Embed Size (px)
Citation preview

CHILDHOOD GAUCOMA
DR. BYRON Y. LARGADO

DEFINITIONS AND CLASSIFICATIONS
Primary congenital/ infantile glaucomaBirth or w/in first few weeks of lifeAbnormalities in the anterior chamber angle
development that obstruct aqueous outflow in the absence of systemic anomalies or other ocular malformation
Secondary infantile glaucomaAssociated with inflammatory, neoplastic,
hamartomatous, metabolic or other congenital abnormalities

DEFINITIONS AND CLASSIFICATIONS
Primary Juvenile glaucomaRecognized early in childhood (after 3 yrs of age) or
early in adulthoodDevelopmental glaucomas
Embraces both primary congenital and secondary glaucoma associated with other developmental anomalies, either ocular or systemic
Appear when the onset of elevated IOP occurs before the age of 3 in primary congenital glaucoma or in pediatric glaucomas associated with other ocular and/or systemic abnormalities

EPIDEMIOLOGY AND GENETICS
Heterogenous in the pediatric age groupPrimary congenital glaucoma –
50-70-% of the congenital glaucomasOccurs less frequent than primary adult glaucomaRare – 1:10,000 births
Of pediatric glaucoma cases60% - diagnosed by the age of 6 mos80% within the 1st year of life65% approximately are male70%- involvement is bilateral

EPIDEMIOLOGY AND GENETICS
Some pedigrees suggest autosomal dominant but more patient shows recessive pattern with incomplete or variable penetrance and possibly multifactorial inheritance
3 major loci of recessively inherited primary congenital galucoma GLC3A - on chromosome 2 (2p21), GLC3B -on chromosome 1 (1p36) GLC3C – on chromosome 14
(14q24.3)
0 Genetic counselling- for parents of child w/ pediatric glaucoma & adults w/ childhood onset glaucoma

PATHOPHYSIOLOGY
2 MAIN GROUPS (THEORIES OF PATHOGENESIS) Cellular or membrane
abnormality in trabecular meshwork is the primary pathologic mechanismEither anomalous
impermeable TM or a Barkan membrane covering the trabecular meshwork
Anterior Segment anomaly Abnormal insertion of
ciliary muscle
Exact mechanism of primary congenital glaucoma remains unproven
Developmental arrest in the late embryonic period suggested

CLINICAL FEATURES AND EXAMINATION
PRIMARY CONGENITAL GLAUCOMAPresents Classic triad in newborn
EpiphoraPhotophobiaBlepharospasm
DiagnosisIOP, corneal diameter and axial length, gonioscopy and
ophthalmoscopyOptic nerve photography for future follow up

CLINICAL FEATURES AND EXAMINATION
Manifestations:Buphthalmos with
corneal enlargement ⦣12 mm in diameter during first year of life
Corneal edemaMild haze to dense
opacification of corneal stroma
Haab striae

CLINICAL FEATURES AND EXAMINATION
Manifestations (Continuation):Reduced visual acuity
As a result of:Optic atrophy Corneal cloudingAstigmatismAmblyopiaCataractLens dislocationRetinal detachment

CLINICAL FEATURES AND EXAMINATION
Manifestations (Continuation):Clinicians successfully measure IOP of an infant younger
than 6 mos. while feeding or immediately after (w/o sedation or anethesia)
Infants require anesthesiaSeveral implications of anesthesia
Lowers IOP – exception is Ketamine which increases IOPdehydration- which lowers also IOPNormal IOP of infants under anesthesia ranges from 10-15
mmHg

CLINICAL FEATURES AND EXAMINATION
Gonioscopy under anesthesia is recommended In primary childhood glaucoma
The anterior chamber is characteristically deep with a normal appearance to the iris
High and flat iris insertion Absence of angle recess Peripheral iris hypoplasia Tenting of the peripheral iris pigment epithelium Thickened uveal trabecular meshwork

CLINICAL FEATURES AND EXAMINATION
Corneal edema Visualization of the optic disc is part of routine
examination : direct and indirect ophthalmoscopy as well as photograph of the disc The optic nerve head of an infant without glaucoma is
pink with a small physiologic cup With glaucoma: enlargement of the cup caused by high
IOP

DIFFERENTIAL DIAGNOSIS Excessive tearing- obstruction
of the lacrimal drainage system Enlarged corneas: X-linked
congenital megalocornea w/o glaucoma, exophthalmos; shallow orbits
Tears in Descemet’s membrane resulting from birth trauma – associated with forceps-assisted deliveries
Optic nerve abnormalities: Coloboma, hypoplasia,
malformation, physiologic cupping
Corneal opacification and clouding: Birth trauma Dysgeneses (Peter’s anomaly
and sclerocornea) Dystrophies Choristomas Intrauterine inflammation Inborn errors of metabolism keratomalacia Keratitis

LONG-TERM PROGNOSIS AND FOLLOW-UP
The initial procedure of choice is goniotomy or
trabeculotomy if the cornea is clear
Trabeculotomy ab externo if the cornea is hazy
Trabeculectomy or shunt procedures – for failed goniotomy and trabeculotomy
Cyclophotocoagulation- in intractable cases

Medical management: ᵦ-adrenergic antagonists or
carbonic anhydrase inhibitors (CAI) – may be used prior to surgery to control IOP and help clear a cloudy cornea

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED OCULAR ANOMALIES
ASSOCIATED OCULAR ANOMALIES microphthalmos Corneal anomalies (microcornea, megalocornea) Anterior segment dysgenesis (Axenfeld-Rieger
syndrome, Peters anomaly, iridoschisis) Aniridia Lens anomalies (congenital cataracts, lens
dislocation) Persistent fetal vasculature (persistent hyperplastic
primary vitreous) Congenital ectropion-uvea syndrome

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED OCULAR ANOMALIES
AXENFELD-RIEGER SYNDROME (A-R) Group of bilateral congenital anomalies that may include
abnormal development of the anterior chamber angle, the iris, and the trabecular meshwork
50% associated with glaucoma Result of abnormal development of tissues derived from the
neural crest Combination of Axenfield anomaly, Rieger Anomaly and
Rieger Syndrome Typical corneal abnormality - Posterior embryotoxon – a
prominent and anteriorly displaced Schwalbe line

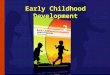
Axenfeld-Rieger Syndrome
Iridocorneal adhesions to Schwalbe line - range from threadlike to broad bands of iris tissue
Iris range from normal to markedly atrophic with corectopia and ectropion uveae

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED OCULAR ANOMALIES
PETER’S ANOMALY Condition of central corneal
opacity with adhesions between the central iris and posterior cornea
Lens may be clear or cataractous Sporadic, although autosomal
dominat and recessive forms have been reported
50% associated with glaucoma Annular corneal opacity (leukoma)
in the central visual axis, with iris strands extending from collarette to the corneal opacity
Leukoma – corresponds to a central defect in the corneal endothelium and underlying Descemet’s membrane

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED OCULAR ANOMALIES
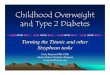
PETER’S ANOMALY (Continuation) Have defects in posterior stroma, descemet’s
membrane and endothelium without extension of iris strands to the edge of the corneal leukoma
Lens may be normal in position, w/ or w/o cataract or the lens may be adherent the posterior layers of the cornea

PETER’S ANOMALY

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED OCULAR ANOMALIES
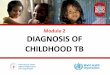
ANIRIDIA Bilateral condition characterized by a variable iris
hypoplasia that often appears as complete absence of the iris
May have limbal stem cell abnormalities that eventually result in a pannus that begins in the peripheral cornea and slowly extends centrally
Cataracts may be present at birth or may develop later in life May also have foveal hypoplasia that leads to reduced vision Mostly familial at transmitted in an autosomal dominant
form

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED OCULAR ANOMALIES
ANIRIDIA (continuation) 20% of sporadic cases are associated with a
chromosomal deletion and an increase risk of Wilms tumor
50-75% develop glaucoma Glaucoma in aniridia usually develops after
rudimentary iris stump rotates anteriorly to progressively cover the trabecular meshwork

ANIRIDIA

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED SYSTEMIC ANOMALIES
ASSOCIATED SYSTEMIC ANOMALIES AND SYNDROMESSystemic disorders associated with pediatric glaucoma: Sturge-Weber syndrome Neurofibromatosis Marfan Syndrome Weill-Marchesani syndrome

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED SYSTEMIC ANOMALIES
STURGE-WEBER SYNDROME/ ENCEPHALOTRIGEMINAL ANGIOMATOSIS A unilateral condition with ipsilateral facial cutaneous
hemangioma, ipsilateral hemangioma of the choroid and ipsilateral leptomeningeal angioma
No sex predilection and no inheritance pattern Glaucoma occurs at 30%-70% of children with this
syndrome Infants with this syndrome – thought to be due to
congenital anterior chamber anomalies Glaucoma developing after the first decade of life - result of
elevated episcleral venous pressure causing elevated IOP

STURGE-WEBER SYNDROME/ ENCEPHALOTRIGEMINAL ANGIOMATOSIS

GLAUCOMA ASSOCIATED WITH SYSTEMIC CONGENITAL SYNDROMES, WITH
REPORTED CHROMOSOMAL ABNORMALITIES
Trisomy 21 (Down Syndrome, Trisomy G syndrome)Trisomy 13 (Patau syndrome)Trisomy 18 (Edwars syndrome, Trisomy E syndrome)Turner (XO/XX) syndrome

GLAUCOMA ASSOCIATED WITH SYSTEMIC CONGENITAL DISORDERS
Lowe (Oculocerebrorenal) syndromeStickler SyndromeZellweger syndromeHallermann-Streiff syndromeRubinstein-Taybi (broad thumb) syndromeOculodentodigital dysplasiaPrader-Will syndromeCockayne syndromeFetal alcohol syndrome

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED SYSTEMIC ANOMALIES
NEUROFIBROMATOSIS Most common phakomatosis 2 forms are recognized
NF1 (von Recklinghausen disease/ Peripheral Neurofibromatosis) Most commom 1:3000-5000 Localized to band 11 of the long arm of chromosome 17 Autosomal dominant about half the time Ectropion uveae – common ocular finding Ocular Findings: Lisch nodules, optic nerve gliomas, eyelid
neurofibromas and glaucoma Systemic Findings: cutaneous café-au-lait spots, cutaneous
nerofibromas, and auxillary or inguinal freckling

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED SYSTEMIC ANOMALIES
NEUROFIBROMATOSIS NF2 (central neurofibromatosis
Localized to chromosome 22 Principal ocular finding: development of posterior
subcapsular cataracts in adolescence or young adulthood Not associated with glaucoma Defined by the presence of bilateral acoustic neuromas Frequently accompanied by multiple other nervous
system tumors

DEVELOPMENTAL GLAUCOMAS WITH ASSOCIATED SYSTEMIC ANOMALIES
OTHER SECONDARY GLAUCOMAS Causes in infants are same in adults
Trauma, inflammation, retinopathy of pre-maturity, lens associated disorders, corticosteroid use, pigmentary glaucoma and intraocular tumors
Intraocular tumors in infants and children: retinoblastoma, juvenile xanthogranuloma, medulloepithelioma
Rubella and congenital cataract are also important associated conditions
Emphasis on removal of all residual cortex during cataract surgery may reduce the occurrence of pediatric aphakic glaucoma following surgery

THANK YOU!