cellular proliferation
• At present, gene therapy continues to be in an experimental phase
Indian J Pediatr (April 2016) 83(4):345–353
Survival rate : from past to present
• Change over last two decades : 90% reaching well into adult
• Better recognition, improvement of awareness, effectiveness of antimicrobial and HSC transplantation
• Major cause of morbidity and mortality : Infection• Median age of the patientBefore 1991 : 15.53 years2001 : 20.17 years2012 :28.12 years
Pediatr Allergy Immunol 2016: 27: 242–253.
THANK YOU







![Skin Inflammation, [Acute, Suppurative, Chronic, Chronic ... · Skin – Inflammation, [Acute, Suppurative, Chronic, Chronic Active, Granulomatous] presence of mononuclear cells (lymphocytes,](https://img.pdfslide.us/doc/110x75/5f0eb0c97e708231d44075f1/skin-inflammation-acute-suppurative-chronic-chronic-skin-a-inflammation.jpg)