Embed Size (px)
Citation preview

Changes In Respiratory System With Various Physiological Conditions
Dr. Anand Kumar BansalJunior Resident
Department Of Pulmonary Medicine

Topics High-Altitude PhysiologyDeep Sea Diving And Effects Of Increased
Barometric Pressure Changes In Respiratory System During
PregnancyPhysiological Changes Of Respiratory System
With ExercisePhysiological Changes Of Respiratory System
With Aging

Normal values of pressures in inspired,expired, alveolar gas and in blood (mm Hg)

High-Altitude Physiology
ALTITUDE TYPE FROM SEA-LEVEL (In feet)• HIGH - 8,000 – 12,000• VERY HIGH - 12,000 – 18,000• EXTREMELY HIGH - Above 18,000
• An estimated 40 million people travel each year to altitudes > 8000 ft (2500 m) and as many or more travel to altitude for leisure and sports, and work in mines, military or border operations.

760 mm Hg 47 --- mm/Hg 95 ---190 ---380 ---523 ---760 ---
21%O2
78% N2
1% Other
The French physiologist Paul Bert first recognized that the harmful effects of high altitude are caused by low oxygen tension.

• Atmospheric composition of air remains almost
constant (upto 30,000 ft) but PO2 decreases with increasing altitude with FIO2 equivalent to 17% O2 at 8000 ft, down to 8% O2 at the summit of Everest (appox. 29,028 ft)
• Hypoxemia causes the physiologic responses and illnesses.
• Altitude-related exposure to cold and extreme exercise may also contribute to illness
• The adaptive changes to high altitude are collectively termed as Acclimatization

Level of altitude
Barometric pressure
Atmospheric pressure
pO2
Alveolar air Po2
pCO2 % O2 saturation of
Hb
Sea level 760 159 104 40 100
5000 630 130 80 40 95
10000 520 110 60 40 90
15000 480 90 50 36 80
18000 400 80 40 30 70
20000 350 70 <40 <30 <70
40000 140 30 12 24 15
Barometric Pressure & Partial Pressure Of Gases

Pulmonary Adaptation to High Altitude• Hyperventilaton is the most important feature due to
decreased PO2 called hypoxic ventilatory drive• Associated with increase in rate and depth of ventilation
resulting in increase in alveolar ventilation• Mechanism
Hypoxia
Carotid body stimulation
Respiratory centres stimulation
Increased ventilation
Improved hypoxia
Decreased PCO2

• Despite decrease in blood oxygen content, the delivery of oxygen to tissues is maintained by increased cardiac output and increased red cell mass (hypoxia induced erythropoietin secretion)
• The alveolar hypoxia triggers hypoxic pulmonary vasoconstriction to maintain ventilation perfusion relationship and this causes a rise in pulmonary arterial pressure. This is important in the pathogenesis of HAPE and altitude related pulmonary hypertension
• Cheyne-Stokes Respiration - Above 10,000 ft (3,000 m) most people experience a periodic breathing during sleep. The pattern begins with a few shallow breaths increases to deep sighing respirations falls off rapidly


Character & Degree Of Hypoxic Effects With Increasing Altitutude Depends Upon:
• Level of the altitude• Rate of ascent• Duration of exposure at high altitude

COMMON CLINICAL DISORDERS OF HIGH ALTITUDE
Acute High-altitude illnesss– High-altitude headache (HAH)– Acute mountain sickness (AMS)– High altitude cerebral oedema (HACE)– High altitude pulmonary oedema (HAPE)Chronic High-altitude illnesss
-- Chronic mountain sickness (CMS)

Evidence for several mechanisms for AMS, HACE, and HAPE

High-altitude Headache
• High-altitude headache (HAH) is very common, and is exacerbated by insufficient hydration in the setting of increased water loss with hyperventilation, overexertion, and insufficient energy intake, particularly in those who have experienced HAH on a previous visit to altitude.
• Acetaminophen or ibuprofen with hydration will improve this symptom.

Acute Mountain Sickness
• Acute mountain sickness (AMS) occurs after 4 to 36 hours of altitude exposure.
• Symptoms are headache (usually frontal), nausea, vomiting, irritability, malaise, insomnia, and poor climbing performance.
• The Lake Louise Symptom Score Questionnaire is the most common and useful self administered tool to determine the severity of AMS. A score of 4 and more is considered AMS, a score of 10 and more is considered severe and requires immediate intervention
Management• The key element is to limit the elevation change per day to less than
400 m/d. A slow rate of ascent is the best way to prevent AMS.

• Adequate hydration should be encouraged, and 2 L of extra fluid per day is advised
• Mild AMS is self-limiting and usually lasts about 3 days, so treatment is not mandatory
• If the symptoms progress, the patient should descend. • If descent is delayed, acetazolamide (250 mg at bedtime or 125 mg bid)
is generally considered first-line treatment; dexamethasone at a dose of 4 mg every 6 hours can be used in sulfaallergic individuals.
• A combination of the two agents can be used for rapidly evolving symptoms. These drugs are continued for a few days at altitude.
• For sleep disturbances, temazepam is effective in reducing recurrent central apnea and arousals, and appears safe to use, without any measurable adverse effects the next day.

Lake Louise Symptom Score Self-Report Questionnaire

High-altitude Cerebral Edema
• Signature symptoms are dizziness, severe almost unbearable headache, and vomiting. Ataxia is common, and a positive Romberg sign is present. Somnolence, stupor, and changes in pupillary responsiveness mark the onset of a fatal stage.
• In the absence of treatment, the condition will progress to coma and mortality will be high.
• HACE can occur even in the relative absence of AMS symptoms• Concurrent signs of pulmonary edema may also be noted. • Descent is critical. While awaiting evacuation, supplemental oxygen should be
given. Every 1% increase in oxygen concentration above 21% reduces the equivalent altitude by about 300 m.
• Administration of dexamethasone (4–8 mg), intramuscularly in severe cases, or orally in less severe cases, helps reduce cerebral edema and should be given while awaiting evacuation; doses can be repeated every 6hours

High-altitude Pulmonary Edema
• A typical patient is a fit young man who has climbed rapidly and is energetic on arrival.
• Prevalence estimates are 0.5% to 2.0% of those rapidly ascending to altitude. • A cough develops, which is initially dry, then productive of frothy white
sputum, later becoming blood tinged. The climber may complain of chest discomfort. The pulse and respiratory rate are increased, and auscultation of the chest reveals crackles at the bases. An elevated jugular venous pressure and peripheral edema may be seen.
• As breathing becomes “bubbly” due to pulmonary edema, cyanosis develops.• In the absence of definitive treatment, hypoxemia progresses to respiratory
failure, and coma and death ensue.• High-altitude pulmonary edema (HAPE) may occur independently of AMS.

Mechanism• HAPE is caused by migration of fluid into extravasal space through endothelial
damage along with shear stresses produced by increased cardiac output and pulmonary artery pressure.
Prevention• In those who have experienced HAPE before, use of nifedipine prophylactically (20
mg twice daily prior to ascent, then three times daily) appears to lower significantly the incidence of HAPE.
Treatment• Descent is critical for survival. • Initial medical treatment while the subject awaits descent includes strict rest and
supplemental oxygen.• Nifedipine (10 mg sublingually) may be used. If clinically significant hypotension
does not occur with the first dose of nifedipine, its administration can be repeated every 15 to 30 minutes

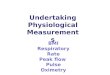
Copyright ©2003 BMJ Publishing Group Ltd.
Barry, P W et al. BMJ 2003;326:915-919
No Caption Found


Pathway for management of acute altitude illnesses

Chronic Mountain Sickness
• The defining feature is extreme polycythemia, with hemoglobin concentrations as high as 23 g/dL and hematocrits as high as 83%.
• Patients may have vague neuropsychological complaints, including headache, dizziness, somnolence, fatigue, difficulty in concentration, and loss of mental acuity.
• The condition of CMS is quite different from AMS. Excessive erythrocytosis associated with a lower oxygen saturation and hypoxic ventilatory response with relative hypercapnia are the main features of CMS, followed by right ventricular enlargement, pulmonary hypertension, and remodeling of pulmonary arterioles.
• Descent to sea level is the definitive treatment. • However, for those who wish to remain at altitude for family or
economic reasons, phlebotomy and administration of supplemental oxygen are beneficial.

Deep Sea Diving And Effects Of Increased Barometric Pressure
• The air-containing atmosphere of the earth applies pressure to any object within it.
• At sea level this pressure is defined as one atmosphere (1 ATM). • One atmosphere is equivalent to 760 torr (mm Hg), 29.92 in Hg,
14.7 psi, 101.3 kPa, or 1.013 bar.• Every 10 m or 33 ft of sea water (fsw) through which a diver
descends adds an additional 1 ATM of pressure.• High ATM pressure seen in – Deep sea diving– Submarines– Caisson’s workers.


Physiological Problems Under Depth
• Due to mechanical effects
• Due to effect of high pressure on respiratory gases.

Physiological Problems Due To Mechanical Effects Of High Atmospheric Pressure
• At a depth of more than 30 meters (100 ft)
• Caving of the chest• Damage to the face• Squeezing of air in the
Paranasal sinuses & middle ear.

Physiological Problems Due To Effect Of High Pressure On Respiraatory Gases.
• Effect of increases PO2• Effect of increased PN2
(nitrogen narcosis)• Effect of carbon
dioxide build up.

Effect Of Increased Po2
• Acute oxygen toxicity – Disorientation,
dizziness, convulsions & coma
• Chronic oxygen toxicity – Irritation of airways– Pulmonary edema &
atelectasis– Bronchopneumonia.
At 4 atm pressure dissolved oxygen increased from 2 to 9ml/100ml
Raises tissue Po2 & changes molecular oxygen to active oxygen.
Superoxide anion- free radical.
Oxidizes PUFA of cell membrane & enzymes – damage cell metabolism – nervous complication.

Effect Of Increased Pn2 (Nitrogen Narcosis)
• PN2 increases when breathed compressed air• Nitrogen dissolves in body fluids
N2 dissolves in FATS

Effect Of Carbon Dioxide Build Up
Person rebreathes
CO2
Passage of CO2 long time in body fluids –
reach toxic levels
Respiratory acidosis & CO2
narcosis.

Physiological Problems Of Ascent• Decompression Sickness
(DCS)• Air Embolism

Decompression Sickness
• Caisson’s disease/Dysbarism/compression of air sickness/the bends/diver’s palsy.
• Cause – under high pressure nitrogen in the breathed air dissolved in the body fluids & fats.

• When individual ascend rapidly to sea level, nitrogen is decompressed & escapes from the tissue in the form of bubbles
• These bubbles block the blood vessels – ischemia & infarction.

Caissons chamber

Symptoms
• Pain in joints & muscles – Bends
• Neurological symptoms – dizziness, collapse, unconsciousness, Sensation of numbness
• Erythematous macular rash involving the trunk
• Coronary ischemia & MI

Treatment
• Slow decompression • Hyperbaric oxygen• Decompression
chamber

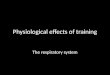
Decompression Chamber or Hyperbaric chamber
A sealed compartment used to treat Air Embolism and decompression sickness, in which pressure is first increased and then gradually decreased

Air Embolism
• Due to entry of air into blood circulation following rupture of pulmonary capillaries, arteries & veins due to sudden expansion of gases in lungs due to sudden fall in atmospheric pressure.
• Occurs in Caisson’s workers.

Symptoms • Chest pain, tachypnoea,
systemic hypotension, hypoxemia
• Sometimes air emboli to systemic circulation – death.
Treatment• Slow decompression • Decompression chamber• Hyperbaric oxygen

Prevention of Physiological Problems Occuring at Depth & Ascent
Measures for short duration dive up to 20 meters Take rapid & deep breaths before diving – CO2 washes out – N2 does
not get enough time to dissolve – O2 toxicity not occur.
Measures for deeper & longer dives Use of breathing apparatus – gives gas to breath & either
dissolves CO2 ( close circuits) or bubbles out in water (open circuits)
SCUBA DIVING ( Self-Contained-Underwater-Breathing-Apparatus) Use of breathing mixtures containing helium & low oxygen
concentration – prevent O2 toxicity. Slow ascent or use of Decompression chamber

Changes In Respiratory System During Pregnancy
• The anatomic and physiological changes of pregnancy have major pulmonary and cardiovascular consequences throughout the gestation.
• An understanding of these changes is necessary since inappropriate diagnosis and interventions may occur in the absence of this knowledge.

Anatomic changes of normalpregnancy
Upper Airways• Hyperemia, friability, mucosal edema, and hypersecretion of
the airway mucosa -- most pronounced in the upper airways, especially during the third trimester.
• Nasal obstruction, epistaxis, sneezing episodes, and vocal changes may occur, and these may worsen when the individual lies down.
• Nasal and sinusoidal polyposis is often seen and tends to recur in women with each pregnancy.

• Nasal obstruction may contribute to upper airway obstruction during sleep, leading to snoring and even obstructive sleep apnea.
• The physiological causes of nasal mucosal changes appear to be predominantly mediated by estrogens.
• Estrogens increase tissue hydration and edema. They also cause capillary congestion and hyperplastic and hypersecretory mucous glands.

Lower airways• Mucosal changes that affect the upper airways may also occur in the central
portion of the airway, such as the larynx and trachea.
• Nonspecific complaints of airway irritation, such as irritant cough or sputum production.
• The enlarging uterus produces upward displacement of the diaphragm → increase in the anteroposterior and transverse diameters of the thoracic cage
• Diaphragm may be elevated up to 4 cm, but diaphragmatic function is not impaired
• Thoracic cage circumference increase by upto 6 cm

• Progressive relaxation of the ligamentous attachments of the ribs broadens the subcostal angle from 60-70 degrees to around 100-110 degrees.
• The shortening and widening of the thoracic cavity results in upward and lateral displacement of the cardiac apex on chest radiography.
• Abdominal muscles have a decreased tone and are less active during the pregnancy, causing respiration to be more thoracic and less diaphragmatic.

Physiological changes of normalpregnancy
• Enlarging uterus cause serial changes in lung volumes• The dead space volume increases due to relaxation of
musculature of the trachea and the bronchi by progesterone• Tidal volume increases gradually by 35-50% as the
pregnancy progresses• Total lung capacity (TLC) is reduced slightly (4 to 5%) by the
elevation of diaphragm• The functional residual capacity (FRC) residual volume (RV),
and expiratory reserve volume (ERV), all decrease by about 10-20% due to anatomical changes in the thoracic cage
• Inspiratory capacity (IC) increases by 5-10%

• The forced vital capacity (FVC) is largely unaltered till later in pregnancy as the widened chest diameters counter the effects of the raised diaphragm
• FEV1/FVC ratio is usually not affected. Therefore, the dyspnea of normal pregnancy is not responsive to bronchodilators
• Lung compliance does not change significantly but compliance of the thoracic cage decreases
• In early pregnancy Diffusing capacity is either unchanged or slightly increased. During rest of pregnancy, the diffusing capacity decreases
• Oxygen consumption start increasing from first trimester and reaches a maximum of 20% - 30% by term.

• Increase in respiratory minute volume by appox. 26% associtaed with the increase in tidal volume with a normal or increased respiratory rate
• As the respiartory minute volume increases “hyperventilation of pregnancy” occurs which results in a respiratory alkalosis with compensatory renal excretion of bicarbonate
• PCO2 falls to levels of 28 to 32 mmHg• Bicarbonate decreases to 18 to 21 mEq/L• Arterial pH is maintained in the range of 7.40 to 7.45• This maternal hyperventilation is considered a protective
measure that prevents the fetus from excessive levels of CO2

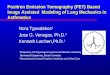
Lung volume changes associated with pregnancy
Although total lung capacity, residual volume, and expiratory reserve volume diminish, vital capacity is preserved in values similar to nonpregnant women

Physiologic Dyspnea of Pregnancy• The increase in minute ventilation that accompanies pregnancy is
often perceived as shortness of breath.
• Shortness of breath at rest or with mild exertion is so common that it is often referred to as ‘‘physiologic dyspnea.’’
• The increase in minute ventilation and the load imposed by the enlarging uterus cause an increase in the work of breathing.
• Other factors contribute to the sensation of dyspnea include increased pulmonary blood volume, anemia, and nasal congestion

• Differentiate the normal dyspnea of pregnancy from that due to disease pathology.
• Pathologic dyspnea : increased respiratory rate greater than 20 breaths per minute, arterial PCO2 less than 28 or greater than 35 mm of Hg, hypoxemia or abnormal measures on forced expiratory spirometry, or cardiac echocardiography
• Abrupt or paroxysmal episodes of dyspnea suggest an abnormal condition

SUMMARYChest Wall/Lung Mechanics• Thoracic diameter Increased• Diaphragm Elevated• Lung compliance Unchanged• Chest wall compliance Decreased
Lung Volumes• Total Lung Capacity - slightly decreased• Vital capacity - Unchanged or slightly increased• Inspiratory capacity -Slightly increased• Functional residual capacity- Decreased• Residual volume - decreased• Expiratory reserve volume- Decreased

Spirometry• FEV1 Unchanged• FVC Unchanged• FEV1/FVC Unchanged
Ventilation• Minute ventilation Increased• Tidal volume Increased• Respiratory rate Unchanged

Gas Exchange• DCO Unchanged or slightly decreased
Blood gases• pH 7.40 to 7.45• PaCO2 decreased to 28 to 32 mmHg• Bicarbonate Slightly decreased (18 to 21
mEq/L)

Physiological Changes Of Respiratory System With Exercise
• As exercise commences pulmonary ventilation (breathing) increases in direct proportion to the intensity and metabolic needs of the exercise.
• Ventilation increases to meet the demands of exercise through the following two methods:1. An increase in ‘tidal volume’ which refers to the quantity of air that is inhaled and exhaled with every breath.2. An increase in the ‘respiration or breathing rate’ which refers to how many times a person completes an inhalation and exhalation every minute.
• If the exercise is intense, breathing rates may increase from a typical resting rate of 15 breaths per minute up to 40 – 50 breaths per minute.

• Immediate in ventilation– Begins before muscle contractions– Due to cerebral input to the respiratory center in the
anticipation of the increased needs depending on the past experiences and afferent impulses from proprioceptors in muscles, tendons and joints
• Gradual second phase of in ventilation– Driven by chemical changes in arterial blood– CO2, H+ sensed by chemoreceptors– Right atrial stretch receptors

• Ventilation increase proportional to metabolic needs of muscle– At low-exercise intensity, only tidal volume – At high-exercise intensity, rate also
• Ventilation recovery after exercise delayed– Recovery takes several minutes (may take upto 90
minutes)– May be regulated by blood pH, PCO2, temperature


Increased Tidal Volume• Tidal volume increases from 10% to 50-60%
of vital capacity with increasing exercise intensity to supply oxygen to working muscles.
INCREASED Pulmonary Ventilation• While the level of maximum ventilation
achieved is dependent on the intensity of exercise, it is seldom beyond 20 times the resting level, i.e. upto 100 to 110 L.
• The maximum breathing capacity is about 150 to 170L in an average person.
• There is still sufficient reserve available for extreme circumstances such as exercise at high altitudes and in extreme environments.

Decreased ratio of Dead Space (VD) to Tidal Volume (VT)• Airway resistance decreases owing to bronchodilation as soon as exercise
begins. Likewise, the ratio of dead space (VD) to tidal volume (VT) decreases. The drop in VD/VT is moderate at low-to-moderate exercise intensities. The VD itself changes minimally with bronchodilation, the change in ratio being largely due to the increased VT. This is advantageous, as it results in greater alveolar ventilation for given minute ventilation.
No Change to Vital Capacity• Lung volume remains unchanged, as it can not be increased as a short term
effect to exercise.

Increased Alveolocapillary Gradient for O2
• Increased extraction of oxygen in the exercising tissues results in a fall in the mixed venous PO2 of blood reaching the right side of the heart, from a normal of 40 mm Hg to 25 mm Hg or even less.
Increased Oxygen Uptake• Oxygen uptake increases with
increasing exercise intensity.• Oxygen uptake will not increase
further once maximum level of oxygen uptake is reached (VO² Max)

Increase in Diffusion Capacity for O2• Upto 3 times on exercise• Results from recruitment of underperfused pulmonary capillary beds
due to increased blood flow and pulmonary artery pressure• The pulmonary blood flow increases from a normal of 5.5 L/min to
as much as 20–35 L/min.
Increased Efforts From Ribcage Muscles and Diaphragm• Diaphragm and intercostal muscles will work harder to enable
increased expansion and contraction of thoracic cavity.• The increased movement of the cavity can accommodate an
increased air volume, required to supply active muscles with oxygen

Physiological Changes Of Respiratory System With Aging
Basic changes that affect lung function are-• Decrease respiratory muscle strength.• Decrease in elastic recoil of lung tissue.• Stiffening of chest wall and calcification of costal
cartilages.• Decrease in size of intervertebral spaces.• Loss of alveolar surface area and pulmonary
capillary blood volume. These effects may present singly or in combination

Anatomical change• Air space size increases due to senile
emphysema.• Compliance- Chest wall compliance decreased.- Lung compliance - increased to normal- Total respiratory compliance decreased

• Lung function- FEV1 is decreased- FVC is decreased- TLC is unchanged- Vital capacity is decreased- Function residual capacity is increased- Residual volume is increased
• Loss of alveolar elastic tissue results in decrease traction on smaller airways to oppose dynamic compression during expiration leading to airway closure at higher lung volumes.

• Muscle strength- Maximal inspiratory pressure decreases- Transdiaphragmatic pressure decreases- Maximum voluntary ventilation decreased• Immunology - Neutrophils % is increased- Ratio of CD4+/CD8+ cells is increased- Anti-oxidant levels are decreased

Summary• There is marked variation in effect of aging on lung function.• Aging is associated with reduction in chest wall compliance
and increased air trapping.• The decline in FEV1 with age likely has a non-linear phase
with acceleration in decline after the age of 70 yrs.• There is increase in air space size resulting from loss of
supporting tissue.• Respiratory muscle strength decreases with age more so in
men than in women.• Despite all these changes respiratory system is capable of
maintaining adequate oxygenation and ventilation during the entire life span. However, the respiratory system reserve is limited with age and diminished ventilatory response to hypoxia and hyper-capnia makes it more vulnerable to ventilatory failure during high demand states (heart failure, pneumonia) and possible poor outcome.


THANK YOU !!!