Embed Size (px)
DESCRIPTION
2011 Clinical Education and Training Institute Annual report 2011
Citation preview

Clinical Education and Training InstituteAnnual Report 2010-2011
Clinical education for excellencein patient care

Legislation Health Services Act 1997, Order Amending Schedule 2 of the Act (insertion of entry for Clinical Education and Training Institute) June 2010.
Clinical Education and Training Institute Annual Report 2010-2011
State Health Publication Number (CETI) 110268
ISSN 1839-7549
Key words: Clinical education, New South Wales Australia.
Suggested citation for manuscripts and publications: Clinical Education and Training Institute Annual Report 2010-2011. Clinical Education and Training Institute, Sydney, October 2011.
Clinical Education and Training Institute
Building 12, Gladesville Hospital, GLADESVILLE NSW 2111 Locked Bag 5022 GLADESVILLE NSW 1675 Tel. (02) 9844 6551 Fax. (02) 9844 6544
Homepage: www.ceti.nsw.gov.au Email: [email protected]
© CETI 2011. This work is copyright.
It may be reproduced in whole or in part for study or training purposes subject to the inclusion of an acknowledgement of the source.
Further copies can be downloaded www.ceti.nsw.gov.au
Acknowledgements
Images on cover and pages 16, 25, 30, 32 and 35 courtesy of Audio Visual Services, Sydney Local Health District Images on pages 3, 18, 20 and 24 thanks to allied health staff at Prince of Wales Hospital Images on pages 6 and 10 thanks to nursing & midwifery staff at Orange Base Hospital

CETI > ANNUAL REPORT 2010/11 1
Letter of submission 02
1. Overview 02Who we are and what we do 03Management and structure 05Chief Executive’s report 08General Manager’s report 09Operational highlights 10Publications and resources 12Conferences/forums 13Our strategic plan 14Overview of financial performance 15
2. Report against our goals 16Goal 1: Education and training supporting safe, multi-disciplinary, team-based, patient-centred care 16Goal 2: Professional development to build clinical skills, knowledge, competency and capacity 18Goal 3: Workforce management 21Goal 4: Flexibility, innovation and quality in learning 24Goal 5: Improved standards in education and learning 26Goal 6: Knowledge and knowledge management 28Goal 7: Communication 30Goal 8: Collaboration 32Evaluation 34
3. Our people 36Management and staff 36Committees 37
4. Financial report 48
5. Appendices 90Compliance requirements 90Internal audit and risk statement 95Abbreviations 96Glossary 97Index 99
Contents

OVERVIEW2
1 Overview
The Hon Jillian Skinner Minister for Health Governor Macquarie Tower 1 Farrer Place SYDNEY NSW 2000
Dear Minister
We have pleasure in submitting the Clinical Education and Training Institute (CETI) Annual Report 2011.
The report complies with the requirements for annual reporting under the Annual Reports (Statutory Bodies) Regulation 2010 under the Annual Reports (Statutory Bodies) Act 1984.
This report summarises our performance for 2010-2011, our first year of operation. This report enunciates the education and training programs coordinated by CETI, outcomes from the programs and collaborative achievements. It includes comments on our financial results and our contributions to the development and improvement of education and training across the NSW health system.
We commend to you this report on the Clinical Education and Training Institute’s involvement in the development and delivery of innovative and collaborative training programs for health professionals in the NSW, supporting excellence in patient care.
Yours sincerely
Professor Steven Boyages Dr Gaynor HeadingChief Executive General Manager
Letter of submission

CETI > ANNUAL REPORT 2010/11 3
Our historyThe Clinical Education and Training Institute (CETI) was established on 1 July 2010 by the NSW Government under the Health Services Act 1997 as one of the “four pillar” key health organisations recommended by the 2009 Garling Inquiry. CETI is a statewide multidisciplinary education and training agency dedicated to the support and development of the health workforce and quality and safety in patient care.
As part of CETI’s formation, two existing agencies and their functions – the Institute of Medical Education and Training (IMET) and the NSW Institute of Rural Clinical Services and Teaching (IRCST) – were absorbed into CETI.
Determination of functionsCETI is a Statutory Health Corporation with a determination of functions:
1. To provide leadership, and work closely with area health service and other public health organisations and clinical training providers, to ensure the development and delivery of clinical education and training across the NSW public health system which:a. Supports safe, high quality, multi-
disciplinary team based, patient centred care
b. Meets service delivery needs and operational requirements
c. Enhances workforce skills, flexibility and productivity
2. To design, commission, conduct, coordinate, support and evaluate a clinical education and training program for all new graduate clinical and clinical support staff in the public health system, which supports their roles in providing safe, high quality, multi-disciplinary team based, patient centred care
3. To design, commission, conduct, coordinate, support and evaluate such other postgraduate clinical education and training programs as the Director-General may direct from time to time
4. To design, commission, conduct, coordinate and support professional development programs to enable clinicians to become skilled teachers, clinical leaders, trainers and supervisors
5. To develop and oversee performance evaluation programs for post graduate clinical education and training in the NSW public health system
6. To set standards for prevocational medical training and accredit institutions for prevocational education and supervision
Who we are and what we do
OVERVIEW4
1 Overview
7. To institute, coordinate and evaluate clinical training networks, including postgraduate medical training networks, and ensure they support service delivery needs, meet operational requirements and are, as far as possible, consistent with, clinical service network
8. In undertaking its functions, to consult and liaise with patients and their carers, clinical and clinical support staff. The Department of Health organisations and providers of clinical education and training
9. To provide advice to the Department of Health, Director-General and Minister on matters relevant to its functions
Our visionOur vision is to build sustainable capacity to achieve better health for the people of NSW through education, training and development of the clinical workforce.
How we workWe achieve our goals through investment, innovation and influence. We coordinate, develop, evaluate and implement clinical education and training for medical, nursing and midwifery, allied health, and clinical support staff, and enhance the capabilities of the workforce by facilitating professional development opportunities, accrediting training facilities and providers and allocating medical intern places.
Our valuesCOLLABORATIONWe work in partnership and in teams for common goals.
EXCELLENCEWe strive for excellence in our communication, programs, products and resources, services and relationships.
TRANSPARENCYWe champion transparency via our commitment to accuracy, communication and our code of conduct.
INNOVATIONWe celebrate innovation by embracing new ideas and emerging technologies while building the evidence base.
Our stakeholdersTo achieve our aim of excellent patient-centred, team-based care in NSW, CETI works collaboratively with a broad range of stakeholders including patients, clinicians, nurses, allied health professionals, clinical support staff, partner agencies, public health services, private health services, professional colleges, clinical training committees and working group members, medical administrators, vocational and tertiary education providers, researchers, NSW Health and the Department of Health and Ageing.
Our staffAt 30 June 2011, we employed 65 people (permanent/fixed term) in a variety of roles.
Our governanceCETI is a statutory body led by the Chief Executive, with the following statutory committees: Chief Executive Committee; Audit and Risk Committee; and Finance and Performance Committee.
Our organisational structureCETI is comprised of four directorates and one centre: • The Allied Health Directorate• The Medical Directorate• The Nursing and Midwifery
Directorate• The Rural and Remote Directorate• The Centre for Learning and
Teaching
These directorates and the centre are supported by the Office of CETI (finance, human resources, governance).
Where we operateCETI operates in NSW. Our head office is located at the old Gladesville Hospital, Gladesville, NSW. Our Rural and Remote Directorate has its main office in Dubbo NSW with smaller offices across the state hosted by Local Health Districts (LHDs).
Principal Office: Clinical Education and Training Institute Building 12, Gladesville Hospital Shea Close, off Victoria Road Gladesville NSW 2111
Locked Bag 5022, Gladesville NSW 1675
Telephone: 02 9844 6551 Facsimile: 02 9844 6544
Home page: www.ceti.nsw.gov.au Email: [email protected]
Office hours: 8:30am to 5:00pm weekdays.

CETI > ANNUAL REPORT 2010/11 5
Management and structure
CETI is a Chief Executive governed statutory body.
Chief Executive: Professor Steven Boyages MB BS PhD DDU FRACP FAFPHM
Steven was formerly the Chief Executive of the Sydney West Area Health Service and has professorial appointments to the University of Sydney and the University of Western Sydney. Steven continues to work in the clinical field of endocrinology and was previously the Director of Diabetes and Endocrinology at Westmead Hospital from 1990 to 1999. He was the foundation director of the Centre for Research and Clinical Policy in NSW Health in 1999.
General Manager: Dr Gaynor Heading PhD
Gaynor has held diverse roles including Senior Manager at the Cancer Institute NSW, Associate Professor at the University of Sydney, and has worked as a research methodologist at the University of Newcastle. Gaynor has a PhD in Medicine.
Our directorates and centreTHE MEDICAL DIRECTORATEThe Medical Directorate continues the work undertaken by the NSW Institute of Medical Education and Training (IMET). The Medical Directorate’s remit covers accreditation, intern allocation, prevocational medical training, generalist training and specialist training for clinicians.
CETI facilitates vocational training networks to support senior residents and trainees (registrars) through a number of specialist training programs including Advanced Cardiology, Basic Physicians, Emergency Medicine, Oncology, Paediatrics, Psychiatry, Radiology and Surgical Skills. The Medical Directorate provides an orientation resource for international medical graduates and also has a Rural Medical Scholarship Program that supports medical trainees committed to training and providing patient care in rural locations in NSW through the continuum of their training and education years.
THE RURAL AND REMOTE DIRECTORATEThe Rural and Remote Directorate continues the work of the NSW Institute of Rural Clinical Services and Teaching (IRCST). The main office for the Rural and Remote Directorate is in Dubbo, but a number of other smaller offices exist across NSW, hosted by various LHDs. The directorate supports rural and remote health professionals and builds clinical and service capability and capacity.
The directorate offers a range of programs, conferences and scholarships developed specifically to meet the needs of our rural and remote workforce. The staff of the
Chief Executive
Office of CETI
Nursing and Midwifery Directorate
Centre for Learning and Teaching
Medical Directorate Rural and Remote Directorate
Allied Health Directorate
OVERVIEW6
1 Overview
directorate bring a broad base of rural and remote experience to the table when planning, developing and implementing our various initiatives which in turn contribute to an effective and sustainable rural and remote health system.
CETI is a Registered Training Provider with the Royal Australian College of General Practitioners and the Australian College of Rural and Remote Medicine. Our educational programs are also endorsed by the Royal College of Nursing, Australia.
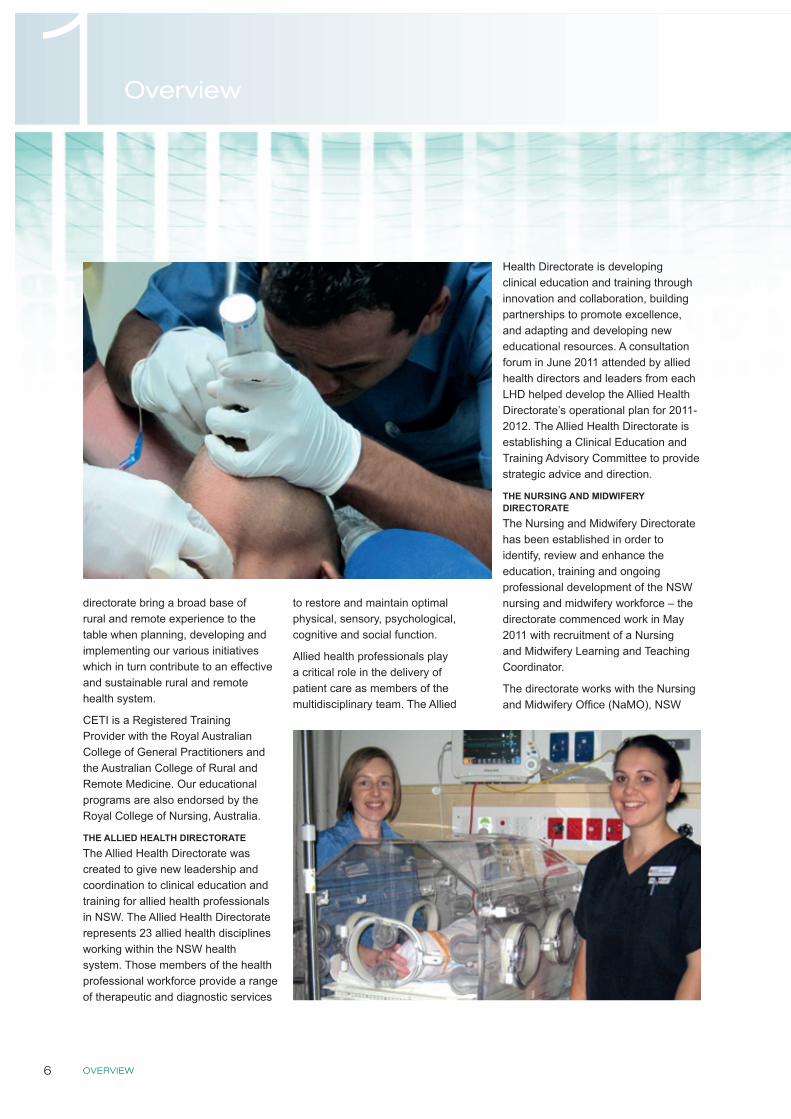
THE ALLIED HEALTH DIRECTORATEThe Allied Health Directorate was created to give new leadership and coordination to clinical education and training for allied health professionals in NSW. The Allied Health Directorate represents 23 allied health disciplines working within the NSW health system. Those members of the health professional workforce provide a range of therapeutic and diagnostic services
to restore and maintain optimal physical, sensory, psychological, cognitive and social function.
Allied health professionals play a critical role in the delivery of patient care as members of the multidisciplinary team. The Allied
Health Directorate is developing clinical education and training through innovation and collaboration, building partnerships to promote excellence, and adapting and developing new educational resources. A consultation forum in June 2011 attended by allied health directors and leaders from each LHD helped develop the Allied Health Directorate’s operational plan for 2011-2012. The Allied Health Directorate is establishing a Clinical Education and Training Advisory Committee to provide strategic advice and direction.
THE NURSING AND MIDWIFERY DIRECTORATEThe Nursing and Midwifery Directorate has been established in order to identify, review and enhance the education, training and ongoing professional development of the NSW nursing and midwifery workforce – the directorate commenced work in May 2011 with recruitment of a Nursing and Midwifery Learning and Teaching Coordinator.
The directorate works with the Nursing and Midwifery Office (NaMO), NSW

CETI > ANNUAL REPORT 2010/11 7
Health and other stakeholders to identify and respond to gaps and development opportunities in nursing and midwifery. Major streams of activity for the Nursing and Midwifery Directorate in 2011-2012 will establish governance for nursing and midwifery clinical education and training in NSW, support the learning culture for nursing and midwifery and provide flexible online learning modules that build knowledge and skills required to support a team-based approach to patient care. Work will also be done to develop a guide for nurses and midwives within NSW Health who are responsible for staff supervision.
THE CENTRE FOR LEARNING AND TEACHINGCETI’s Centre for Learning and Teaching provides support and
expertise to CETI directorates and the NSW health system. The Centre houses the Interprofessional Practice Unit (including the Team Health program), and Learning Innovations and Future Technologies. The Centre provides curriculum, competency and capability expertise and educational resource development. CETI plays a leadership role in e-learning and is establishing standards and guidelines for the state. CETI is partnering with Health Support Services to support state-wide e-learning initiatives.
Team Health is a new program which aims to improve teamwork, communication and collaboration for safer patient-centred care and better staff experiences. It will do this by implementing team-based interprofessional learning
activities drawn from the substantial interprofessional learning literature. Activities include the Right Start Program (a pregraduation program for health profession students), clinical team modules (aimed at new and current employees within a clinical team), policy development (influencing health policies and implementation plans), and system integration (working in partnership with existing stakeholders already developed local training initiatives).
In June 2011, Team Health held an inaugural Team Health Consultation Forum with directors of workforce, learning and development managers, clinical redesign managers, workforce design managers and representatives from CEC, BHI and ACI.
OVERVIEW8
1 Overview
Chief Executive’s report
Health is a knowledge-centred enterprise. Those working in health are involved in the business of generating new
knowledge (research and evaluation), imparting knowledge to their workforce (education and training) and applying knowledge for the betterment of health (service delivery).
CETI was formed as one of the four pillars supporting public health services in NSW following the 2008 Garling Inquiry. CETI builds capacity, competency, collaboration, communication, coordination, culture and clinical care models that support safe, high quality, interprofessional team-based, patient-centred care that meets service delivery needs and operational requirements.
CETI has a huge responsibility to the people who use and work for our public health services. We fulfill that responsibility through investment in new programs, collaborating with key stakeholders (e.g. universities, colleges, clinical leaders, health services, the community) and through innovation. Our work helps to improve communication, capacity and competency by using blended learning approaches (e.g. face-to-face, simulation and e-learning) to provide a responsive health workforce, available in appropriate numbers to meet growing health service challenges.
CETI has built on the excellent work of its foundation directorates, Medical and Rural. Our stakeholders have a strong desire to maintain discipline-specific directorates as well as creating cross-linking inter-professional units. CETI has established new programs including e-learning, allied health,
nursing and midwifery, interprofessional practice and an organisational structure to support this expanded focus.
This year CETI has been working on a number of initiatives across a range of areas. CETI’s major achievements to date have included solutions to training challenges posed by the increased supply of medical graduates (interns), the development of an interprofessional team program for new starters in health and the development of common standards and platforms for a state-wide learning management system. We have also produced the Superguide as a guide for medical supervision and established the Allied Health Directorate and its advisory committee.
Other highlights have been: CETI’s new Surgical Sciences Course which is seeking specialist College accreditation; Nursing Grand Rounds by videoconference enhancing the knowledge of 180 rural nurses; and achieving 50 graduates from the rural clinical team leadership and management programs. We have also established our Nursing and Midwifery Directorate and agreed on a program of work drafted with NaMO.
Planned activities and outcomes for the following year include:
INNOVATION AND TECHNOLOGY • Future Technologies Unit supporting
simulated learning environments and e-learning within LHDs, and promoting e-learning standards.
INTERPROFESSIONAL / MULTIDISCIPLINARY• In partnership with LHDs, CETI will
develop Team Health’s Right Start Program consisting of blended learning modules which will build core foundation skills and improve the workforce readiness of new graduate health professionals
• A supervisor training course based on the Superguide handbook aims to provide a certifiable level of supervision skills to participants in all clinical professions
• Development of training modules for common skill areas including teaching skills
MEDICAL EDUCATION AND TRAINING• Online prevocational trainee
assessment and online prevocational training term evaluation
ALLIED HEALTH• The Superguide: a handbook for
supervising allied health professionals will be published in October 2011
• Allied health clinicians and the CETI Allied Health Advisory Committee will identify opportunities for allied health learning
NURSING & MIDWIFERY• The Superguide: a handbook for
supervising nurses and midwives, planned for 2011 publication
RURAL & REMOTE• GP Procedural Training Program
developed for an integrated state-wide model
• Training and Support Unit for Aboriginal mothers, babies and children will run workshops and training, for staff supporting families
May I take this opportunity to thank all those who have worked so hard for CETI and with CETI to deliver these wonderful highlights and who are working together to make our future achievements happen.
Professor Steven Boyages MB BS PhD DDU FRACP FAFPHM Chief Executive
CETI > ANNUAL REPORT 2010/11 9
General Manager’s report
Due to Garling’s vision, in CETI we now have a NSW Health organisation dedicated to supporting the development of
clinicians’ technical and non-technical knowledge, skills and capability. It is important to have an agency dedicated to learning that can partner with stakeholders to drive innovation in learning, develop learning standards, promote resource sharing and support excellence in learning. Establishing this new institution has been a major undertaking, needing leadership and engagement with stakeholders as we take on new challenges and integrate existing programs and systems.
Leadership and legacy programsThe lead time needed to change and develop people can be shortened with strong leadership and legacy programs. CETI was lucky in this regard as we were able to build on the strong activities of two existing Institutes which were dissolved and had their functions transferred to CETI, namely the Institute of Medical Education and Training (IMET) and the NSW Institute of Rural Clinical Services and Teaching (IRCST).
This legacy supported the creation of new directorates (Allied Health, Nursing and Midwifery) and a Centre for Learning and Teaching with specialist skills in developing interprofessional learning resources, competencies and innovation in learning. We were able to capitalise on the learnings and resources produced by IMET and IRCST and swiftly commence the development of new resources e.g. the Superguide for Allied Health.
We initiated the series of consultations for our Team Health Program and used existing structures (e.g. the Prevocational Forum) to gain rapid insight into learners’ needs.
EngagementEffective development of clinicians and health professionals involves engagement with hearts and minds, tapping into local strengths and balancing the local with central roles and priorities. CETI strongly supports working collaboratively, with stakeholder involvement on our program committees and clinical programs being led by clinical chairs. It has been important to hold a number of consultation forums, particularly around the establishment of our new directorates. Another way CETI is supporting engagement is by aiming to make learning resources as accessible as possible.
CETI staff have been highly engaged and have demonstrated resiliency as we navigated the old to invent the new. Our expanded remit has been reflected in much evidence of our staff collaborating across disciplines as they bring their education and training skills and their stakeholder engagement skills together. This work has resulted in new online resources and a new-look website which has laid the groundwork for an enhanced learning platform, planned for next year. The notions of access to learning materials, support for local training and limiting resource duplication have shaped CETI’s programs of work and will remain important.
Improving outcomesTo support the overall goal of improved patient outcomes we have laid the groundwork for evaluating our activities. The CETI evaluation framework is linked to our strategic direction and will be refined to ensure that we can report on relevant key performance indicators. To support staff development, a CETI Colloquium series has been established which provides a forum for exchanging ideas and theory related to learning, and the Office of CETI has supported in-house training related to evaluation, technologies and stakeholder learning.
The breadth of CETI outputs reflects staff dedication to improving patient outcomes and the clinical experience. I appreciate stakeholder and staff efforts and look forward to new learning initiatives that will develop capacity in the health economy.
Dr Gaynor Heading General Manager
CETI is an agency dedicated to learning that can partner with stakeholders to drive innovation in learning, develop learning standards, promote resource sharing and support excellence in learning

GOAL KEY ACHIEVEMENTS
OVERVIEW10
1 Overview
Operational highlights
In our first year of operation CETI has been implementing the recommendations from the Garling Report.
Our new Allied Health and Nursing and Midwifery Directorates have built on the great work of our foundation directorates (Medical, and Rural and Remote)
Our new Centre for Learning and Teaching (CLT) has established Team Health to promote interprofessional team-based patient-centred care, one of the key recommendations arising from the Garling Report. The CLT is also driving our input into e-learning to establish online standards and flexible learning.
We have built on sound foundations in a number of key programs including the allocation of medical interns to training networks, with the greatest number of interns ever placed in NSW (one third of Australia’s total intern placements). We have done this while working to ensure the allocation of resources and support to rural and remote areas and the development of the Aboriginal Mothers and Babies Training Support Unit.
GOAL KEY ACHIEVEMENTS
Education and training supporting safe, multi-disciplinary, team-based patient-centred care
• Set up Team Health and interprofessional training modules• Called for expressions of interest to run interprofessional training
for new graduates under our Right Start program• Contributions to policy to enhance team-based care
• Review of induction process for international medical and nursing graduates
• Supporting rural team-based clinical improvement process• The Leadership and Management Essentials Program trained
31 from a range of disciplines over nine months
Professional development to build clinical skills, knowledge, competency and capacity
• New Allied Health Directorate established as a major initiative to promote training and learning resources for allied health professionals
• New Nursing and Midwifery Directorate established to support the training needs of nursing and midwifery
• GP Procedural Training Program supported 25 rural positions• Basic Physician Training (BPT) increased numbers and helped
achieve higher pass rates• Physician Education Program (PEP) by video and online assisted
192 trainees• Psychiatry education support by providing access to workshops
and developing resources with online access• Paediatrics professional qualities curriculum development• New online resources for emergency medicine trainees to help
prepare for exams
• Basic Sciences in Oncology Course (BSOC) reached 40 participants over 95 teaching sessions
• New Surgical Science Intensive Course developed for those not enrolled in the RACS Surgical Education and Training (SET)
• Training and Support Unit for Aboriginal Mothers, Babies and Children (TSU) established
• Hospital Skills Program (HSP) expanded with four new core units under development
• Building Future Leaders Program trained 22 potential leaders• Reviewed training in medical administration to develop a model
for training and career development• Rural Research Capacity Building Program
Workforce management • Increase in GP placement training sites for medical interns from four to 47
• Allocated one third of national intern training places• Specialist Training Program to address workforce distribution
and increase Aboriginal workforce participation rate• Supported rural rotations for training networks, increased rural
training places in Basic Physician Training and travel support for rural paediatric trainees
• Clinical medical supervision resource Superguide produced and distributed with similar guides for allied health and nursing and midwifery planned
• Supporting the rural workforce through 84 scholarships, sponsoring 30 clinicians to attend NSW Health Expo and employing an Aboriginal clerical trainee
• Working with Health Workforce Australia to expand training capacity
Flexibility, innovation and quality in learning
• Supporting the increasing use of simulation in training• Publishing online resources to support a range of training programs
and workforce development• Promoting evidence-based training in our collaboration with other
training bodies
• Developing e-learning standards to enhance online learning and training content and access
• Nursing Grand Rounds via videoconference enhances learning for 180 nurses
Improved standards in education and learning
• Providing access to the Teaching on the Run program (TOTR) enhancing doctor educator and supervision skills and training 21 new TOTR facilitators
• CETI’s leadership program for current and future clinical leaders trained 22 participants
• Working with RACP to improve standards of physician training service delivery
• Improving assessment training in the Hospital Skills Program and producing a DVD Assessment in Action
• Planning a Multi-Medical Supervisors Forum for second half of 2011• Staff capacity building that is providing enhanced education services
and learning support in the NSW Health system• Developing a learning management system (LMS) to support
increased online access to learning resources
Knowledge and knowledge management
• New supervision guide for doctors produced and work commenced on a supervision guide for allied health professionals
• New online e-education resources developed to support training programs and access to learning
• Developing e-standards for uploading resources
• CETI website development to promote access to resources and support
• Exploring web-based applications for rural access• Planning webpage for GP Procedural Training Program• New LinkedIn group for allied health professionals
Communication • Informing our stakeholders and seeking input via a range of media and opportunities eg website, forums. E-newsletter (cetiscape) and social media (Facebook, LinkedIn)
• Fostering wider communication through our collaborations, programs and resources
• Engaging Junior Medical Officers through quarterly JMO Forums
Collaboration • Working with the other health “pillars organisations” – CEC, ACI and BHI
• Collaborating with Medical Colleges and Fellowships on training programs
• Collaborating with Cancer Institute NSW on Basic Sciences in Oncology Course
• Collaborating with Local Health Districts in trainees allocations and research programs
• Collaborating with the Rural Doctors Network on training and research programs
• Working with Health Workforce Australia on workforce capacity and allocation
Overview of key achievements against goalsWe are working collaboratively with our stakeholders to support excellence in learning and training for workers in the NSW health system including training directed to non-traditional areas such as educational leadership, generalist hospital skills and medical administration, as well as supporting specialist training through professional Colleges.
We have produced a number of resources for teaching and learning and to support workforce capacity building. These resources include a guide for supervisors of medical trainees and a number of online course modules.
Future PlansOur success lies in strengthening education and training opportunities in NSW and supporting flexible learning. Our commitment to safe and accessible learning will see further investment in e-learning and synthetic learning environments. We plan to appoint the first Clinical Chair in Simulated Learning Environments to lead the strategic development of synthetic learning across NSW. While recognising the importance of blended learning, we will take on a new responsibility for e-learning across NSW and will collaborate with health services to support access to quality e-learning resources. We will be setting e-learning standards to support excellence in learning.
Supporting the workforce, improving learning opportunities and adding value to the NSW health system

GOAL KEY ACHIEVEMENTS
CETI > ANNUAL REPORT 2010/11 11
GOAL KEY ACHIEVEMENTS
Education and training supporting safe, multi-disciplinary, team-based patient-centred care
• Set up Team Health and interprofessional training modules• Called for expressions of interest to run interprofessional training
for new graduates under our Right Start program• Contributions to policy to enhance team-based care
• Review of induction process for international medical and nursing graduates
• Supporting rural team-based clinical improvement process• The Leadership and Management Essentials Program trained
31 from a range of disciplines over nine months
Professional development to build clinical skills, knowledge, competency and capacity
• New Allied Health Directorate established as a major initiative to promote training and learning resources for allied health professionals
• New Nursing and Midwifery Directorate established to support the training needs of nursing and midwifery
• GP Procedural Training Program supported 25 rural positions• Basic Physician Training (BPT) increased numbers and helped
achieve higher pass rates• Physician Education Program (PEP) by video and online assisted
192 trainees• Psychiatry education support by providing access to workshops
and developing resources with online access• Paediatrics professional qualities curriculum development• New online resources for emergency medicine trainees to help
prepare for exams
• Basic Sciences in Oncology Course (BSOC) reached 40 participants over 95 teaching sessions
• New Surgical Science Intensive Course developed for those not enrolled in the RACS Surgical Education and Training (SET)
• Training and Support Unit for Aboriginal Mothers, Babies and Children (TSU) established
• Hospital Skills Program (HSP) expanded with four new core units under development
• Building Future Leaders Program trained 22 potential leaders• Reviewed training in medical administration to develop a model
for training and career development• Rural Research Capacity Building Program
Workforce management • Increase in GP placement training sites for medical interns from four to 47
• Allocated one third of national intern training places• Specialist Training Program to address workforce distribution
and increase Aboriginal workforce participation rate• Supported rural rotations for training networks, increased rural
training places in Basic Physician Training and travel support for rural paediatric trainees
• Clinical medical supervision resource Superguide produced and distributed with similar guides for allied health and nursing and midwifery planned
• Supporting the rural workforce through 84 scholarships, sponsoring 30 clinicians to attend NSW Health Expo and employing an Aboriginal clerical trainee
• Working with Health Workforce Australia to expand training capacity
Flexibility, innovation and quality in learning
• Supporting the increasing use of simulation in training• Publishing online resources to support a range of training programs
and workforce development• Promoting evidence-based training in our collaboration with other
training bodies
• Developing e-learning standards to enhance online learning and training content and access
• Nursing Grand Rounds via videoconference enhances learning for 180 nurses
Improved standards in education and learning
• Providing access to the Teaching on the Run program (TOTR) enhancing doctor educator and supervision skills and training 21 new TOTR facilitators
• CETI’s leadership program for current and future clinical leaders trained 22 participants
• Working with RACP to improve standards of physician training service delivery
• Improving assessment training in the Hospital Skills Program and producing a DVD Assessment in Action
• Planning a Multi-Medical Supervisors Forum for second half of 2011• Staff capacity building that is providing enhanced education services
and learning support in the NSW Health system• Developing a learning management system (LMS) to support
increased online access to learning resources
Knowledge and knowledge management
• New supervision guide for doctors produced and work commenced on a supervision guide for allied health professionals
• New online e-education resources developed to support training programs and access to learning
• Developing e-standards for uploading resources
• CETI website development to promote access to resources and support
• Exploring web-based applications for rural access• Planning webpage for GP Procedural Training Program• New LinkedIn group for allied health professionals
Communication • Informing our stakeholders and seeking input via a range of media and opportunities eg website, forums. E-newsletter (cetiscape) and social media (Facebook, LinkedIn)
• Fostering wider communication through our collaborations, programs and resources
• Engaging Junior Medical Officers through quarterly JMO Forums
Collaboration • Working with the other health “pillars organisations” – CEC, ACI and BHI
• Collaborating with Medical Colleges and Fellowships on training programs
• Collaborating with Cancer Institute NSW on Basic Sciences in Oncology Course
• Collaborating with Local Health Districts in trainees allocations and research programs
• Collaborating with the Rural Doctors Network on training and research programs
• Working with Health Workforce Australia on workforce capacity and allocation
Overview of key achievements against goals
OVERVIEW12
1 Overview
Resources developedONLINE RESOURCES• Online learning management system
for the Basic Sciences in Oncology Course
• Online component for Psychotherapy Workshops
• Mental Illness in People with Intellectual Disability for Psychiatrists and Psychiatry Trainees
• Online component for Advanced Training Leadership and Management Tutorial Package for Psychiatrists
• Osteoporosis: joint project with the Agency for Clinical Innovation (ACI): online learning in development to improve detection and early management of osteoporosis by junior doctors
• Emergency medicine online Primary Exam preparation
• Emergency medicine NSW Fellowship examination preparation course. The e-learning resource for this course is intended to compliment the face to face teaching and provide access to trainees who are unable to attend. It has information for the weekly tutorials and practice sessions, an up to date timetable and contact details for the local convenors at each hospital site.
• Common urological emergencies• Managing minor burns
TRAINING MODULES• Advanced Training Leadership and
Management Tutorial Package for Psychiatrists
• Psychotherapy curriculum• Core Professional Skills for
Hospital Skills• Emergency Medicine for Hospital
Skills• Aged Care for Hospital Skills• Mental Health for Hospital Skills
PUBLICATIONS AND OTHER RESOURCES• The Doctor’s Compass – a guide to
prevocational training developed by the JMO Forum for junior doctors
• Superguide: a handbook for supervising doctors in training
• DVD Assessment in Action has been produced and distributed to all Network Directors of Hospital Training. This DVD demonstrates the use of MiniCEX as an assessment tool in history taking and physical examination scenarios.
• Positive Cardiometabolic Health: an early intervention framework for patient on psychotropic medication
REPORTS• Allied Health Clinical Education
and Training Future Directions Consultation Report – June 2011
• JMO Forum Report – May 2011• External Report on the Outcome
of the National Audit of Internship Acceptances Pilot Project Clinical Year 2011 – March 2011
• External Review of the Prevocational Training and Education Network System in NSW Final Report – November 2010
Articles for publication in peer reviewed journals• Better methods of assessing trainees
and evaluating the outcomes of training (Assessment research conducted by the Prevocational Training Council) – submitted to Medical Journal of Australia
• Overview of the Hospital Skills Program – submitted to Medical Journal of Australia
• Magin P, Adam J, Heading G, Pond D. Perfect Skin: the media and patients with skin disease: a qualitative study of patients with acne, psoriasis and atopic eczema. Australian Journal of Primary Health Vol. 17, 181-185, Jun 2011
• Luckett T, King MT, Butow PN, Oguchi M, Rankin N, Price MS, Heading G. Choosing between the EORTC QLQ-C30 and FACT-G for measuring health-related quality of life in cancer clinical research: issues, evidence and recommendations. Annals of Oncology Feb 2011
• Webster E, Thomas M, Ong N and Cutler L (2011) Rural Research Capacity Building Program: capacity building outcomes. Australian Journal of Primary Health, Vol. 17, No. 1, Mar 2011, 107-113
• Magin P, Heading G, Adams J, Pond D. Sex and the skin: a qualitative study of patients with acne, psoriasis and atopic eczema. Pyschology Health Med. Aug 15 (4): 454-462
• Luckett T, Butlow PN, King MT, Ogulich M, Heading G, Hackl NA, Rankin N, Price MA. A review and recommendations for optimal outcome measures in anxiety, depression and general distress in studies evaluating psychological interventions for English-speaking adults with heterogeneous cancer diagnoses. Supportive Care Cancer. Oct: 18(10): 1242-1262. Epub July 2, 2010
• Duncombe R (2011) Receptionists in Intake in Community Health. Australian Health Review, Vol. 35, No. 2, Jun 2011, 164-167 (from Rural Research Capacity Building project)
Publications and resources

CETI > ANNUAL REPORT 2010/11 13
• Occupational Therapy Australia 24th National Conference & Exhibition 2011 29 June – 1 July, Gold Coast (attended by Jacqueline Dominish)
• Team Health Consultation Forum, Sydney June 2011 (organised by CETI)
• CETI Allied Health Clinical Education and Training Future Directions Consultation Forum, Sydney June 2011 (Organised by CETI) – 31 participants including CETI staff with all 18 local health districts and specialty networks represented as well as the NSW Department of Health
• Emergency Medicine Inaugural Trainee Conference Day, Liverpool Hospital May 2011 (supported by CETI) – 60 participants
• Junior Medical Officer JMO Forums – held four times per year (organised by CETI). In 2010-2011 they were held September and December 2010, and March and May 2011
• Hospital Skills Program Forums, November 2010 and April 2011 (organised by CETI)
• 11th National Rural Health Conference, Perth March 2011 (27 rural clinicians supported to attend)
• Australasian Prevocational Forum, November 2010 (attended by Ros Crampton, Simon Willcock, Greg Keogh, Craig Bingham, Kirsten Campbell, Jeremiah Jacinto, representing CETI, and also by 4 CETI-sponsored JMOs – Dr Ricki Sayers, Dr Lucy Cho, Dr Matt Stanowski, Dr Hamish Dunn)
• 2nd NSW Rural and Remote Health Conference, Albury November 2010 (100 rural clinicians supported to attend)
• NSW Prevocational Forum, Sydney August 2010 (organised by CETI) attended by over 110 people involved in prevocational training (30 supported by CETI to attend)
Conferences/forums organised, supported or attended
JMO Forum March 2011
Allied Health Consultation Forum June 2011
OVERVIEW14
1 Overview
Our strategic plan
CETI is working to achieve our goals with the aid of a strategic plan to guide the development and outcomes of our programs and activities. A planning day was held in November 2010 which led to the current eight goals with associated operational plans. These eight goals are:
1. Education and training that supports safe, high quality, multi-disciplinary, team-based patient-centred care
2. Professional development and training to build clinical skills, knowledge, competency and capacity
3. Workforce management4. Flexibility, innovation and quality
in learning5. Improved standards in education
and training6. Knowledge and knowledge
management
7. Communication8. Collaboration
As part of our quality improvement, CETI will conduct an annual review of our strategic plan and continue to work on developing and strengthening our evaluation process.
In Section 2 of this report, information is provided about our programs and activities under each of these eight goals.
CETI > ANNUAL REPORT 2010/11 15
Overview of financial performance
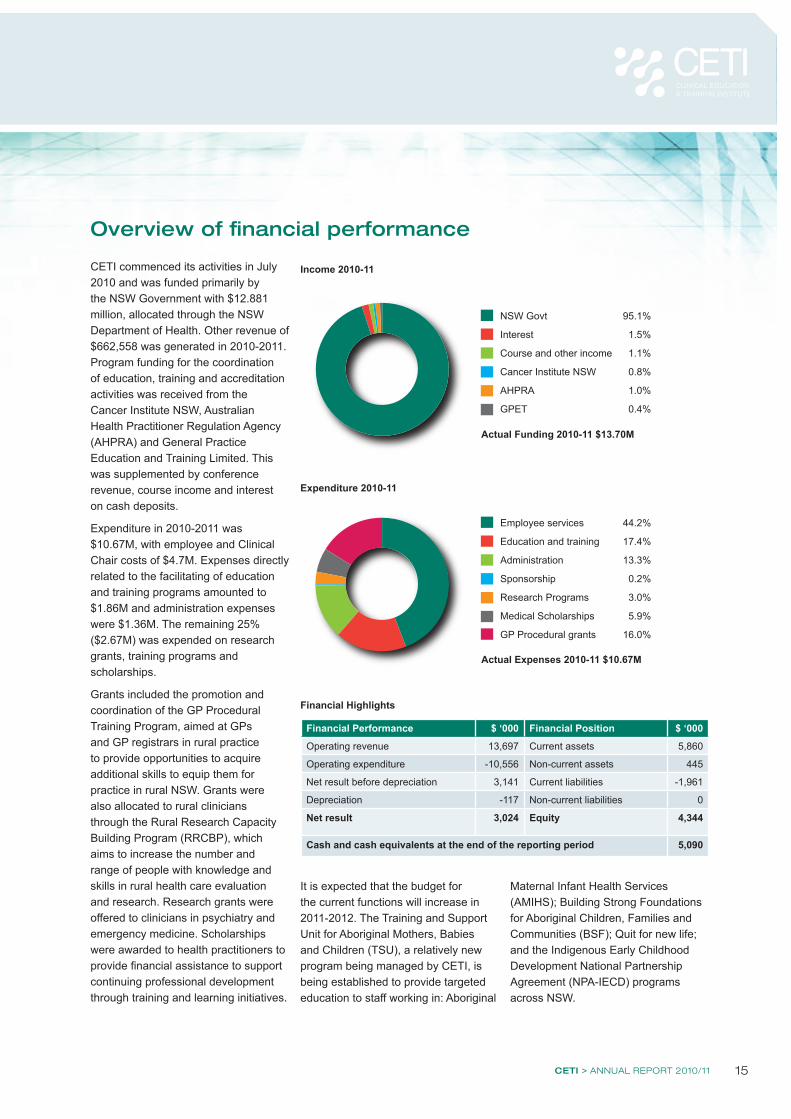
CETI commenced its activities in July 2010 and was funded primarily by the NSW Government with $12.881 million, allocated through the NSW Department of Health. Other revenue of $662,558 was generated in 2010-2011. Program funding for the coordination of education, training and accreditation activities was received from the Cancer Institute NSW, Australian Health Practitioner Regulation Agency (AHPRA) and General Practice Education and Training Limited. This was supplemented by conference revenue, course income and interest on cash deposits.
Expenditure in 2010-2011 was $10.67M, with employee and Clinical Chair costs of $4.7M. Expenses directly related to the facilitating of education and training programs amounted to $1.86M and administration expenses were $1.36M. The remaining 25% ($2.67M) was expended on research grants, training programs and scholarships.
Grants included the promotion and coordination of the GP Procedural Training Program, aimed at GPs and GP registrars in rural practice to provide opportunities to acquire additional skills to equip them for practice in rural NSW. Grants were also allocated to rural clinicians through the Rural Research Capacity Building Program (RRCBP), which aims to increase the number and range of people with knowledge and skills in rural health care evaluation and research. Research grants were offered to clinicians in psychiatry and emergency medicine. Scholarships were awarded to health practitioners to provide financial assistance to support continuing professional development through training and learning initiatives.
It is expected that the budget for the current functions will increase in 2011-2012. The Training and Support Unit for Aboriginal Mothers, Babies and Children (TSU), a relatively new program being managed by CETI, is being established to provide targeted education to staff working in: Aboriginal
Financial Performance $ ‘000 Financial Position $ ‘000
Operating revenue 13,697 Current assets 5,860
Operating expenditure -10,556 Non-current assets 445
Net result before depreciation 3,141 Current liabilities -1,961
Depreciation -117 Non-current liabilities 0
Net result 3,024 Equity 4,344
Cash and cash equivalents at the end of the reporting period 5,090
NSW Govt 95.1%
Interest 1.5%
Course and other income 1.1%
Cancer Institute NSW 0.8%
AHPRA 1.0%
GPET 0.4%
Actual Funding 2010-11 $13.70M
Employee services 44.2%
Education and training 17.4%
Administration 13.3%
Sponsorship 0.2%
Research Programs 3.0%
Medical Scholarships 5.9%
GP Procedural grants 16.0%
Actual Expenses 2010-11 $10.67M
Income 2010-11
Expenditure 2010-11
Financial Highlights
Maternal Infant Health Services (AMIHS); Building Strong Foundations for Aboriginal Children, Families and Communities (BSF); Quit for new life; and the Indigenous Early Childhood Development National Partnership Agreement (NPA-IECD) programs across NSW.

REPORT AGAINST OUR GOALS16
2 Report against our goals
The doctors, nurses and allied health professionals will need to replace the old system where different specialists would see the patient but no one person would necessarily take complete charge of the patient’s care. A new model of teamwork will be required to replace the old individual and independent “silos” of professional care. (Garling Report 1.25)
The fundamental goal of CETI is to assure that our health professionals are technically competent, well trained and able to work effectively as inter-professional teams.
As stated in the recent Global Commission Report of Health Professional Education:
“Redesign of professional health education is necessary and timely, in view of the opportunities for mutual learning and joint solutions offered by global interdependence due to acceleration of flows of knowledge, technologies, and financing across borders, and the migration of both professionals and patients.” (Frenk et al; Lancet, Nov 29, 2010)
• CETI is working to introduce team-based, patient-centred care and interprofessional collaborative practice through establishing our Team Health Program in May 2011. Team Health is:- Collaborating with tertiary education
providers and local health districts to design and implement programs to prepare pre-graduate health professionals for the workplace under the Right Start program.
Twenty-three expressions of interest were received and nine programs were funded
- Developing clinical team education modules for new and existing staff in different care settings including foundational team skills and empowering high performing teams
• CETI is providing feedback on health policies and implementation plans to reflect a team based interprofessional collaborative approach through setting up a policy review process with NSW Health
• We reviewed the induction process for international medical and nursing graduates to ensure that they understand the health context in NSW including responsibilities, values and working as a team
• The NSW Rural and Remote Clinical Team Leadership Program (CTLP) which commenced in 2009 aims to increase leadership and management skills in interprofessional team environment. The second intake which ran from August 2010 to June 2011 had 18 health professionals from NSW rural health services including three GP Visiting Medical Officers (VMOs) and one Staff Specialist. Participants completed six rural team based clinical practice improvement projects. The program involves collaboration with the Clinical Excellence Commission and NSW Rural Doctors Network
• The Leadership and Management Essentials Program (LMEP) is a nine month interprofessional program to develop leaders from a range of disciplines in rural areas. It includes leadership, management, self-governance and team governance Thirty one participants from rural and regional LHDs completed the program in 2010-2011
Goal 1: Education and training that supports safe, high quality, multi-disciplinary, team-based patient-centred care
CETI is working to introduce team-based, patient-centred care and interprofessional collaborative practice through establishing our Team Health Program

CETI > ANNUAL REPORT 2010/11 17
As part of our Right Start program to address the interprofessional capacities of pregraduate medical students, one of the key goals identified in the Garling Report, CETI is funding a number of training programs. One of these is ‘Get Ready’ - a training program under development to give students confidence in managing common medical emergencies in an interprofessional team environment. It is a collaborative effort between St Vincent’s Hospital Sydney, the University of New South Wales, The University of Sydney, Australian Catholic University and the University of Tasmania. “Fifty students, from medicine, nursing, nutrition, occupational therapy, physiotherapy, social work and speech pathology, will take part in a five day program during the course of their student placements at St Vincent’s Hospital,” explains Grainne O’Loughlin, Director Allied Health, St Vincent’s Hospital and “it will be great to see the benefits for patients and staff alike.”
CETI’s Team Health program, established in May 2011 in response to the Garling recommendation, is working to develop a suite of learning and teaching tools which build interprofessional collaborative practice amongst doctors, nurses, midwives and allied health professionals working in the public health system in New South Wales, for safer patient-centred care and better staff experiences.
After a consultation process with key stakeholders and in order to draw on the existing programs of work already underway, CETI invited Local Health Districts (in partnership with tertiary
education providers) to design and implement programs to prepare pre-graduate health professionals for a team based workplace. CETI received a total of 23 Expressions of Interest; with a total of nine programs funded to develop programs for pre-graduate health professionals starting work in 2012. One of the successful programs was the Get Ready program: A course for interprofessional work-place readiness in the health service.
Topics covered include roles and responsibilities, professionalism, communication skills and teamwork. Some aspects of the program will be delivered in a simulated learning environment, using scenario based training to develop students’ procedural skills, as well as skills in interdisciplinary teamwork. The program is set to run from 14 November 2011.
“We are very excited to be developing the program, which is in itself an interprofessional team exercise,” adds Grainne. “A number of the medical students taking part in the ‘Get Ready’ Program are set to join the hospital ranks as interns in 2012.”
St Vincent’s is also developing an interdisciplinary e-learning package to support the five day face-to-face program. The ‘Get Ready’ program will be evaluated, with a view to the program being included as part of the state-wide roll-out of Team Health in 2012.
“It will be great to see the benefits for patients and staff alike.”
Get Ready gets the interprofessional teamwork message out to pre-graduates
Fifty students from medicine, nursing, nutrition, occupational therapy, physiotherapy, social work and speech pathology will take part in a five day program during the course of their student placements at St Vincent’s Hospital
in focus
Grainne O’Loughlin
REPORT AGAINST OUR GOALS18
2 Report against our goals
The safety and quality of care provided to patients in public hospitals depends upon the skill of the whole hospital workforce which in turn depends upon how well they were trained before coming to the hospital, and how well they continue to be trained within the hospital after they join the staff. (Garling Report 1.61)
CETI works in partnership with a range of educational providers to build capacity in the health system for ongoing professional education and learning.• The GP Procedural Training Program
for skills to equip GPs to practice in rural NSW supported another 25 fulltime, part-time and flexible positions (285 since program commencement in 2003). A CETI convened stakeholder workshop held in April 2011 provided information to develop an operational plan and strategies to improve the overall coordination and management of the program, maximise the number of participants and enhance the
alignment of service and workshop planning for rural procedural GPs
• The Basic Physician Training (BPT) Networks Committee collaborated with the Royal Australasian College of Physicians (RACP) to enhance BPT, with five master classes conducted, trainee numbers increased by from 393 to 413, and pass rates significantly higher than national average. CETI successfully managed the 2011 BPT recruitment and intake. The number of rural and regional training positions in BPT networks increased from 56 in June 2010 to 65 in June 2011 – a 16% increase
• In 2011 CETI commenced supporting the Physician Education Program (PEP), a lecture series and clinical exam preparation sessions, as part of the BPT, delivered by video live to hospitals and available for viewing online. The lectures commenced in February 2011 with 192 trainees registered and the exam preparation sessions had 98 trainees registered
as at 30 June 2011. CETI is participating in a review of PEP with the RACP
• CETI’s Psychiatry education support has enabled the development of a number of resources such as an online component of the Psychotherapy Workshops, an online resource “Mental Illness in People with Intellectual Disability”, an Advanced Training Leadership and Management Tutorial Package with an online component, and a Psychotherapy Curriculum. Support has also been provided to assist state-wide access for trainees to attend workshops on subjects including cognitive behaviour therapy, psychotherapy, adult education techniques and strategies, communications skills, family therapy in the context of psychiatric disorders, critical analysis and research methodology, and an introduction to psychiatric epidemiology
• Emergency Medicine trainees have used CETI’s online education
Goal 2: Professional development and training to build clinical skills, knowledge, competency and capacity

CETI > ANNUAL REPORT 2010/11 19
resources, including study guide and interactive questions and answers for their Primary Examinations Preparation Course and the NSW Fellowship Examination Preparation course
• CETI administered the Basic Sciences in Oncology Course (BSOC) which teaches core skills and competencies in oncology covering anatomy, physics, biology and critical appraisal with links to clinical practice. In 2010 there were 40 participants and 95 teaching sessions. Five scholarships were awarded – three rural, two metropolitan. An online resource e-BSOC has also been developed to support participants
• CETI’s Surgical Skills Training Network undertook a number of new initiatives including a pilot of a Practical Professionalism Course which aims to improve the trainees understanding and application of non-clinical competencies as well as improve performance in the Royal Australasian College of Surgeons (RACS) Surgical Education and Training (SET) entry interviews
• CETI has developed a Surgical Science Intensive Course in conjunction with the University of Western Sydney to assist those on or seeking entry to the RACS program (General Surgery).The course was conducted in January / February 2011 with 21 participants attending for 10 teaching days comprising anatomy, physiology, pathology, pharmacology, radiology and assessments and has been submitted to RACS for accreditation
• The Clinical Surgical Training Council Trainee Subcommittee developed formal feedback forms to assess trainee progress, as well as a logbook to track management of conditions
and clinical skills practice. These forms will be piloted in Term Four 2011
• CETI is helping to close the gap by establishing a Training and Support Unit for Aboriginal Mothers, Babies and Children (TSU) to deliver a professional development program for staff of the Aboriginal Maternal and Infant Health Services (AMIHS) and Building Strong Foundations for Aboriginal Children, Families and Communities (BSF)
• CETI’s new Nursing and Midwifery Directorate has been established to support transition to practice, fill gaps and support resource development for nurses and midwives
• CETI continued its successful Hospital Skills Program (HSP) and held forums to provide professional development for directors of hospital training and education support officers and an opportunity for CMOs from across the state to train together. A working group is piloting a workplace-based assessment program for HSP participants. HSP curriculum modules being finalised include: core skills, aged care, mental health, and emergency department
• CETI is working to develop skilled medical administrators by participating in a review of their training needs to develop a sustainable model for training and career development. Extensive consultation has taken place which will form the basis of recommendations regarding training opportunities
• CETI’s Rural Research Capacity Building Program provided face-to-face training in research methods and project development. This investment impacts positively on service delivery as evidence drives practice
• CETI sponsored a trainee position in the Health NSW Biostatistician Training Program to focus on rural issues. This year’s studies have included an exploration of not waiting and discharging against medical advice at NSW Emergency Departments and an examination of misclassification of Triage 3 patients in NSW Emergency Departments
• CETI began building a program of core skills and interprofessional practice competencies for allied health professionals working in NSW hospitals. This new investment will for the first time provide training support for allied health professionals. A consultation forum of allied health representatives was held in June 2011 which provided input to the future directions of the Allied Health Directorate
The Clinical Surgical Training Council Trainee Subcommittee developed formal feedback forms to assess trainee progress, as well as a logbook to track management of conditions and clinical skills practice

REPORT AGAINST OUR GOALS20
2 Report against our goals
CETI’s Allied Health Directorate was established in 2011 in recognition of the fact that allied health practitioners are essential members of the clinical team but have historically been under-resourced regarding team support. According to Trish Bradd, Director of Allied Health for South Eastern Sydney Local Health District “we are hugely excited and enthusiastic to work with CETI and address the key issues for allied health. Education and training for skill and practice development promotes excellence in clinical care which in turn produces better patient outcomes. We are only just starting.”
There are many professions which are encompassed by the term ‘allied health’, each of which contributes a unique set of skills and interventions to the patient care journey. Allied health personnel have specialist knowledge in the identification, assessment, diagnosis, treatment and prevention of disease, disabilities and disorder across the healthcare spectrum.
As a Director of Allied Health since 2006 in the former South Eastern Sydney Illawarra Area Health Service, and with tertiary qualifications in speech pathology and management, Trish has over 22 years’ experience in the health care sector. She is familiar with the strengths and opportunities for the allied health profession and reflects that “for many years there has been a lack of dedicated resources to coordinate and think strategically about the education and training needs of allied health. Work in this domain has largely been conducted as an ‘add on’ to core business, occurring mainly at the local level and driven
by an enthusiasm and commitment to enhance skill and practice development by clinicians themselves. With the establishment of CETI and the Allied Health Directorate this is an exciting time for allied health and offers a wonderful opportunity to shape the future in new and innovative ways.”
While it is early days for this new directorate, Trish has had an opportunity to collaborate with CETI as chair of the NSW Health Allied Health Directors Network and as a member of the steering committee producing The Superguide: a handbook for supervising allied health professionals Steering Committee. She also attended the ‘Future Directions’ consultation forum in June 2011 which was held to identify priorities for allied health.
“It comes down to what you value and where you think you can make a difference. By collaborating with CETI and the Allied Health Directorate, I saw there was capacity for significant gains in promoting a skilled and educated allied health professional workforce in NSW Health. I look forward to further opportunities to collaborate with CETI into the future.”
Trish hopes that with the establishment of strong foundations in education and training, projects at a local level can complement, align with and springboard from the overall strategic direction for allied health education and training provided by CETI.
“I am looking forward to seeing greater allied health involvement in developing of new models of care and in arenas of extended scope of practice and interprofessional learning.”
Education and training for skill and practice development promotes excellence in clinical care which in turn produces better patient outcomes
in focus
Pamela Bloomfield and Trish Bradd
Allied Health – a key part of excellence in clinical care
CETI > ANNUAL REPORT 2010/11 21
Goal 3: Workforce management
CETI coordinates and integrates the support of a future workforce through a range of programs that build networks, supervision, and accreditation.
• CETI manages the allocation of medical intern applicants in NSW – one third of the total national intern places. Intern applicants are allocated to prevocational training networks to maximise applicant preferences and ensure equitable workforce distribution especially in rural and regional areas. A total of 770 prevocational training places were accepted in 2011 with two places allocated to the Building Capacity in the Aboriginal Medical Workforce program. CETI identified 790 emergency term rotations in NSW ensuring each intern had an opportunity to complete an emergency term
• In collaboration with the Commonwealth Department of Health and Ageing (DoHA) CETI processed applications for the 2012 Specialist Training Program (STP) providing new registrar training posts. The program addresses priorities related to workforce maldistribution, increases the specialist workforce in rural and regional areas and increases the Aboriginal workforce participation rate
• CETI works to ensure rural and regional training network placements are supported by including rural rotations in networked training programs. Basic Physician Training (BPT) had a 16% increase during the year for rural and regional places. To support Paediatrics trainees, funds are provided for travel back to Sydney
• CETI is building the capacity of those who provide clinical supervision of prevocational trainees by producing The Superguide: a handbook for supervising doctors in training. This resource provides the model for similar guides for supervisors of allied health and nursing and midwifery staff requiring supervision
• CETI is supporting the rural workforce through a number of programs: - The Rural Medical Scholarship
program provided 84 scholarships totalling $89,316 in 2010/11 to encourage prevocational trainees and basic and advanced trainees in CETI networked training programs to work in rural areas
- CETI sponsored 30 rural and remote clinicians in 2010 to attend the NSW Health Expo and Awards to gain exposure to quality innovations and models of care
- CETI’s Rural Directorate employs an Aboriginal clerical trainee on an annual basis
• CETI is working with Health Workforce Australia (HWA) on the Clinical Training Reform Work Group to prepare for the roll out of the following programs:- Integrated Regional Clinical Training
Networks project to expand the capacity of clinical training through better organisation at national, jurisdictional and regional levels
- Clinical Training Funding program to expand the clinical training capacity and address workforce shortages through subsidised training places for medical and health professional students across 22 disciplines
- Clinical Supervision Support program to enhance the supervision capacity and competence of professional entry, post-graduate and vocational trainee students including allied health, dental, medical, nursing and midwifery by funding supervision training support models and resources
• Medical Graduates Prevocational Training Program increased general practice placement training sites from four to 47 and hospital training sites from 51 to 53 with 28 hospital accreditations completed during the year. The increase in GP training sites was achieved with the pilot of a new provisional accreditation model. The model provides a high level of streamlining compared to hospital accreditation processes, but remains robust to ensure the safety of both junior doctors and patients. The accreditation model is a unique response to the general practice prevocational training context and has successfully enabled accreditation of an additional 43 general practices and six Regional Training Providers. An evaluation of the pilot was undertaken which indicated that trainee experiences were highly positive
• CETI has successfully developed key relationships with Regional Training Providers, who provide leadership and governance of the PGPPP education and training programs
CETI works to ensure rural and regional training network placements are supported by including rural rotations in networked training programs

REPORT AGAINST OUR GOALS22
2 Report against our goals
CETI’s Prevocational General Practice Placements Program (PGPPP) provides prevocational medical trainees with opportunities to encounter a different range of clinical training experiences in a primary health care setting outside the traditional hospital environment. It exposes trainees to the kinds of common healthcare problems that they would not encounter in a hospital setting, including the care of chronic physical and mental illness, the very young and old and those with multiple comorbidities. According to Sharon Flynn, Chief Executive of Coast City Country General Practice Training, a regional training provider, “doctors who have completed PGPPP rotations talk of the greater confidence they have on their return to complete their in-hospital rotations.”
Feedback from trainees indicates that these placements are an invaluable addition to their prevocational training experience. A recent evaluation indicated that 100% of trainees would recommend the placement to their colleagues and 67% rated their skills and confidence as a doctor as ‘significantly improved’ by the experience.
The placements are supported by a collaborative relationship between a feeder hospital, who releases the trainee, a regional training provider that provides governance and leadership of the program, and a general practice, which provides the clinical experience and training. CETI has focused on acknowledging and supporting these collaborations, which are unique to this setting.
The program has provided a significant expansion to the training settings available to prevocational trainees. Coast City Country General Practice Training has seen the number of
prevocational general practice placements they offer increase from a single practice in 2008 to 17 in 2011, with more to be added next year.
According to Sharon Flynn, “we are also experiencing an increase in the number of junior doctors choosing networks because of the availability of our rural and regional PGPPP posts.” She noted that “perhaps the most telling measure of the success of the program is the stories.” One such story comes from Dr Barbara Cameron, a prevocational trainee in her first year after graduation, who remarks: “I found this placement extremely fulfilling. I would strongly recommend a PGPPP term during internship to any doctor and particularly to those interested in a possible career in general practice.”
Another key to success has been CETI’s ability to accredit GP practices and regional training providers to take the placements. In 2010 CETI piloted a new provisional accreditation model in response to almost 50 practices seeking accreditation in a short space of time. The model provides a high level of streamlining compared to hospital accreditation processes, but remains robust to ensure the safety
of both junior doctors and patients. The model has a number of distinctive attributes:• General practices already holding
accreditation with the RACGP or ACRRM can avoid the need for an initial site visit. This significantly reduces the time required to complete provisional accreditation
• The leadership and governance role of the regional training providers is recognised by requiring these organisations also to be accredited
• A collaborative agreement forms the basis of a partnership between the regional training provider, a feeder hospital and the general practice in the delivery of the education and training program
CETI’s accreditation model is a unique response to the general practice prevocational training context and has successfully enabled the accreditation of an additional 43 general practices and six regional training providers.
The PGPPP is a Commonwealth funded program and is being undertaken in close partnership with General Practice Education and Training (GPET).
Prevocational General Practice Placements Program – a new training experience not just for potential GPs
Collaborative team for PGPPP in Wagga Wagga (left to right): Dr Gary Yang (Prevocational Trainee), Dr Mir Musaul Tarique (Prevocational Trainee), Dr Peter English (Coast City Country PGPPP Medical Educator), Ms Sharon Flynn (Coast City Country, CEO), Dr Andrew Cumberlege (DPET, Wagga Wagga Base Hospital), Dr Barbara Cameron (Prevocational Trainee), Dr Murray Schofield (Prevocational Trainee)

CETI > ANNUAL REPORT 2010/11 23
Dr Martin Mackertich
NSW intern allocation: managing training places and rural needs
One of CETI’s important strategic roles is to manage the allocation of graduates to places in training networks in NSW - a third of all intern places in Australia. The challenge for CETI is not only to assist as many graduates as possible to start their prevocational training but also to help build a sustainable workforce in rural and regional areas where attracting and retaining staff can be a significant issue.
CETI is the first allocation body in Australia to implement a fully electronic allocation process, with applicants applying for internships through a unique online system known as the Prevocational Training Allocation Program (PTAP). This system allows graduates to upload all of their documentation and receive an immediate confirmation that it has been received and assists CETI to manage the allocation process more efficiently.
To attract graduates to rural and regional areas, special pathways have been established that allow priority allocations before the main round. These pathways include:• Rural preferential recruitment where
graduates can apply directly to rural hospitals and participate in a merit based selection process. Numbers have increased from 15 in 2007 to 80 for 2012
• Building capacity in the Aboriginal medical workforce, which is aligned with the national “Closing the Gap” in Aboriginal health care outcomes agreement, allows placement of Aboriginal medical graduates into hospitals or networks with access to support and mentoring. Almost 50% of Aboriginal graduates so far have taken this pathway
• Regional preferential allocation where graduates are allocated before the main round of allocation. Under this pathway the number of trainee doctors allocated to regional hospitals increased by 50% for 2012
According to Dr Martin Mackertich, Chair of the Prevocational Workforce Advisory Committee “it’s important to have this flexibility because we know that undertaking your internship in a location that meets both your personal and career needs is one of the best indicators for success in your prevocational years.”
The allocation process for the clinical year 2012 commenced in March 2011, with 846 positions to fill across 15 prevocational training networks.
In 2010 CETI introduced a series of presentations to medical students in their final year. In early 2011 this included presentations at the rural clinical schools as well. A significant
amount of information is also now provided online, including relevant dates, policies and procedures, with the site being accessed 4800 times in regard to the 2012 allocation. These innovations have made the process easier for all potential medical interns and also helped contribute to the uptake of the regional preferential allocation.
Dr Mackertich added that “the Committee’s main focus at the moment is in working with other sectors of the system to ensure that not only is there an equitable distribution of the increasing numbers of medical graduates across the system based on clinical demand, but that all NSW graduates continue to have access to good training opportunities.”
This program of work is a significant contribution to the task of building a high quality and sustainable medical workforce for all the people of NSW.
Programs in each Clinical Year Positions Offered
2011
Positions Accepted
2011
Positions Offered
2012
Positions Accepted
2012
Rural Preferential Recruitment 81 61 89 80
Regional Preferential Allocation 78 70 144 144
Building Capacity Aboriginal Medical Workforce Program
2 2 3 3
General Allocation 637 619
Total 770 846
in focus
Table 1 – Number of prevocational training positions recruited to and allocated in NSW as at 30 June 2011 (note that the 2012 allocation process was not complete at that date)
CETI allocates a third of all intern places in Australia

REPORT AGAINST OUR GOALS24
2 Report against our goals
CETI leads the way in using new technology to deliver education and learning to the health professions. It has created a new directorate of Learning Innovation and Future Technology (LIFT) to progress e-learning, blended learning, learning management systems and simulation.
• CETI is working to increase the use of simulation in learning. We have appointed our first Simulation Coordinator to support development of this initiative and plan to appoint a Chair of Simulated Learning Environments
• CETI promotes evidence-based training in our production of resources and our collaboration with training networks and programs, Colleges
and Fellowships, universities and research capacity building program
• CETI is conducting an analysis of e-learning standards to be disseminated in October / November 2011
• Using technology to support learning, CETI has established a number of resources that are available online across a range of programs to enable more flexible and cost effective access to learning
• Nursing Grand Rounds is a rural program using video conferencing as an innovative way to enable shared learning for rural and remote nurses with six out of seven rural LHDs participating linking 160 nurses each month
Goal 4: Flexibility, innovation and quality in learning
CETI has appointed our first Simulation Coordinator to support the development of simulation in learning
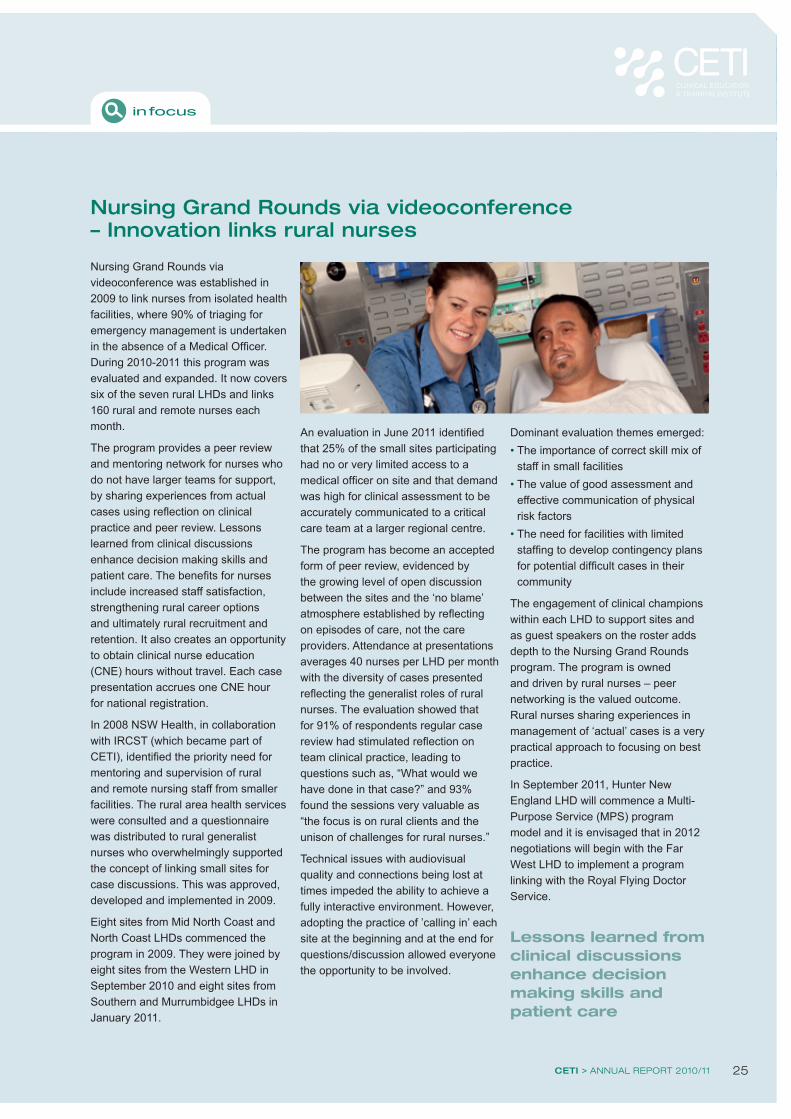
CETI > ANNUAL REPORT 2010/11 25
Nursing Grand Rounds via videoconference was established in 2009 to link nurses from isolated health facilities, where 90% of triaging for emergency management is undertaken in the absence of a Medical Officer. During 2010-2011 this program was evaluated and expanded. It now covers six of the seven rural LHDs and links 160 rural and remote nurses each month.
The program provides a peer review and mentoring network for nurses who do not have larger teams for support, by sharing experiences from actual cases using reflection on clinical practice and peer review. Lessons learned from clinical discussions enhance decision making skills and patient care. The benefits for nurses include increased staff satisfaction, strengthening rural career options and ultimately rural recruitment and retention. It also creates an opportunity to obtain clinical nurse education (CNE) hours without travel. Each case presentation accrues one CNE hour for national registration.
In 2008 NSW Health, in collaboration with IRCST (which became part of CETI), identified the priority need for mentoring and supervision of rural and remote nursing staff from smaller facilities. The rural area health services were consulted and a questionnaire was distributed to rural generalist nurses who overwhelmingly supported the concept of linking small sites for case discussions. This was approved, developed and implemented in 2009.
Eight sites from Mid North Coast and North Coast LHDs commenced the program in 2009. They were joined by eight sites from the Western LHD in September 2010 and eight sites from Southern and Murrumbidgee LHDs in January 2011.
An evaluation in June 2011 identified that 25% of the small sites participating had no or very limited access to a medical officer on site and that demand was high for clinical assessment to be accurately communicated to a critical care team at a larger regional centre.
The program has become an accepted form of peer review, evidenced by the growing level of open discussion between the sites and the ‘no blame’ atmosphere established by reflecting on episodes of care, not the care providers. Attendance at presentations averages 40 nurses per LHD per month with the diversity of cases presented reflecting the generalist roles of rural nurses. The evaluation showed that for 91% of respondents regular case review had stimulated reflection on team clinical practice, leading to questions such as, “What would we have done in that case?” and 93% found the sessions very valuable as “the focus is on rural clients and the unison of challenges for rural nurses.”
Technical issues with audiovisual quality and connections being lost at times impeded the ability to achieve a fully interactive environment. However, adopting the practice of ’calling in’ each site at the beginning and at the end for questions/discussion allowed everyone the opportunity to be involved.
Dominant evaluation themes emerged:• The importance of correct skill mix of
staff in small facilities• The value of good assessment and
effective communication of physical risk factors
• The need for facilities with limited staffing to develop contingency plans for potential difficult cases in their community
The engagement of clinical champions within each LHD to support sites and as guest speakers on the roster adds depth to the Nursing Grand Rounds program. The program is owned and driven by rural nurses – peer networking is the valued outcome. Rural nurses sharing experiences in management of ‘actual’ cases is a very practical approach to focusing on best practice.
In September 2011, Hunter New England LHD will commence a Multi-Purpose Service (MPS) program model and it is envisaged that in 2012 negotiations will begin with the Far West LHD to implement a program linking with the Royal Flying Doctor Service.
Nursing Grand Rounds via videoconference – Innovation links rural nurses
in focus
Lessons learned from clinical discussions enhance decision making skills and patient care
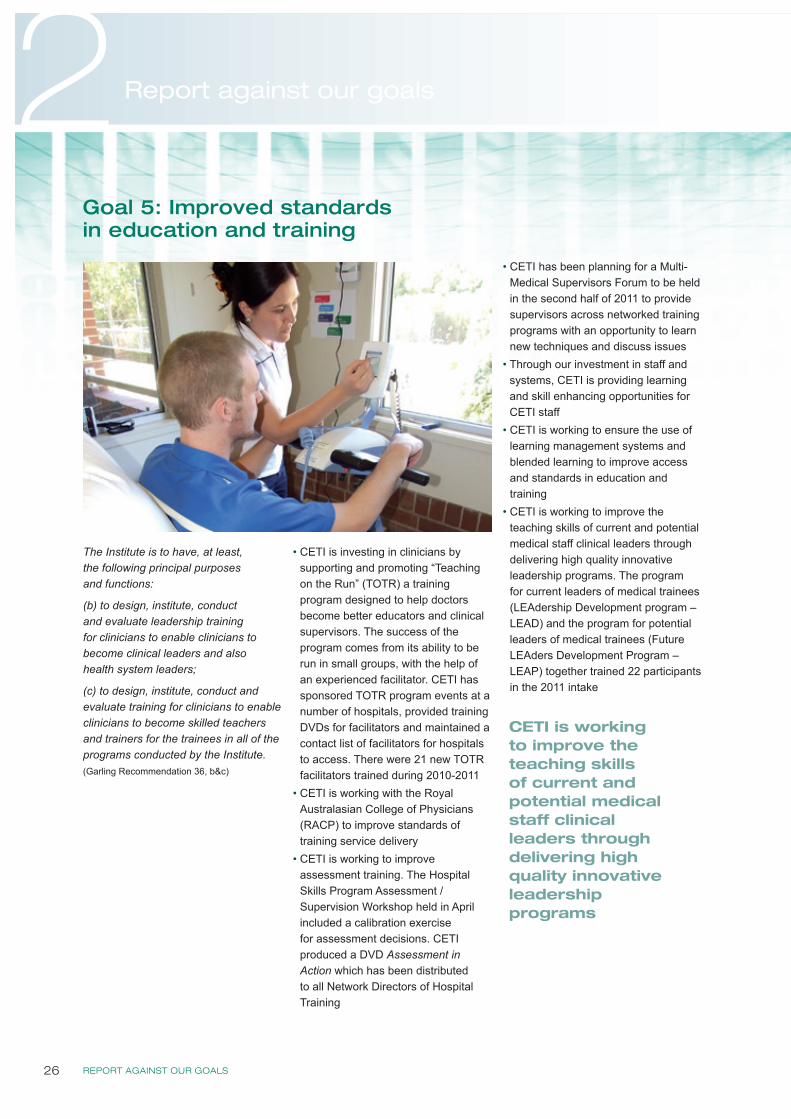
REPORT AGAINST OUR GOALS26
2 Report against our goals
The Institute is to have, at least, the following principal purposes and functions:
(b) to design, institute, conduct and evaluate leadership training for clinicians to enable clinicians to become clinical leaders and also health system leaders;
(c) to design, institute, conduct and evaluate training for clinicians to enable clinicians to become skilled teachers and trainers for the trainees in all of the programs conducted by the Institute. (Garling Recommendation 36, b&c)
• CETI is investing in clinicians by supporting and promoting “Teaching on the Run” (TOTR) a training program designed to help doctors become better educators and clinical supervisors. The success of the program comes from its ability to be run in small groups, with the help of an experienced facilitator. CETI has sponsored TOTR program events at a number of hospitals, provided training DVDs for facilitators and maintained a contact list of facilitators for hospitals to access. There were 21 new TOTR facilitators trained during 2010-2011
• CETI is working with the Royal Australasian College of Physicians (RACP) to improve standards of training service delivery
• CETI is working to improve assessment training. The Hospital Skills Program Assessment / Supervision Workshop held in April included a calibration exercise for assessment decisions. CETI produced a DVD Assessment in Action which has been distributed to all Network Directors of Hospital Training
• CETI has been planning for a Multi-Medical Supervisors Forum to be held in the second half of 2011 to provide supervisors across networked training programs with an opportunity to learn new techniques and discuss issues
• Through our investment in staff and systems, CETI is providing learning and skill enhancing opportunities for CETI staff
• CETI is working to ensure the use of learning management systems and blended learning to improve access and standards in education and training
• CETI is working to improve the teaching skills of current and potential medical staff clinical leaders through delivering high quality innovative leadership programs. The program for current leaders of medical trainees (LEAdership Development program – LEAD) and the program for potential leaders of medical trainees (Future LEAders Development Program – LEAP) together trained 22 participants in the 2011 intake
Goal 5: Improved standards in education and training
CETI is working to improve the teaching skills of current and potential medical staff clinical leaders through delivering high quality innovative leadership programs

CETI > ANNUAL REPORT 2010/11 27
CETI’s strategy to achieve improved standards in education and training is being realised in the Leadership Development Program (LEAD) and the Future Leaders Development Program (LEAP) which deliver an innovative, interactive and inspirational trainee leadership program for current and future clinician leaders in medical education and training within the NSW Health system. Dr Chamindra Wijeratne, a previous program participant and Anaesthetic Senior Resident Medical Officer Concord Hospital, noted that “the skills gained have played an invaluable part in my efforts to improve medical training and education in NSW.”
Traditional teaching methods in medical education and training have focused on the diagnosis and treatment of medical conditions. According to Dr Emma McCahon, Chair of the Paediatric Physician Training Council and Clinical Chair of CETI’s Future Leaders Program, “whilst clinical skills are clearly important, the importance of nontechnical skills such as communication, conflict resolution and negotiation are becoming more recognised. These skills are particularly pertinent in designing, implementing and running clinical education within the health system.” Dr McCahon comments that with CETI’s Future Leaders Development program “trainees and clinicians get a chance to look at what it actually means to be a leader in medical education and training.”
Following a 2009 LEAP pilot program, the LEAD program for consultants was added in 2010. In 2011 the programs were run jointly with 22 participants. One of the benefits was the clinical consultants on the program enriching the content for the trainees with their experience. Since 2009 there have been over 45 participants who now hold leadership roles and are influencing medical education in the NSW health system.
The programs consist of five workshops, three projects undertaken in groups and workplace-based experience. There is a strong focus on medical education and training, drawing on the participant’s experience and faculty experience in the health and corporate sector. The participants are challenged to develop and apply their skills both in the workshops and in their workplace.
Dr Wijeratne adds “most of the ideas that have been developed by participants are now being implemented in NSW Health at various levels, and I have no doubt that this is only the beginning of the contribution by these leaders in medical education and training in NSW.”
One idea being implemented is the Clinical Acquisition of Procedural Skills (CAPS) program piloted at Westmead Hospital. The aim of the program was to assist junior medical staff in the clinical acquisition of procedural skills. This program was designed, championed and implemented by junior doctors who saw a gap in the system as an opportunity.
An important objective of CETI is that modern learning theories and adult learning principles should be reflected in the design and delivery of curriculum, courses and learning materials for health professionals, as evident in the LEAP and LEAD programs. “Participants have an opportunity to develop skills through collegiate learning and by engaging in interactive workshops, group discussions and self-reflection” explains Dr McCahon. These skills are complemented and further developed by self-directed and web-based learning, a mentor program and practical leadership experience in the workplace.
Improving standards in health education and training by developing clinical leaders
Participants who now hold leadership roles are influencing medical education in the NSW health system
Dr Chaminda Wijeratne Dr Emma McCahon teaching on the 2010 Leadership Development Program
Developing Clinical Leaders
in focus
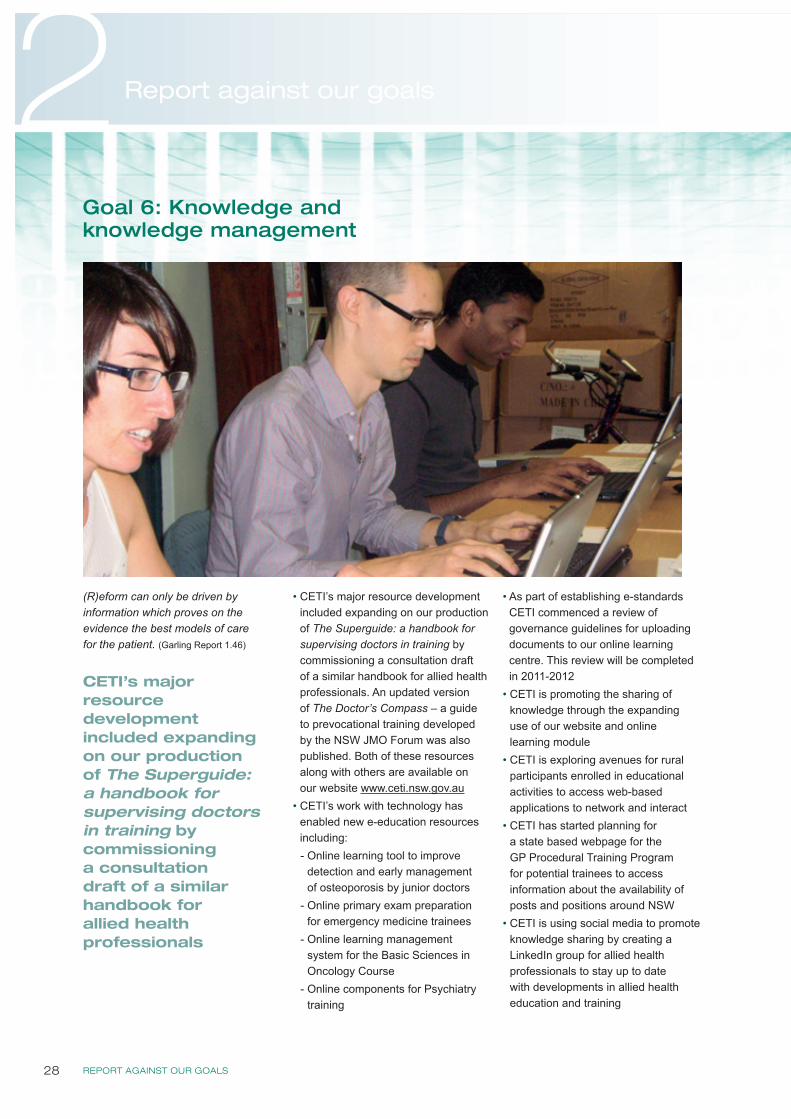
REPORT AGAINST OUR GOALS28
2 Report against our goals
(R)eform can only be driven by information which proves on the evidence the best models of care for the patient. (Garling Report 1.46)
• CETI’s major resource development included expanding on our production of The Superguide: a handbook for supervising doctors in training by commissioning a consultation draft of a similar handbook for allied health professionals. An updated version of The Doctor’s Compass – a guide to prevocational training developed by the NSW JMO Forum was also published. Both of these resources along with others are available on our website www.ceti.nsw.gov.au
• CETI’s work with technology has enabled new e-education resources including:- Online learning tool to improve
detection and early management of osteoporosis by junior doctors
- Online primary exam preparation for emergency medicine trainees
- Online learning management system for the Basic Sciences in Oncology Course
- Online components for Psychiatry training
• As part of establishing e-standards CETI commenced a review of governance guidelines for uploading documents to our online learning centre. This review will be completed in 2011-2012
• CETI is promoting the sharing of knowledge through the expanding use of our website and online learning module
• CETI is exploring avenues for rural participants enrolled in educational activities to access web-based applications to network and interact
• CETI has started planning for a state based webpage for the GP Procedural Training Program for potential trainees to access information about the availability of posts and positions around NSW
• CETI is using social media to promote knowledge sharing by creating a LinkedIn group for allied health professionals to stay up to date with developments in allied health education and training
Goal 6: Knowledge and knowledge management
CETI’s major resource development included expanding on our production of The Superguide: a handbook for supervising doctors in training by commissioning a consultation draft of a similar handbook for allied health professionals
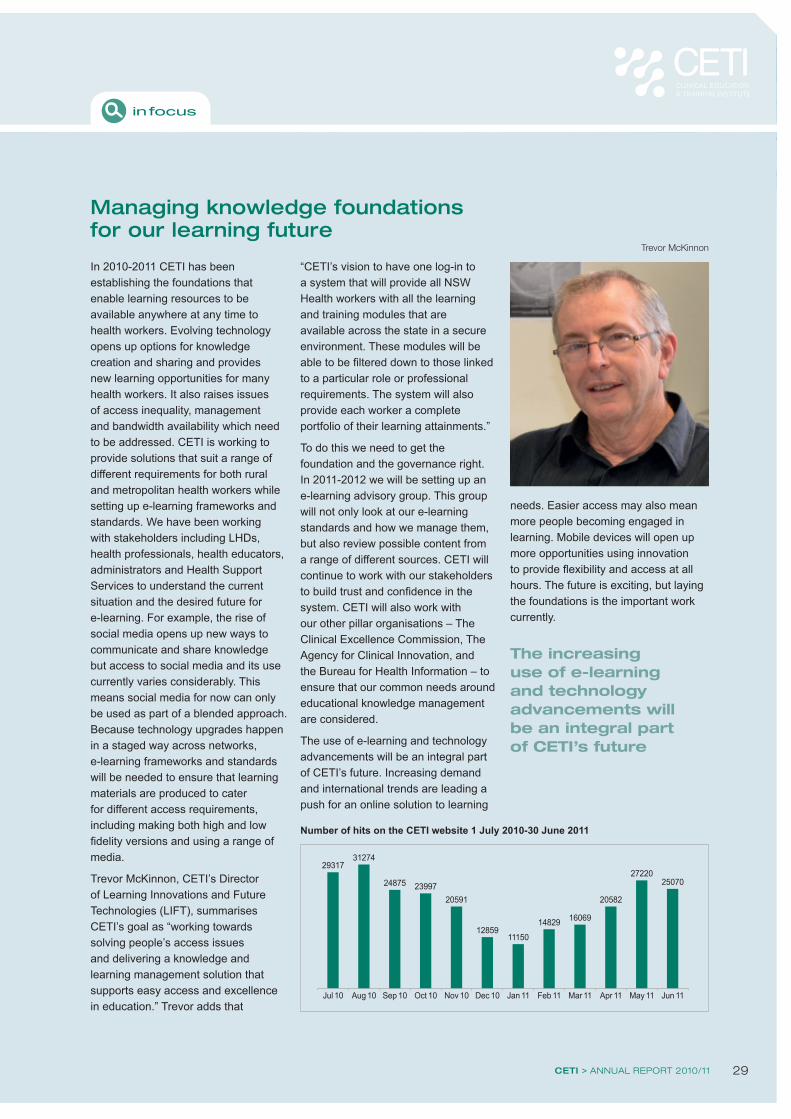
CETI > ANNUAL REPORT 2010/11 29
In 2010-2011 CETI has been establishing the foundations that enable learning resources to be available anywhere at any time to health workers. Evolving technology opens up options for knowledge creation and sharing and provides new learning opportunities for many health workers. It also raises issues of access inequality, management and bandwidth availability which need to be addressed. CETI is working to provide solutions that suit a range of different requirements for both rural and metropolitan health workers while setting up e-learning frameworks and standards. We have been working with stakeholders including LHDs, health professionals, health educators, administrators and Health Support Services to understand the current situation and the desired future for e-learning. For example, the rise of social media opens up new ways to communicate and share knowledge but access to social media and its use currently varies considerably. This means social media for now can only be used as part of a blended approach. Because technology upgrades happen in a staged way across networks, e-learning frameworks and standards will be needed to ensure that learning materials are produced to cater for different access requirements, including making both high and low fidelity versions and using a range of media.
Trevor McKinnon, CETI’s Director of Learning Innovations and Future Technologies (LIFT), summarises CETI’s goal as “working towards solving people’s access issues and delivering a knowledge and learning management solution that supports easy access and excellence in education.” Trevor adds that
“CETI’s vision to have one log-in to a system that will provide all NSW Health workers with all the learning and training modules that are available across the state in a secure environment. These modules will be able to be filtered down to those linked to a particular role or professional requirements. The system will also provide each worker a complete portfolio of their learning attainments.”
To do this we need to get the foundation and the governance right. In 2011-2012 we will be setting up an e-learning advisory group. This group will not only look at our e-learning standards and how we manage them, but also review possible content from a range of different sources. CETI will continue to work with our stakeholders to build trust and confidence in the system. CETI will also work with our other pillar organisations – The Clinical Excellence Commission, The Agency for Clinical Innovation, and the Bureau for Health Information – to ensure that our common needs around educational knowledge management are considered.
The use of e-learning and technology advancements will be an integral part of CETI’s future. Increasing demand and international trends are leading a push for an online solution to learning
needs. Easier access may also mean more people becoming engaged in learning. Mobile devices will open up more opportunities using innovation to provide flexibility and access at all hours. The future is exciting, but laying the foundations is the important work currently.
Managing knowledge foundations for our learning future
Trevor McKinnon
in focus
Jul 10
29317
Aug 10
31274
Sep 10
24875
Oct 10
23997
Nov 10
20591
Dec 10
12859
Jan 11
11150
Feb 11
14829
Mar 11
16069
Apr 11
20582
May 11
27220
Jun 11
25070
Number of hits on the CETI website 1 July 2010-30 June 2011
The increasing use of e-learning and technology advancements will be an integral part of CETI’s future
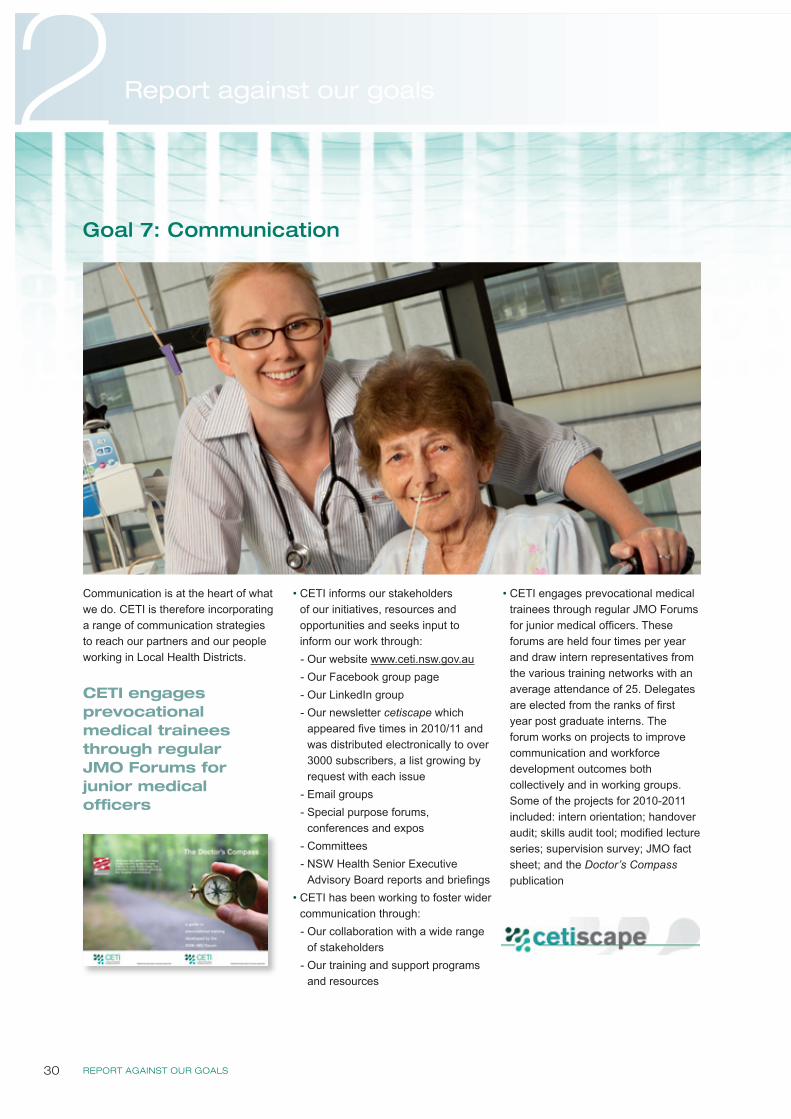
REPORT AGAINST OUR GOALS30
2 Report against our goals
Communication is at the heart of what we do. CETI is therefore incorporating a range of communication strategies to reach our partners and our people working in Local Health Districts.
• CETI informs our stakeholders of our initiatives, resources and opportunities and seeks input to inform our work through:- Our website www.ceti.nsw.gov.au- Our Facebook group page- Our LinkedIn group - Our newsletter cetiscape which
appeared five times in 2010/11 and was distributed electronically to over 3000 subscribers, a list growing by request with each issue
- Email groups- Special purpose forums,
conferences and expos- Committees- NSW Health Senior Executive
Advisory Board reports and briefings • CETI has been working to foster wider
communication through:- Our collaboration with a wide range
of stakeholders- Our training and support programs
and resources
• CETI engages prevocational medical trainees through regular JMO Forums for junior medical officers. These forums are held four times per year and draw intern representatives from the various training networks with an average attendance of 25. Delegates are elected from the ranks of first year post graduate interns. The forum works on projects to improve communication and workforce development outcomes both collectively and in working groups. Some of the projects for 2010-2011 included: intern orientation; handover audit; skills audit tool; modified lecture series; supervision survey; JMO fact sheet; and the Doctor’s Compass publication
Goal 7: Communication
CETI engages prevocational medical trainees through regular JMO Forums for junior medical officers

CETI > ANNUAL REPORT 2010/11 31
CETI’s work is helping to improve communication in the hospital environment, which is often the key
to improving patient care. In 2009 the Health Services Performance Improvement Branch (HSPIB) of NSW Health began work on a Safe Clinical Handover project to improve the communication of patient information at transitions in the health system. In 2010 the project focused on the handover of patients between junior medical officers (JMOs) at shift changes, a crucial moment when a failure of communications can have adverse effects on patient care. The CETI JMO Forum has enabled JMOs to come up with solutions by emphasising the educational opportunities handover provides.
The JMO Forum, CETI’s advisory committee of prevocational medical trainees includes interns and residents from the 15 prevocational training networks. It helps connect CETI to the networks, and provides a channel for communication and creative collaboration between clinicians and change agencies in the health system. It is a good example of CETI’s collaborative way of working: connecting clinicians, administrators and educators for workforce development to improve patient care. CETI contributed to the Safe Clinical Handover project by connecting the HSPIB taskforce with the JMO Forum.
Dr Hamish Dunn, a resident medical officer at Hornsby Hospital was one of a small group who volunteered to give essential JMO input. “Our JMO
group was made a core component of the project team, and we could offer advice on what JMOs needed to make handover work well,” says Hamish. HSPIB Principal Project Officer Ian Richards agrees: “The project benefited greatly by having JMOs from a range of networks representing their peers in all phases of development. Their hard work and creative input gives us confidence that the project is relevant to and meets the needs of newly graduated medical officers.”
The JMO Forum group emphasised the role of senior clinicians and the educational opportunities at shift handover, knowing that making handover educational would help to make it happen.
“Working with CETI’s JMO Forum has given us an opportunity to contribute to the health of the healthcare system,” says Hamish. “As a JMO, you are usually immersed in the day-to-day round of patient care – which is great. But junior doctors can offer a unique way of looking at the health system, and it’s refreshing to step back sometimes to consider the system as a whole, and the ways we might do things better.”
Making handover educational helps communication
Working with CETI’s JMO Forum gives junior medical officers an opportunity to contribute to the health of the healthcare system
Dr Hamish Dunn
JMO Forum September 2010
Dr Amanda Brownlow and Dr Ricki Sayers, JMO Forum Chairs 2010 and 2011
in focus
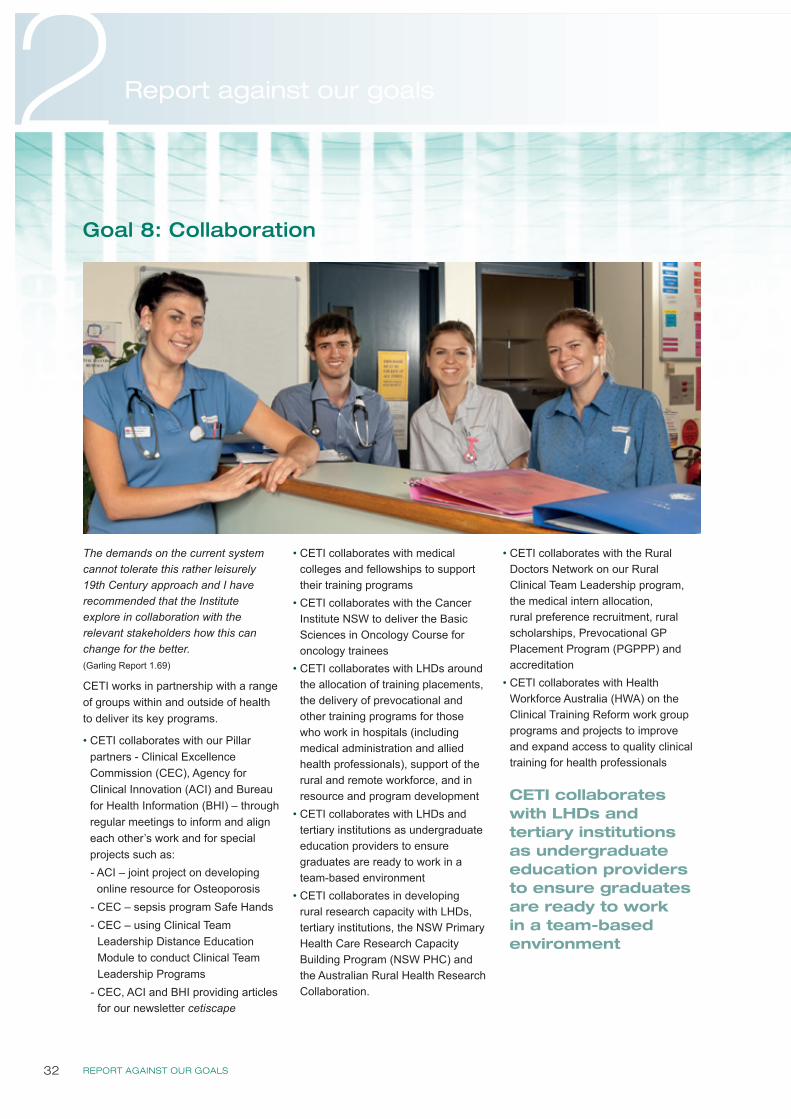
REPORT AGAINST OUR GOALS32
2 Report against our goals
The demands on the current system cannot tolerate this rather leisurely 19th Century approach and I have recommended that the Institute explore in collaboration with the relevant stakeholders how this can change for the better. (Garling Report 1.69)
CETI works in partnership with a range of groups within and outside of health to deliver its key programs.
• CETI collaborates with our Pillar partners - Clinical Excellence Commission (CEC), Agency for Clinical Innovation (ACI) and Bureau for Health Information (BHI) – through regular meetings to inform and align each other’s work and for special projects such as:- ACI – joint project on developing online resource for Osteoporosis
- CEC – sepsis program Safe Hands- CEC – using Clinical Team
Leadership Distance Education Module to conduct Clinical Team Leadership Programs
- CEC, ACI and BHI providing articles for our newsletter cetiscape
• CETI collaborates with medical colleges and fellowships to support their training programs
• CETI collaborates with the Cancer Institute NSW to deliver the Basic Sciences in Oncology Course for oncology trainees
• CETI collaborates with LHDs around the allocation of training placements, the delivery of prevocational and other training programs for those who work in hospitals (including medical administration and allied health professionals), support of the rural and remote workforce, and in resource and program development
• CETI collaborates with LHDs and tertiary institutions as undergraduate education providers to ensure graduates are ready to work in a team-based environment
• CETI collaborates in developing rural research capacity with LHDs, tertiary institutions, the NSW Primary Health Care Research Capacity Building Program (NSW PHC) and the Australian Rural Health Research Collaboration.
• CETI collaborates with the Rural Doctors Network on our Rural Clinical Team Leadership program, the medical intern allocation, rural preference recruitment, rural scholarships, Prevocational GP Placement Program (PGPPP) and accreditation
• CETI collaborates with Health Workforce Australia (HWA) on the Clinical Training Reform work group programs and projects to improve and expand access to quality clinical training for health professionals
Goal 8: Collaboration
CETI collaborates with LHDs and tertiary institutions as undergraduate education providers to ensure graduates are ready to work in a team-based environment

CETI > ANNUAL REPORT 2010/11 33
CETI has been using a collaborative approach to build the capacity of rural based researchers with the aim of growing the rural evidence base. There are many organisations and individuals working together to support the Rural Research Capacity Building Program (RRCBP) providing tutoring, mentoring, training or advocacy. These include The NSW Primary Health Care Research Capacity Building Program (NSW PHC) – a Commonwealth funded program that includes the University of Sydney, University of New South Wales, Newcastle University, Australian National University Departments of General Practice, and the Broken Hill, Lismore (USYD) and Tamworth (Newcastle University) University Departments of Rural Health, as well as the Australian Rural Health Research Collaboration and The University of Sydney School of Rural Health (Dubbo and Orange).
Staff from all rural local health districts in NSW are invited to participate in the RRCBP and are awarded a place in the program based on their readiness to undertake a research project, the relevance of the research to advancing rural health and support from their health service. The program commenced in 2006 and in 2011 received its sixth intake.
Candidates from the 2009 and 2010 intakes, along with mentors and lecturers attended a workshop in February 2011 at the University of Sydney to provide the skills and confidence required by candidates to advance their chosen research project. The NSW PHC collaboration in the workshops worked well. The teaching team were experienced facilitators with a deep appreciation of the context in which rural health professionals are working and knowledge of rural research that could support each candidate’s research project.
Mentoring is a highly valued part of the RRCBP which contributes to the development of sustainable research relationships. All mentors give freely of their time and expertise and are a tangible product of the extensive collaboration which supports the program.
Program outcomes are measured by self-assessed competence on selected research skills using the ‘Research Spider’, a validated tool for measuring research skills. Data collected since the program’s inception indicates that there is a statistically significant increase in research experience in each of the ten measured skills by all participants. Evaluation of the RRCBP includes the routine collection of information for all intakes on factors such as financial investment, attendances at face to face workshops or teleconferences and progress to timelines for candidates. This is collected in terms of inputs, outputs and outcomes and is based on a program logic model.
Evaluation, feedback from candidates and evolving partnerships in collaboration have continued to strengthen the structure and content of the program, which is delivering skilled rural based researchers.
“Each of the participants has produced high quality research that addresses an important rural health issue. This is an excellent program.”Professor David Lyle, Head of The University of Sydney, Broken Hill, University Department of Rural Health
“This is the gold standard for a collaborative researcher development program in that it selects clinicians who research important clinical problems and provides them with academic and organisational supports which assist them to produce high quality and clinically relevant research. The future of rural health research depends on programs like this.”Associate Professor D A Perkins, Director Centre for Remote Health Research, University of Sydney, Editor in chief, Australian Journal of Rural Health
“[Research is] not about one person‘s work, it‘s about collaboration and that‘s one thing the program can help you with. It identifies networks and the value of working within a network.” [Candidate comment from the external ARTD Consultants evaluation 2010]
Collaboration helps rural based researchers
Workshop lecturers, Prof David Lyle, A/Prof David Perkins, Ms Frances Boreland (University Department of Rural Health, University of Sydney, Broken Hill), Dr Raechelle Rubenstein (University of Sydney), Dr Emma Webster and Mr David Schmidt (CETI) with research candidates and mentors
in focus
REPORT AGAINST OUR GOALS34
2 Report against our goals
As part of our ongoing evaluation and planning process, CETI has started developing an organisational evaluation framework to ensure that the organisation and its initiatives, programs and projects are evaluated regularly, consistently and in accord with principles of best practice. This work builds on a number of related CETI activities including the review of prevocational training networks and the evaluation of capacity building programs. In addition to identifying organisational achievements and informing decision making, the framework will ensure that business decisions are based on evidence and that the organisation is accountable. Evaluation findings will identify our strengths and weaknesses and contribute to continual enhancement of our work.
Part of CETI’s approach to evaluation is staff capability building. Staff will be supported in evaluation planning including program logic modeling. Results identified through such activities will be communicated to stakeholders and findings will be incorporated into programs to drive improvement. In March 2011, CETI held its first program logic workshop for staff. A number of places were offered to partner agencies, and we welcomed participants from the Policy and Technical Support Unit, the Clinical Excellence Commission and the Cancer Institute NSW. Program logic is a practical method for planning programs to ensure that the linkages between aims, processes and outcomes are logical and that evaluation of the program is integral to the program design.
As CETI’s new directorates and centre take shape, staff will create program-specific evaluation plans within the framework and guided by the organisation’s mission and goals.
Evaluation
As CETI’s new directorates and centre take shape, staff will create program-specific evaluation plans within the framework and guided by the organisation’s mission and goals
CETI > ANNUAL REPORT 2010/11 35

OUR PEOPLE36
3Our people
Executive teamIn 2010-2011 the CETI Executive team consisted of
Prof Steven Boyages Chief Executive
Dr Gaynor Heading General Manager
Linda Cutler Executive Director Rural Directorate
Prof Simon Willcock Acting Director Medical Directorate
Dr Paul Cunningham Acting Head Medical Directorate (from April 2011)
The CETI team
Management and staff
Linda Cutler, Prof Steven Boyages, Dr Gaynor Heading
CETI Rural & Remote Directorate staffProfessor Simon Willcock
CETI Head Office staff
CETI > ANNUAL REPORT 2010/11 37
Statutory Committees AUDIT AND RISK MANAGEMENT COMMITTEEThe objective of the Committee is to provide independent assistance to the Boards of the three Statutory Health Corporations (Agency for Clinical Innovation (ACI), Bureau of Health Information (BHI), Clinical Excellence Commission (CEC) and to the Chief Executive of CETI by overseeing and monitoring the statutory health corporation’s governance, risk and control frameworks, and its external accountability requirements.
Prof Steven Boyages
Member CETI Non-independent member appointed for the term of appointment as the Chief Executive of CETI
Ms Gerry Brus Member Independent memberMr Allan Cook Chair Independent memberMs Robyn Kruk Member CEC Non-independent member appointed for the term of appointment to the Board of Clinical
Excellence Commission Mrs Liz Rummery Member BHI & ACI Non-independent member appointed for the term of appointment to the Board of Bureau
of Health Information
FINANCE AND PERFORMANCE COMMITTEEThe primary purpose of the Finance and Performance Committee is to assist the CETI Chief Executive to ensure that the operating funds, capital works funds and service outputs required of the organisation are being achieved in an appropriate and efficient manner.
The Chief Executive is to ensure the requirements and provisions of the Accounts and Audit Determination issued by the Department of Health are properly observed throughout the organisation.
Mr Craig Bingham Program Manager, General Medical Training UnitMs Pamela Bloomfield Learning and Teaching Coordinator, Nursing & Midwifery DirectorateProf Steven Boyages Chief Executive (Chair) Ms Linda Cutler Director, Rural DirectorateMs Jacqueline Dominish Learning and Teaching Coordinator, Allied Health Ms Jane Evans Acting Program Manager, Standards, Accreditation and AllocationMs Lynny Groshinski Acting Deputy Head, Specialist Medical Training UnitDr Gaynor Heading General ManagerMr Trevor McKinnon Director LIFT, Centre for Learning and TeachingMs Daniella Pfeiffer Learning and Teaching Coordinator, Allied HealthMr Norman Smith (Independent Member) Finance Director, Health Support Services Ms Julie Tonowicz Acting Finance Information & Resource ManagerDr Rob Wilkins Learning and Teaching Coordinator, Centre for Learning & Teaching Prof Simon Willcock Director, Medical Directorate
CHIEF EXECUTIVE COMMITTEEThe purpose of the Chief Executive Committee is to govern CETI as determined by the Health Services Act 1997 no 154:• To promote, protect and maintain the health of the residents of NSW• To achieve and maintain adequate standards of clinical education and training that supports safe, high quality patient care• Generally to consult and co-operate (as it considers appropriate) with any one or more of the following:
- the other three pillar corporations recommended by Garling- key stakeholders (clinicians, clinical support staff, students, local hospital networks)- other individuals and organisations (including voluntary agencies, private agencies and public or local authorities)
concerned with the promotion, protection and maintenance of health
(Table on next page)
Committees
OUR PEOPLE38
3Our people
Ms Melissa Adattini ACHSM Management Trainee (Secretariat)
Ms Danielle Byers Program Coordinator, Centre for Learning & Teaching
Ms Pamela Bloomfield Learning and Teaching Coordinator, Nursing and Midwifery
Prof Steven Boyages Chief Executive
Dr Paul Cunningham Acting Head, Medical Directorate
Ms Linda Cutler Director, Rural Directorate
Ms Jacqueline Dominish Learning and Teaching Coordinator, Allied Health
Ms Jane Evans Acting Program Manager, Standards, Accreditation and Allocation
Ms Lynny Groshinski Acting Deputy Head, Specialist Medical Training Unit
Dr Gaynor Heading General Manager (Chair)
Ms Katrina Hoult Secretariat
Dr Greg Keogh Director, Medical Directorate
Mr Trevor McKinnon Director LIFT, Centre for Learning and Teaching
Ms Daniella Pfeiffer Learning and Teaching Coordinator, Allied Health
Dr Rob Wilkins Learning and Teaching Coordinator, Centre for Learning and Teaching
Prof Simon Willcock Director, Medical Directorate
Other CommitteesBASIC PHYSICIAN TRAINING COUNCIL • Promotes high quality physician training by ensuring the effective functioning of the Network Governance
Committees for basic physician training networks in New South Wales• Supports the delivery of advanced physician training as required
Ms Carmen Axisa Medical Education Officer Royal Australasian College of Physicians
Dr Sandy Beveridge Network Director of Physician Training St Vincent’s Network
Ms Christina Dawson Basic Trainee Executive Officer Royal Australasian College of Physicians
Dr Dominic Dawson Area Health Service Manager NSW Health
Dr Kumari Dissanayake Basic Trainee Junior Medical Staff Unit, Northern Sydney LHD
Ms Margaret Harburg Executive Officer, Site Accreditation, Education Deanery
Royal Australasian College of Physicians
Prof Anne Marie Hennessey Former Chairman, Professor of Medicine University of Western Sydney
Mr Jeremiah Jacinto Program Coordinator CETI
Dr Adam Lee Basic Trainee Northern Sydney & Central Coast LHDs
Dr Ken Liu Basic Trainee Sydney South West LHD
Dr Linda MacPherson Workforce Development and Innovation Ministry of Health
Dr Katrina Morris Advanced trainee
Dr Jay Ramanathan Basic Trainee
Ms Andrea Ross Support Officer CETI
Assoc Prof Ian Rewell Director of Medical Services South Eastern Sydney & Illawarra Shoalhaven LHDs
Dr Raymond Slobodniuk General Clinical Training Committee Chair General Clinical Training Committee Chair
Ms Marie-Anne Van Roie Medical Education Officer Royal Australasian College of Physicians
Prof Iven Young Clinical Chair, Basic Physician Training Council Royal Prince Alfred Hospital University of Sydney
Committees continued
CETI > ANNUAL REPORT 2010/11 39
BASIC SCIENCES IN ONCOLOGY COURSE ADVISORY COMMITTEE• Provides advice and assists CETI and the Cancer Institute NSW in achieving its objectives in the development
and delivery of the Basic Sciences in Oncology Course
Dr Joseph Bucci Topic Coordinator Radiobiology (retired December 2010)
Dr Melvin Chin Topic Coordinator Cancer Biology Medical Oncology, Prince Of Wales Clinical School
Assoc Prof Katy Clark Topic Coordinator Palliative Care Director of Palliative Care, Hunter New England LHD
Prof Stewart Dunn Topic Coordinator Communications Royal North Shore Hospital, The University of Sydney
Dr Kerwyn Foo Topic Coordinator Physics and BSOC Clinical Coordinator
Radiation Oncologist, Illawarra Cancer Group, Wollongong Hospital, University of Sydney
Ms Kay Francis Executive Officer Medical Oncology Group of Australia
Prof Val Gebski Topic Coordinator Research and Evidence Based Medicine
NHMRC Clinical Trials Centre University of Sydney Medical School
Dr Debra Graves Chief Executive Officer The Royal College of Pathologists of Australia
Ms Nadine Hackl Program Coordinator Cancer Professional and Patient Support
Cancer Institute NSW
Dr Amy Hayden Topic Coordinator Radiobiology Radiation Oncology, Westmead Cancer Care Centre
Dr Craig Lewis Medical Oncology Supervisor Medical Oncology, Prince of Wales Hospital
Dr Winston Liauw Topic Coordinator Clinical Pharmacology and BSOC Clinical Coordinator
Cancer Care Centre, St George and Sutherland Hospitals
Dr Matthew Links Medical Oncology Supervisor Cancer Care Centre, SES & Illawarra Shoalhaven LHDs
Dr Denise Lonergan Radiation Oncology Supervisor Southern NSW Network, Prince of Wales Hospital
Dr Najmun Nahar Radiation Oncology Supervisor Radiation Oncology, Westmead Cancer Care Centre
Dr Andrew Penman Chief Executive Officer (retired December 2010) Cancer Institute NSW
Dr Monica Robotin Medical Director NSW Cancer Council, School of Public Health
Dr Stephen Thompson Topic Coordinator Anatomy Radiation Oncology, SES & Illawarra Shoalhaven LHDs
CARDIOLOGY TRAINING COMMITTEE• The purpose of the NSW Joint CETI / Cardiac Society of Australia and New Zealand (SCANZ)
Cardiology Training Committee (JCTC) is to promote high quality adult cardiology training in NSW
Dr Len Kritharides Clinical Chair, Director of Cardiology Concord Repatriation Hospital
Dr Chris Alexopoulos Cardiology Specialist Port Macquarie Cardiology
Dr Rav Bhindi Cardiology - Interventional Royal North Shore Hospital
Dr Jennifer Law Advanced Cardiology Trainee St Vincent’s Hospital Sydney
Dr Christian Mussap Staff Specialist Cardiology Liverpool Hospital
Dr Young Yu Advanced Cardiology Trainee Cardiology Royal Prince Alfred
Dr Rajesh Puranik Senior Lecturer, Cardio- vascular Diseases University of Sydney, Royal Prince Alfred
Dr Preeti Choudhary Advanced Cardiology Trainee Westmead Network, JMO education
Dr Kristian Prados Advanced Cardiology Trainee Port Macquarie Hospital
Dr Pratap Shetty Cardiac Diagnostics Centre Wollongong Hospital
Ms Lynne Portelli Chief Executive Officer Cardiac Society of Australia and New Zealand

OUR PEOPLE40
3Our people
EMERGENCY MEDICINE TRAINING IMPLEMENTATION GROUP / EMERGENCY MEDICINE STATE TRAINING COUNCIL (FROM MAY 2011)• Provides oversight of the emergency medicine training networks in NSW Health services in accordance with the NSW
Health endorsed recommendations for the delivery of emergency medicine training in NSW• Reviews the composition and governance of the emergency medicine training networks in NSW
Dr Shalini Arunanthy ACEM representative Westmead Hospital
Dr Cameron Dart Emergency Department Heads representative Calvary Mater Newcastle
Ms Cathy Ellis Department of Health representative NSW Health
Ms Lynny Groshinski Senior Program Coordinator, Medical Directorate
CETI
Dr Jon Hayman Clinical Chair, Emergency Medicine Implementation Group / Emergency Medicine State Training Council (from May 2011)
Royal Prince Alfred Hospital,
Ms Mary Lawson Director of Education ACEM (from May 2011) Australasian College for Emergency Medicine
Dr Greg Keogh Deputy Director, Medical Directorate CETI
Ms Alana Killen Director of Education ACEM (to May 2011) Australasian College for Emergency Medicine
Dr Kylie McNamara Trainee representative Royal Prince Alfred Hospital
Dr Fenton O’Leary Paediatric representative Children’s Hospital Westmead
Dr Brett Oliver AHS/LHD representative South Western Sydney LHD, Liverpool Hospital
Dr Clare Skinner Trainee representative Royal North Shore Hospital
Ms Sarah Smith ESO representative (from May 2011) Western Sydney LHD
Dr Paul Spillane Directors of Emergency Medicine Training representative
Coffs Harbour Health Campus
Dr Chris Trethewy Rural representative Tamworth Base Hospital
Dr Zena Tawfik Trainee representative (to April 2011) Wollongong Hospital
Ms Toni Vial ESO representative (to March 2011) member (from March 2011)
CETI
Committees continued
Professor Iven Young, Clinical Chair Basic Physician Training Council
Dr Winston Liauw, Clinical Coordinator BSOC Advisory Committee
Dr Simon Leslie, Clinical Chair Hospital Skills Program Training Council
CETI > ANNUAL REPORT 2010/11 41
HOSPITAL SKILLS PROGRAM (HSP) TRAINING COUNCIL• Ensures effective development, implementation and oversight of the Hospital Skills Program • Promotes the delivery of professional development and life-long learning to non-specialist medical staff in NSW hospitals • Provides expert advice to CETI, Local Health Districts and the NSW Ministry of Health regarding the Hospital Skills
Program• Oversees the work of any sub-committees and working groups that may be established
Dr Michael Boyd CMO Rep HSP State Training Council Australian Society of Career Medical Officers
Mr Peter Davy Curriculum Developer CETI
Dr Anna Di Marco Network Director of Hospital Training South Eastern Sydney and Illawarra Shoalhaven LHDs
Ms Cathy Ellis Workforce Development & Innovation NSW Health
Ms Emily Feeney Education Support Officer Hunter New England LHD
Dr Ian Fielding Network Director of Hospital Training Mid North Coast and Northern NSW LHDs
Dr Briege Hamill Network Director of Hospital Training Hunter New England LHD
Dr Brett Gardiner Medical Admin Rep, Director of Clinical Governance
St Vincent’s Hospital
Mr Marcello Gizzi Education Support Officer Sydney Clinical Skills & Simulation Centre, Royal North Shore Hospital
Mr Michael Hannon NSW Health Rep NSW Health
Ms Cathy Hull NSW Health Rep NSW Health
Ms Kathy James Education Support Officer South Western Sydney LHD
Dr Stephen Jurd Director of Postgraduate Medical Training in Psychiatry
Northern Sydney LHD
Dr Ross Kerridge Hunter New England LHD Representative John Hunter Hospital
Dr Simon Leslie Clinical Chair, HSP Training Council Shellharbour Hospital
Dr Geoff Marshall Clinical Rep Bathurst Base Hospital
Dr Danielle Morris Network Director of Hospital Training Western NSW and Far West LHDs
Prof Kichu Nair Director Centre for Medical Professional Development
John Hunter Hospital, Hunter New England LHD
Ms Karen Nelson Education Support Officer Western Sydney and Nepean Blue Mountains LHDs
Ms Kylie Pleming Education Support Officer Murrumbidgee and Southern NSW LHDs
Prof Graham Reece Network Director of Hospital Training Western Sydney and Nepean Blue Mountains LHDs
Prof Graeme Richardson Network Director of Hospital Training Murrumbidgee and Southern NSW LHDs
Ms Susan Sanders Education Support Officer Western NSW and Far West LHDs
Assoc Prof Tim Shaw Workforce Education & Development Group University of Sydney
Dr Kavita Varshney Network Director of Hospital Training Northern Sydney and Central Coast LHDs
Ms Toni Vial Program Coordinator CETI
Dr Mary Webber CMO Rep Ryde District Hospital, Australian Society of Career Medical Officers
Dr Ross White CMO Rep Ryde District Hospital
Ms Karen Wickham Education Support Officer Mid North Coast and Northern NSW LHDs
OUR PEOPLE42
3Our people
INTERNATIONAL HEALTH PROFESSIONALS ORIENTATION PROJECT• Oversees the development of an orientation resource for IHPs who are employed by NSW Health • Provides expert advice to CETI in relation to the form, scope and content of the resource• Adheres to CETI’s principles for the delivery of education and training in NSW
Ms Linda Cutler Executive Director Rural Directorate CETI
Ms Toni Hazell NSW Health Representative Workforce Development and Innovation Branch, NSW Health
Mr Richard McLelland Manager, Medical Recruitment Unit Murrumbidgee and Southern LHDs
Ms Rose Meiruntu Manager Nursing and Midwifery Education Centre for Education and Workforce Development
Mr Kim Nguyen A/Allied Health Director Hunter New England Health
Dr Brett Oliver Director of Clinical Governance St Vincent’s Hospital
Ms Sharon White Manager Nursing Workforce NSW Health Transitional Organisation Southern
MEDICAL ADVISORY COUNCIL / GENERAL CLINICAL TRAINING COUNCIL • Ensures that trainees are clinically competent for safe practice and to provide quality patient care• Advises on education and information resources needed to support education programs• Provides appropriate advice on other matters relating to the delivery of medical education and training
as required by the hospital
Prof Simon WillcockDr Greg Keogh
Committees continued
Overseas trained doctors Australian Medical Council pre-employment program graduates November 2010
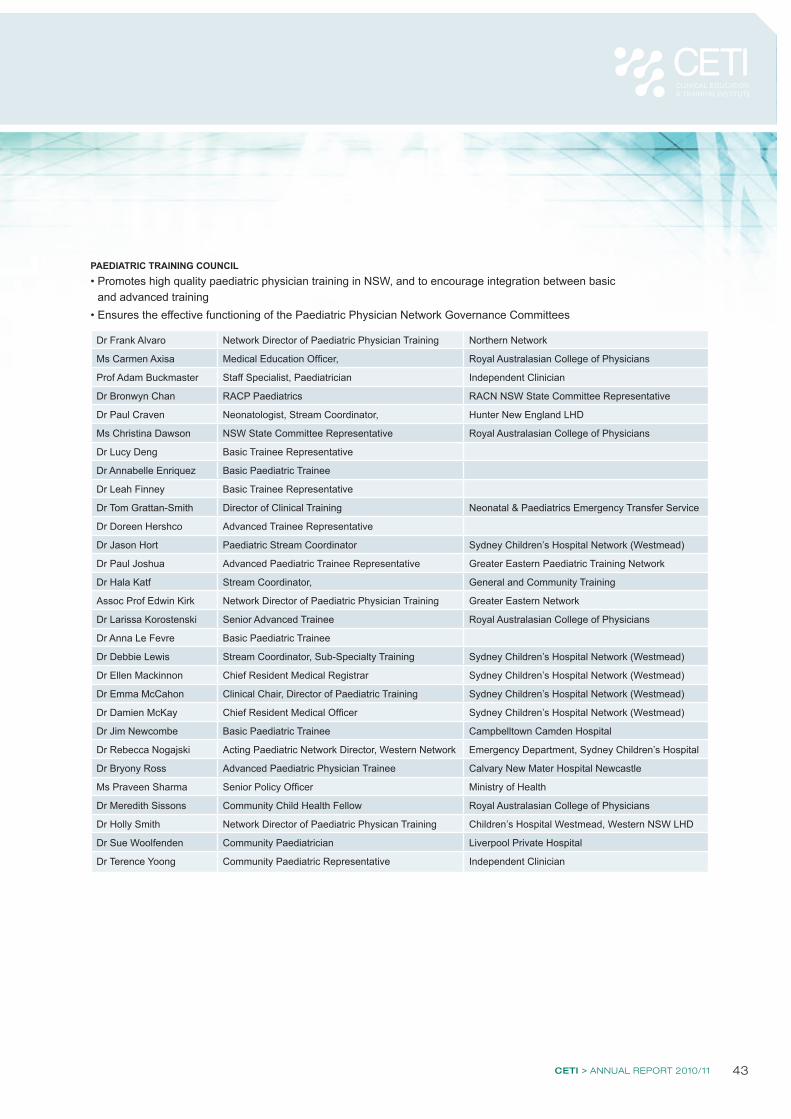
CETI > ANNUAL REPORT 2010/11 43
PAEDIATRIC TRAINING COUNCIL • Promotes high quality paediatric physician training in NSW, and to encourage integration between basic
and advanced training• Ensures the effective functioning of the Paediatric Physician Network Governance Committees
Dr Frank Alvaro Network Director of Paediatric Physician Training Northern Network
Ms Carmen Axisa Medical Education Officer, Royal Australasian College of Physicians
Prof Adam Buckmaster Staff Specialist, Paediatrician Independent Clinician
Dr Bronwyn Chan RACP Paediatrics RACN NSW State Committee Representative
Dr Paul Craven Neonatologist, Stream Coordinator, Hunter New England LHD
Ms Christina Dawson NSW State Committee Representative Royal Australasian College of Physicians
Dr Lucy Deng Basic Trainee Representative
Dr Annabelle Enriquez Basic Paediatric Trainee
Dr Leah Finney Basic Trainee Representative
Dr Tom Grattan-Smith Director of Clinical Training Neonatal & Paediatrics Emergency Transfer Service
Dr Doreen Hershco Advanced Trainee Representative
Dr Jason Hort Paediatric Stream Coordinator Sydney Children’s Hospital Network (Westmead)
Dr Paul Joshua Advanced Paediatric Trainee Representative Greater Eastern Paediatric Training Network
Dr Hala Katf Stream Coordinator, General and Community Training
Assoc Prof Edwin Kirk Network Director of Paediatric Physician Training Greater Eastern Network
Dr Larissa Korostenski Senior Advanced Trainee Royal Australasian College of Physicians
Dr Anna Le Fevre Basic Paediatric Trainee
Dr Debbie Lewis Stream Coordinator, Sub-Specialty Training Sydney Children’s Hospital Network (Westmead)
Dr Ellen Mackinnon Chief Resident Medical Registrar Sydney Children’s Hospital Network (Westmead)
Dr Emma McCahon Clinical Chair, Director of Paediatric Training Sydney Children’s Hospital Network (Westmead)
Dr Damien McKay Chief Resident Medical Officer Sydney Children’s Hospital Network (Westmead)
Dr Jim Newcombe Basic Paediatric Trainee Campbelltown Camden Hospital
Dr Rebecca Nogajski Acting Paediatric Network Director, Western Network Emergency Department, Sydney Children’s Hospital
Dr Bryony Ross Advanced Paediatric Physician Trainee Calvary New Mater Hospital Newcastle
Ms Praveen Sharma Senior Policy Officer Ministry of Health
Dr Meredith Sissons Community Child Health Fellow Royal Australasian College of Physicians
Dr Holly Smith Network Director of Paediatric Physican Training Children’s Hospital Westmead, Western NSW LHD
Dr Sue Woolfenden Community Paediatrician Liverpool Private Hospital
Dr Terence Yoong Community Paediatric Representative Independent Clinician
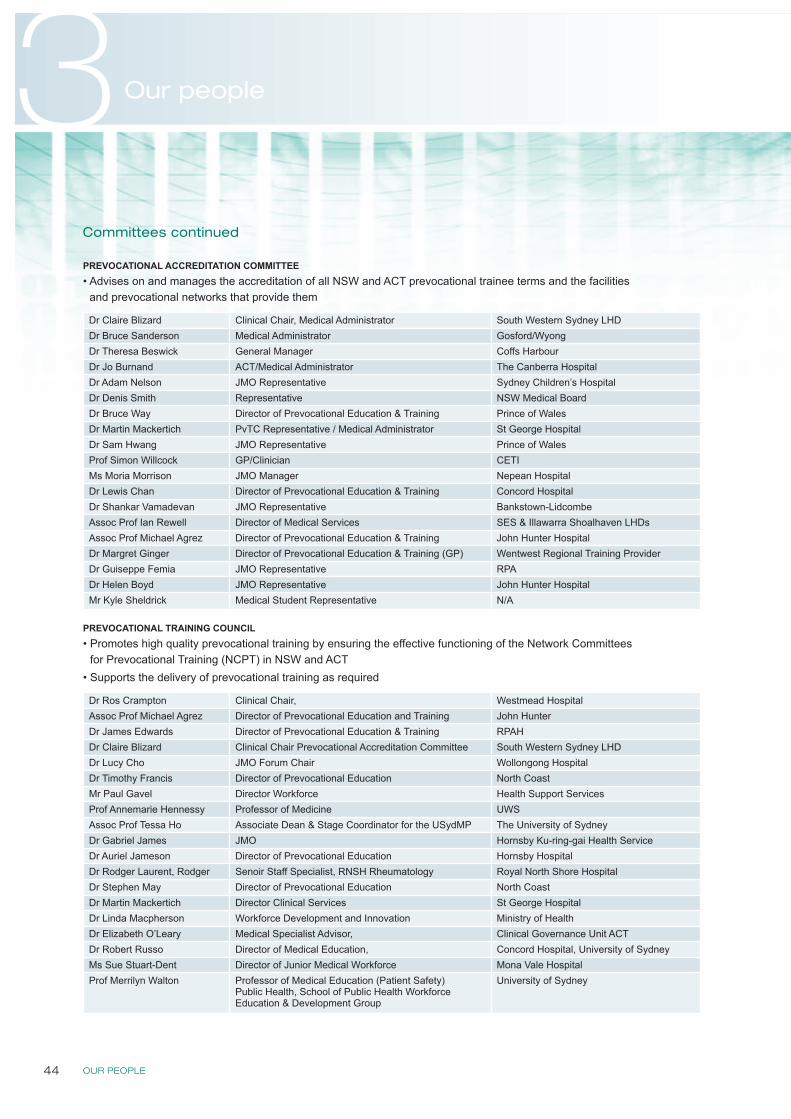
OUR PEOPLE44
3Our people
PREVOCATIONAL ACCREDITATION COMMITTEE • Advises on and manages the accreditation of all NSW and ACT prevocational trainee terms and the facilities
and prevocational networks that provide them
Dr Claire Blizard Clinical Chair, Medical Administrator South Western Sydney LHDDr Bruce Sanderson Medical Administrator Gosford/WyongDr Theresa Beswick General Manager Coffs HarbourDr Jo Burnand ACT/Medical Administrator The Canberra HospitalDr Adam Nelson JMO Representative Sydney Children’s HospitalDr Denis Smith Representative NSW Medical BoardDr Bruce Way Director of Prevocational Education & Training Prince of WalesDr Martin Mackertich PvTC Representative / Medical Administrator St George HospitalDr Sam Hwang JMO Representative Prince of WalesProf Simon Willcock GP/Clinician CETIMs Moria Morrison JMO Manager Nepean HospitalDr Lewis Chan Director of Prevocational Education & Training Concord HospitalDr Shankar Vamadevan JMO Representative Bankstown-LidcombeAssoc Prof Ian Rewell Director of Medical Services SES & Illawarra Shoalhaven LHDsAssoc Prof Michael Agrez Director of Prevocational Education & Training John Hunter HospitalDr Margret Ginger Director of Prevocational Education & Training (GP) Wentwest Regional Training ProviderDr Guiseppe Femia JMO Representative RPADr Helen Boyd JMO Representative John Hunter HospitalMr Kyle Sheldrick Medical Student Representative N/A
PREVOCATIONAL TRAINING COUNCIL• Promotes high quality prevocational training by ensuring the effective functioning of the Network Committees
for Prevocational Training (NCPT) in NSW and ACT• Supports the delivery of prevocational training as required
Dr Ros Crampton Clinical Chair, Westmead HospitalAssoc Prof Michael Agrez Director of Prevocational Education and Training John HunterDr James Edwards Director of Prevocational Education & Training RPAHDr Claire Blizard Clinical Chair Prevocational Accreditation Committee South Western Sydney LHDDr Lucy Cho JMO Forum Chair Wollongong HospitalDr Timothy Francis Director of Prevocational Education North CoastMr Paul Gavel Director Workforce Health Support ServicesProf Annemarie Hennessy Professor of Medicine UWSAssoc Prof Tessa Ho Associate Dean & Stage Coordinator for the USydMP The University of SydneyDr Gabriel James JMO Hornsby Ku-ring-gai Health ServiceDr Auriel Jameson Director of Prevocational Education Hornsby HospitalDr Rodger Laurent, Rodger Senoir Staff Specialist, RNSH Rheumatology Royal North Shore HospitalDr Stephen May Director of Prevocational Education North CoastDr Martin Mackertich Director Clinical Services St George HospitalDr Linda Macpherson Workforce Development and Innovation Ministry of HealthDr Elizabeth O’Leary Medical Specialist Advisor, Clinical Governance Unit ACTDr Robert Russo Director of Medical Education, Concord Hospital, University of SydneyMs Sue Stuart-Dent Director of Junior Medical Workforce Mona Vale HospitalProf Merrilyn Walton Professor of Medical Education (Patient Safety)
Public Health, School of Public Health Workforce Education & Development Group
University of Sydney
Committees continued
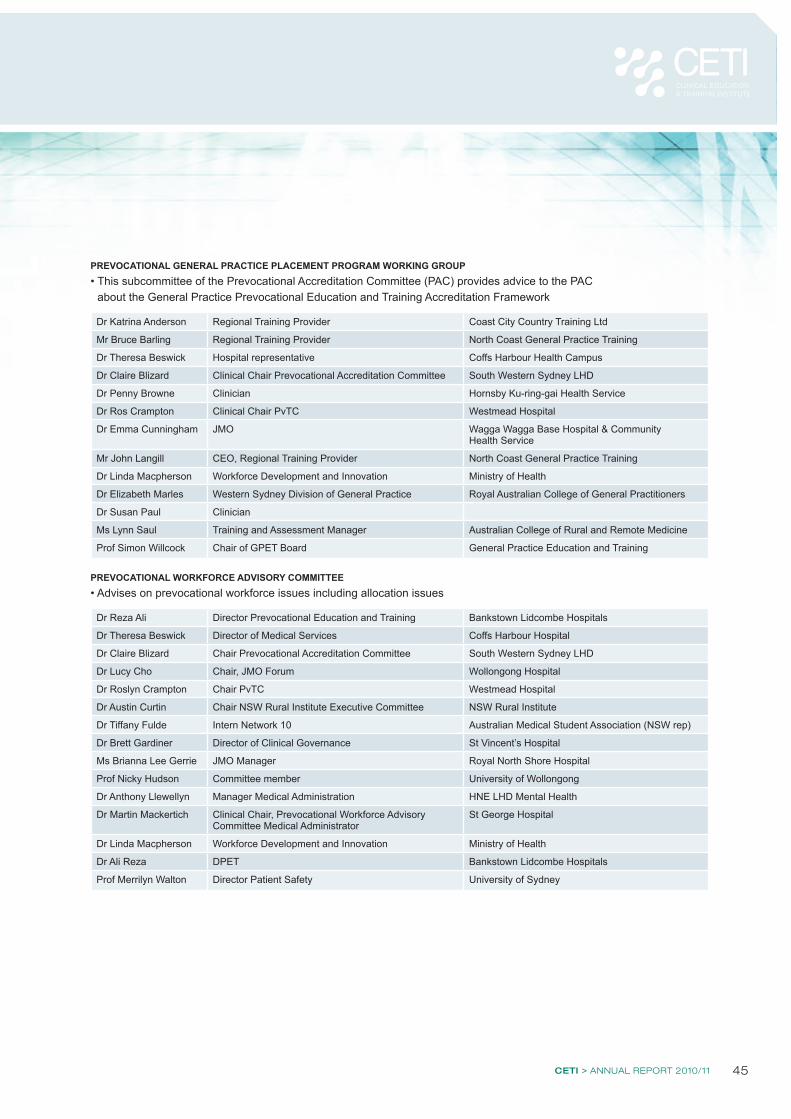
CETI > ANNUAL REPORT 2010/11 45
PREVOCATIONAL GENERAL PRACTICE PLACEMENT PROGRAM WORKING GROUP• This subcommittee of the Prevocational Accreditation Committee (PAC) provides advice to the PAC
about the General Practice Prevocational Education and Training Accreditation Framework
Dr Katrina Anderson Regional Training Provider Coast City Country Training Ltd
Mr Bruce Barling Regional Training Provider North Coast General Practice Training
Dr Theresa Beswick Hospital representative Coffs Harbour Health Campus
Dr Claire Blizard Clinical Chair Prevocational Accreditation Committee South Western Sydney LHD
Dr Penny Browne Clinician Hornsby Ku-ring-gai Health Service
Dr Ros Crampton Clinical Chair PvTC Westmead Hospital
Dr Emma Cunningham JMO Wagga Wagga Base Hospital & Community Health Service
Mr John Langill CEO, Regional Training Provider North Coast General Practice Training
Dr Linda Macpherson Workforce Development and Innovation Ministry of Health
Dr Elizabeth Marles Western Sydney Division of General Practice Royal Australian College of General Practitioners
Dr Susan Paul Clinician
Ms Lynn Saul Training and Assessment Manager Australian College of Rural and Remote Medicine
Prof Simon Willcock Chair of GPET Board General Practice Education and Training
PREVOCATIONAL WORKFORCE ADVISORY COMMITTEE• Advises on prevocational workforce issues including allocation issues
Dr Reza Ali Director Prevocational Education and Training Bankstown Lidcombe Hospitals
Dr Theresa Beswick Director of Medical Services Coffs Harbour Hospital
Dr Claire Blizard Chair Prevocational Accreditation Committee South Western Sydney LHD
Dr Lucy Cho Chair, JMO Forum Wollongong Hospital
Dr Roslyn Crampton Chair PvTC Westmead Hospital
Dr Austin Curtin Chair NSW Rural Institute Executive Committee NSW Rural Institute
Dr Tiffany Fulde Intern Network 10 Australian Medical Student Association (NSW rep)
Dr Brett Gardiner Director of Clinical Governance St Vincent’s Hospital
Ms Brianna Lee Gerrie JMO Manager Royal North Shore Hospital
Prof Nicky Hudson Committee member University of Wollongong
Dr Anthony Llewellyn Manager Medical Administration HNE LHD Mental Health
Dr Martin Mackertich Clinical Chair, Prevocational Workforce Advisory Committee Medical Administrator
St George Hospital
Dr Linda Macpherson Workforce Development and Innovation Ministry of Health
Dr Ali Reza DPET Bankstown Lidcombe Hospitals
Prof Merrilyn Walton Director Patient Safety University of Sydney

OUR PEOPLE46
3Our people
PSYCHIATRY TRAINING COUNCIL• Promotes and supports high quality Psychiatry training in NSW• Facilitates the integration between basic and advanced Psychiatry training• Oversees the effective functioning of the Psychiatry Network Governance Committees (NGC)
and state committees for Subspecialist Advanced Training in Psychiatry• Oversees the implementation of the CETI Principles for Psychiatry Training in NSW
Assoc Prof John Allan Mental Health Drug & Alcohol Office, NSW Chief Psychiatrist MHDAO
NSW Health
Dr Warren Kealy-Bateman
NSW Branch Training Committee University of Wollongong, Royal Australian and New Zealand College of Psychiatrists
Dr Michael Bowden Director of Training, Child & Adolescent Psychiatry Institute of Psychiatry
Dr Scott Clark Area Clinical Director of Psychiatry (Rural) Sydney West Greater South Network
Dr Martin Cohen Psychiatry Network Director of Training HNET Calvary New Mater Hospital Newcastle
Dr Andrew Ellis Forensic Mental Health Justice Health
Ms Cate Gadsby CETI representative CETI
Dr Stephen Jurd Director of Postgraduate Medical Training in Psychiatry Northern Sydney LHD
Dr Linda Macpherson Workforce Development and Innovation Ministry of Health
Dr Ros Montague Director Institute of Psychiatry
Dr Nick O’Connor Director of Mental Health (metro) Southern Western Sydney LHD
Dr Andrew Pethebridge Network Director of Training South East Sydney Illawarra Network
Prof Ian Rewell Workforce Director South East Sydney Illawarra Network
Dr Murray Wright Clinical Chair, Clinical Director Mental Health Royal North Shore Hospital
RADIOLOGY TRAINING NETWORKS IMPLEMENTATION GROUP• Provides oversight of radiology training in NSW Health services in accordance with the NSW
Health endorsed recommendations for the delivery of radiology training in NSW
Mr Nick Bradshaw Workforce Manager Royal Australian and New Zealand College of Radiologists
Ms Annie Hutton Network Manager Gynae Oncology, Radiology & Nuclear Medicine
Greater Metropolitan Clinical Taskforce, Ryde
Dr Noel Young Clinical Chair, Director Imaging Services Westmead Hospital
Committees continued
Dr Claire Blizard, Clinical Chair Prevocational Accreditation Committee
Dr Ros Crampton, Clinical Chair Prevocational Training Council
Dr Vasco de Carvalho, Clinical Chair Medical Administrators Training
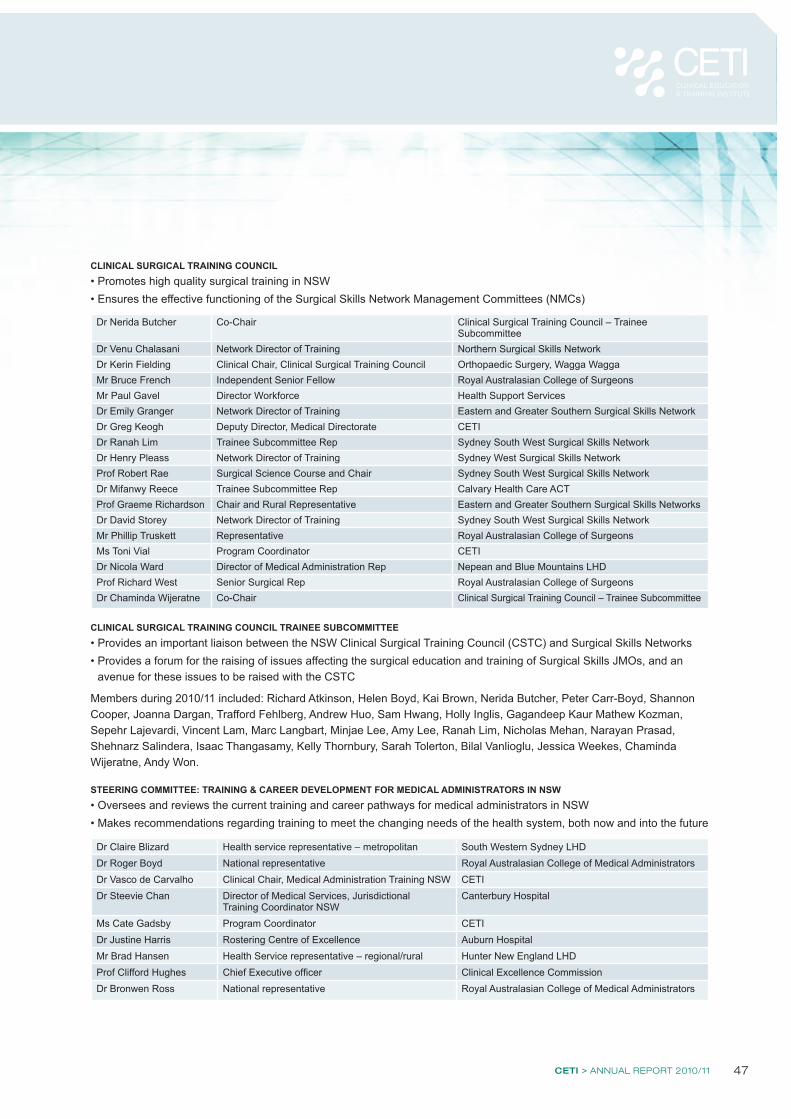
CETI > ANNUAL REPORT 2010/11 47
CLINICAL SURGICAL TRAINING COUNCIL • Promotes high quality surgical training in NSW• Ensures the effective functioning of the Surgical Skills Network Management Committees (NMCs)
Dr Nerida Butcher Co-Chair Clinical Surgical Training Council – Trainee Subcommittee
Dr Venu Chalasani Network Director of Training Northern Surgical Skills NetworkDr Kerin Fielding Clinical Chair, Clinical Surgical Training Council Orthopaedic Surgery, Wagga WaggaMr Bruce French Independent Senior Fellow Royal Australasian College of SurgeonsMr Paul Gavel Director Workforce Health Support ServicesDr Emily Granger Network Director of Training Eastern and Greater Southern Surgical Skills NetworkDr Greg Keogh Deputy Director, Medical Directorate CETI Dr Ranah Lim Trainee Subcommittee Rep Sydney South West Surgical Skills NetworkDr Henry Pleass Network Director of Training Sydney West Surgical Skills NetworkProf Robert Rae Surgical Science Course and Chair Sydney South West Surgical Skills NetworkDr Mifanwy Reece Trainee Subcommittee Rep Calvary Health Care ACTProf Graeme Richardson Chair and Rural Representative Eastern and Greater Southern Surgical Skills NetworksDr David Storey Network Director of Training Sydney South West Surgical Skills NetworkMr Phillip Truskett Representative Royal Australasian College of SurgeonsMs Toni Vial Program Coordinator CETIDr Nicola Ward Director of Medical Administration Rep Nepean and Blue Mountains LHDProf Richard West Senior Surgical Rep Royal Australasian College of SurgeonsDr Chaminda Wijeratne Co-Chair Clinical Surgical Training Council – Trainee Subcommittee
CLINICAL SURGICAL TRAINING COUNCIL TRAINEE SUBCOMMITTEE• Provides an important liaison between the NSW Clinical Surgical Training Council (CSTC) and Surgical Skills Networks• Provides a forum for the raising of issues affecting the surgical education and training of Surgical Skills JMOs, and an
avenue for these issues to be raised with the CSTC
Members during 2010/11 included: Richard Atkinson, Helen Boyd, Kai Brown, Nerida Butcher, Peter Carr-Boyd, Shannon Cooper, Joanna Dargan, Trafford Fehlberg, Andrew Huo, Sam Hwang, Holly Inglis, Gagandeep Kaur Mathew Kozman, Sepehr Lajevardi, Vincent Lam, Marc Langbart, Minjae Lee, Amy Lee, Ranah Lim, Nicholas Mehan, Narayan Prasad, Shehnarz Salindera, Isaac Thangasamy, Kelly Thornbury, Sarah Tolerton, Bilal Vanlioglu, Jessica Weekes, Chaminda Wijeratne, Andy Won.
STEERING COMMITTEE: TRAINING & CAREER DEVELOPMENT FOR MEDICAL ADMINISTRATORS IN NSW• Oversees and reviews the current training and career pathways for medical administrators in NSW• Makes recommendations regarding training to meet the changing needs of the health system, both now and into the future
Dr Claire Blizard Health service representative – metropolitan South Western Sydney LHDDr Roger Boyd National representative Royal Australasian College of Medical AdministratorsDr Vasco de Carvalho Clinical Chair, Medical Administration Training NSW CETIDr Steevie Chan Director of Medical Services, Jurisdictional
Training Coordinator NSWCanterbury Hospital
Ms Cate Gadsby Program Coordinator CETIDr Justine Harris Rostering Centre of Excellence Auburn HospitalMr Brad Hansen Health Service representative – regional/rural Hunter New England LHD Prof Clifford Hughes Chief Executive officer Clinical Excellence CommissionDr Bronwen Ross National representative Royal Australasian College of Medical Administrators
FINANCIAL REPORT48
4 Financial report
Auditor’s report
CETI > ANNUAL REPORT 2010/11 49
FINANCIAL REPORT50
4 Financial report
Auditor’s report
CETI > ANNUAL REPORT 2010/11 51
FINANCIAL REPORT52
4 Financial report
Auditor’s report (Special Purpose Service Entity)
CETI > ANNUAL REPORT 2010/11 53
FINANCIAL REPORT54
4 Financial report
Auditor’s report (Special Purpose Service Entity)
CETI > ANNUAL REPORT 2010/11 55

FINANCIAL REPORT56
4 Financial report
Management representation letter (for the year ended 30 June 2011)
2 28/09/11
TRIM DOC11/9687 Peter Achterstraat, Auditor-General The Audit Office of New South Wales GPO Box 12 SYDNEY NSW 2001
28 September 2011
Representation Letter Clinical Education and Training Institute
This representation letter is provided in connection with your audit of the financial statements of Clinical Education and Training Institute for the year ended 30 June 2011, for the purpose of you expressing an opinion as to whether the financial statements give a true and fair view in accordance with: Public Finance and Audit Act 1983
Australian Accounting Standards
We acknowledge our responsibility for keeping proper accounts and records, and preparing the financial statements. We approved the financial statements on 28 September 2011. We confirm the financial statements are free of material misstatements, including omissions. We confirm, to the best of our knowledge and belief, having made such enquiries as we considered necessary for the purpose of appropriately informing ourselves, the following representations made to you during your audit. 1. GENERAL We believe that, in all material respects, the financial statements present a view which is consistent with our understanding of the Clinical Education and Training Institute’s financial position as at 30 June 2011, and its financial performance for the year then ended. We have fulfilled our responsibilities, as set out in the terms of the audit engagement dated 30 June 2011 for the preparation of the financial statements in accordance with Australian Accounting Standards and the Public Finance and Audit Act 1983. The financial statements give a true and fair view in accordance with these requirements. There have been no deficiencies in financial reporting practices and we have disclosed any changes to accounting policies in the financial statements. These also include voluntary changes in accounting policies not arising from initial adoption of an accounting standard or a Treasury mandate. 2. ACCOUNTING RECORDS AND TRANSACTIONS We have provided you with:
all financial records and related data, other information, explanations and assistance necessary for the conduct of the audit
minutes of all meetings (e.g. Board meetings, Audit Committee or other management meetings)
all legal issues and legal opinions which have the capacity to be relevant to the fairness of the financial statements
CETI > ANNUAL REPORT 2010/11 57
3 28/09/11
information about all deficiencies in internal control of which we are aware
additional information that you have requested from us for the purpose of the audit
unrestricted access to all persons within the entity from whom you determined it necessary to obtain audit evidence.
All transactions have been recorded in the accounting records and are reflected in the financial statements. This includes all ‘off- balance sheet’ agreements or instruments.
3. COMPLIANCE WITH LEGISLATION AND OTHER REQUIREMENTS We have no knowledge of any instances of non-compliance with laws and regulations, contracts or agreements involving management or employees who have significant roles in internal control. We have no knowledge of any breaches or possible breaches of laws and regulations, contracts or agreements whose effects should be considered when preparing the financial statements. In respect to operations during the year, we have complied with: all Cabinet and other Government directives, including Ministerial directions
all central regulatory agency financial reporting requirements
all aspects of contractual agreements that would have a material effect on the financial statements in the event of non compliance.
We have notified you of any activities or operations conducted which are not specifically required by enabling legislation. There have been no communications from regulatory authorities concerning non-compliance with, or deficiencies in, financial reporting practices that could have a material effect on the financial statements. We have notified you of: the existence of all controlled entities within one month of their creation (section 63B of the
Public Finance and Audit Act 1983)
any transactions or arrangements capable of being regarded as ‘private sector funded infrastructure’, outsourcings of significant areas of activity or any other matters dealt with in Part 2B of the Public Authorities (Financial Arrangements) Act 1987
all Cabinet and other Government directives.
We have prepared contract summaries for all transactions covered by the ‘Working with Government: Guidelines on Privately Financed Projects’ (Treasury Circular 06/25) and submitted these summaries to the Auditor-General for audit within 30 days of the contract becoming effective. 4. INTERNAL CONTROLS We have established and maintained adequate internal control to ensure we: prepare reliable financial statements
maintain adequate financial records
record all material transactions in the accounting records underlying the financial statements
minimise the risk of fraud and error occurring and are able to detect them should they occur
minimise the risk of significant breaches of legislation and other mandatory requirements occurring and detect significant breaches of legislation and other mandatory requirements should they occur.
FINANCIAL REPORT58
4 Financial report
Management representation letter continued
4 28/09/11
5. FRAUD AND ERROR We acknowledge our responsibility for the design and implementation of internal controls to prevent and detect fraud and error. We have disclosed to you the results of our assessment of the risk that the financial statements may be materially misstated as a result of fraud. We have no knowledge of any fraud or suspected fraud affecting the entity involving management, employees who have significant roles in internal control or others where the fraud could have a material effect on the financial statements. Fraud includes misstatements resulting from fraudulent financial reporting and misstatements resulting from misappropriation of assets. We have no knowledge of any allegations of fraud, or suspected fraud, affecting the entity’s financial statements communicated to us by employees, former employees, analysts, regulators or others. 6. INTERNAL AUDIT We operate an effective internal audit function and management promptly rectify any shortcomings reported. We have appropriate internal audit and risk management practices in place (TPP 09-5 ‘Internal Audit and Risk Management Policy’) and have satisfied core requirements specified in the Policy. In particular we have: established and maintained an Internal Audit function
established an Audit and Risk Committee with a majority of independent members and an independent chair including at least three members and no more than five members
ensured the Audit and Risk Committee has a charter consistent with the content of the ‘model charter’
established and maintained an enterprise risk management process appropriate to Clinical
Education and Training Institute and this is consistent with current Australian/New Zealand Standards on risk management
ensured the operation of the Internal Audit function is consistent with IIA International Standards for the Professional Practice of Internal Audit.
7. FINANCIAL STATEMENTS We have no plans or intentions that may materially affect the carrying values or classification of assets or liabilities. For-Profit/Not-For-Profit Classification We have considered all aspects in evaluating whether our entity is ‘For-Profit’ or ‘Not-For-Profit’ based on Treasury’s Accounting Policy Distinguishing For-Profit from Not-For-Profit Entities (TPP 05-4). Our entity’s classification is supported by consideration of: statements about the objectives of the entity, such as those contained in legislation,
regulations, entity constitutions and shareholder resolutions
the governance framework applied to the entity i.e. the corporate structure
the purpose, nature and extent of funding, focusing on the extent to which ongoing budget support is provided to the entity
CETI > ANNUAL REPORT 2010/11 59
5 28/09/11
the targeted financial performance of the entity, as agreed between the Government and the board/management, focusing on the extent to which the entity funds its expenses, maintains its asset base and provides returns
the classification of the entity under Government Finance Statistics (GFS). Non-Current Assets Clinical Education and Training Institute has satisfactory title of all assets. There are no liens or encumbrances on such assets nor has any asset been pledged as collateral. We depreciate assets over their useful lives and we have adjusted depreciation charges for all material abandoned or otherwise unusable items of property, plant and equipment. Depreciation rates have been reviewed against asset usage and the rate of technical and commercial obsolescence. Any adjustment to reflect the most recent assessment of the useful lives of all non-current assets has been recognised and disclosed in the financial statements. The carrying amount of each physical non-current asset does not materially differ from its fair value at the end of the reporting period. Significant fair value assumptions, including fair value assumptions with high estimation uncertainty are reasonable. We have considered the requirements of AASB 136 ‘Impairment of Assets’, when assessing the impairment of assets and in ensuring no assets are stated in excess of their recoverable amount. We have communicated to you all indicators of impairment and where these exist, we have conducted appropriate impairment testing on the relevant asset. Impairment of Receivables The impairment of receivables is sufficient to provide for any losses on realisation and we have written off all known bad debts. Other Current Assets We expect to realise all other current assets at least at the amounts at which they are stated in the financial statements. Liabilities We have recognised all liabilities including those arising under derivative financial instruments in the financial statements. Provisions, Contingent Assets and Contingent Liabilities We have properly recorded and/or disclosed in the financial statements: arrangements involving restrictions on cash balances, compensating balances and line-of-credit
or similar arrangements
agreements or options to repurchase assets previously sold
material or contingent liabilities or assets including those arising under derivative financial instruments.
Employee Benefits All post-employment benefits have been identified and properly accounted for and all events impacting the plans have been brought to the actuary’s attention. For defined benefit plans:
FINANCIAL REPORT60
4 Financial report
Management representation letter continued
6 28/09/11
the actuarial assumptions underlying the valuation of the plan are in accordance with the Clinical Education and Training Institute’s best estimate of future events and are consistent with our knowledge of the business
the actuary’s calculations have been based on complete and up-to-date member information
the amounts included in the financial statements derived from the work of the actuary are in accordance with the requirements of AASB 119 ‘Employee Benefits’.
Commitments We have disclosed all material commitments for construction or acquisition of property, plant and equipment or to acquire other non-current assets, such as investments or intangibles, in the financial statements. Taxation We have calculated and recognised all other applicable taxes according to relevant tax legislation. There are no activities that invoke the anti-avoidance provisions of the Tax Equivalent Regime or other applicable tax legislation. Related Party Transactions We have made available to you details and records relating to: any agreements or transactions between employee controlled entities and any of our controlled
entities
any equity interests or directorships held by employees in other entities, which are party to, directly or indirectly, any agreements or transactions with this organisation and/or any controlled entity or related party of this organisation
any external accounting advice received on these agreements, transactions or interests. Key Management Personnel Disclosures We have indentified all the agency’s key management personnel and have disclosed all remuneration benefits received during the year. We believe that disclosures in the financial statements are complete and in accordance with Australian Accounting Standards. Accounting for Investments in Associates We have made available to you details and records relating to the existence and ownership of all equity interests held in associates (i.e. all entities over which Clinical Education and Training Institute has significant influence). Accounting for Investments in Joint Ventures We have made available to you details and records relating to the existence of all our ownership interests held in any joint venture operation. Environmental Issues We have considered whether environmental matters could have a material impact on the financial statements and conclude that: we are not aware of any material liabilities or contingencies arising from environmental matters,
including those resulting from illegal or possibly illegal acts
we are not aware of environmental matters that may result in a material impairment of assets
where we are aware of such matters referred to in the two points above, we have disclosed to you all facts relating to those matters.
CETI > ANNUAL REPORT 2010/11 61
7 28/09/11
Accounting Misstatements Detected by Audit We acknowledge that the attached schedule of uncorrected misstatements has been brought to our attention and we have considered the impact on the financial statements. We conclude the effects of these uncorrected misstatements are immaterial, both individually and in aggregate, to the financial statements as a whole. We have also considered the impact of uncorrected misstatements from previous periods and conclude the aggregate amount of these misstatements is immaterial to the previous and current periods’ financial statements. Native Title Land Claims We are not aware of any native title land claims that may have a material impact on the financial statements. Insurance We have established procedures to assess the adequacy of insurance cover on all assets and insurable risks, and where appropriate, assets and insurable risks are adequately covered by insurance. Litigation and Claims We confirm that all known actual or possible litigation and claims have been disclosed to you. The effects of these events have been appropriately accounted for and disclosed in accordance with the applicable financial reporting framework. We have provided to you all information regarding material outstanding legal matters. Accounting Estimates We confirm the significant assumptions used in making accounting estimates are reasonable and have been disclosed in the financial statements. We confirm the measurement processes, including related assumptions, used by management to determine accounting estimates in the context of the applicable financial reporting framework are appropriate and have been consistently applied. We confirm the disclosures related to accounting estimates are complete and appropriate. Fair Value Measurements and Disclosures Where assets and liabilities are recorded at fair value, the value attributed to these assets and liabilities is the fair value. We confirm the significant assumptions used in fair value measurements and disclosures are reasonable, and appropriately reflect our intent and ability to carry out specific courses of action on behalf of Clinical Education and Training Institute. We confirm the measurement methods, including related assumptions, used by management in determining fair values within the applicable financial reporting framework are appropriate, and have been consistently applied. We confirm the disclosures related to fair value in the financial statements are complete and appropriate. Going Concern We confirm the going concern basis is appropriate for the financial statements.
FINANCIAL REPORT62
4 Financial report
Management representation letter continued
8 28/09/11
After Balance Date Events All events subsequent to the date of the financial statements and for which Australian Accounting Standards require adjustment or disclosure have been adjusted or disclosed in the financial statements. Electronic Presentation of the Audited Financial Statements and Audit Report With respect to publication of the financial statements on our website and Parliament's website, we acknowledge: we are responsible for the electronic presentation of the financial statements on our website
we will ensure the electronic version of the audited financial statements and the Independent Auditor’s Report on our website will be identical to the final signed hard copy version of the audited financial statements which bears the Auditor-General's seal and the Independent Auditor’s Report
we will clearly differentiate between audited and unaudited information in the construction of our website as we understand the risk of potential misrepresentation between unaudited and audited information in the absence of appropriate controls
we have assessed the controls over the security and integrity of the data on our website and that adequate procedures are in place to ensure the integrity of the information published
we will ensure that where the Independent Auditor’s Report on the financial statements is published on our website, the financial statements are also published in full
we have complied with the requirements of the Corporations Act 2001 with respect to the electronic presentation of the audited financial statements, where applicable.
Impairment of Financial Assets We have reviewed all our financial assets for the indicators of impairment. We have no reason to believe these assets may be impaired at balance date. We have also reviewed financial assets previously written down as impaired for circumstances indicating that impairment may no longer exist in the current year. We have adjusted our financial statements appropriately in accordance with accounting standards. Financial Instruments We have notified you of all reclassifications of financial instruments made during the year together with explanations, in accordance with the requirements of Australian Accounting Standards. Other We understand your examination was made in accordance with Australian Auditing Standards and was, therefore, designed primarily for the purpose of expressing an opinion on the financial statements of the entity taken as a whole, and your tests of the financial records and other auditing procedures were limited to those you considered necessary for that purpose.
Steven Boyages MB BS PhD DDU FRACP FAFPHM Chief Executive

CETI > ANNUAL REPORT 2010/11 63
Certification of financial statements
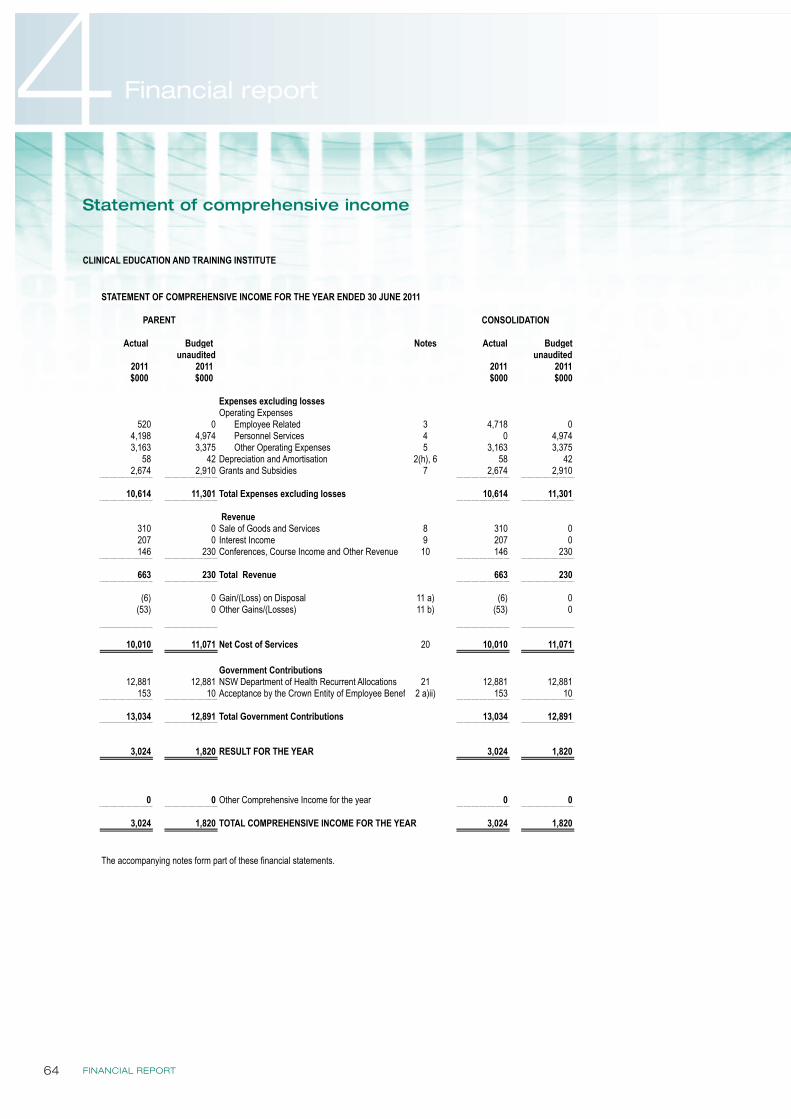
FINANCIAL REPORT64
4 Financial report
Statement of comprehensive income
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 2 of 29
PARENT CONSOLIDATION
Actual Budget Notes Actual Budgetunaudited unaudited
2011 2011 2011 2011$000 $000 $000 $000
Expenses excluding lossesOperating Expenses
520 0 Employee Related 3 4,718 04,198 4,974 Personnel Services 4 0 4,9743,163 3,375 Other Operating Expenses 5 3,163 3,375
58 42 Depreciation and Amortisation 2(h), 6 58 422,674 2,910 Grants and Subsidies 7 2,674 2,910
10,614 11,301 Total Expenses excluding losses 10,614 11,301
Revenue310 0 Sale of Goods and Services 8 310 0207 0 Interest Income 9 207 0146 230 Conferences, Course Income and Other Revenue 10 146 230
663 230 Total Revenue 663 230
(6) 0 Gain/(Loss) on Disposal 11 a) (6) 0(53) 0 Other Gains/(Losses) 11 b) (53) 0
10,010 11,071 Net Cost of Services 20 10,010 11,071
Government Contributions12,881 12,881 NSW Department of Health Recurrent Allocations 21 12,881 12,881
153 10 Acceptance by the Crown Entity of Employee Benefits 2 a)ii) 153 10
13,034 12,891 Total Government Contributions 13,034 12,891
3,024 1,820 RESULT FOR THE YEAR 3,024 1,820
0 0 Other Comprehensive Income for the year 0 0
3,024 1,820 TOTAL COMPREHENSIVE INCOME FOR THE YEAR 3,024 1,820
The accompanying notes form part of these financial statements.
STATEMENT OF COMPREHENSIVE INCOME FOR THE YEAR ENDED 30 JUNE 2011
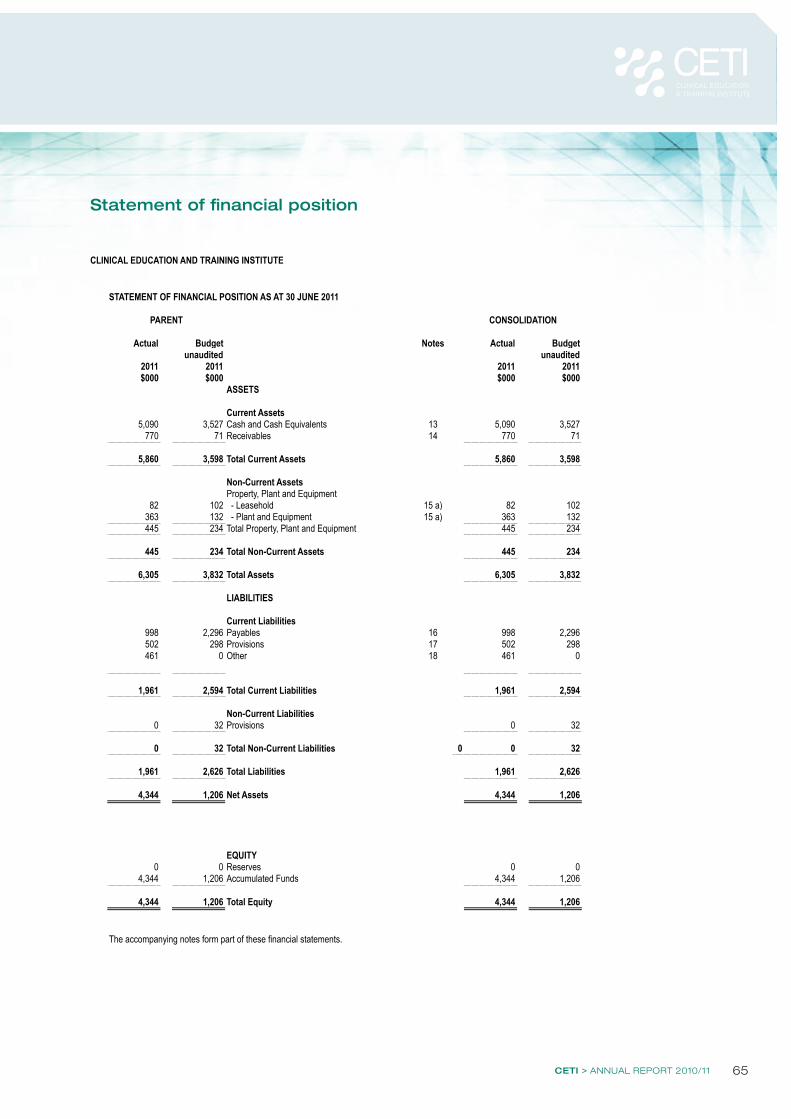
CETI > ANNUAL REPORT 2010/11 65
Statement of financial position
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 4 of 29
STATEMENT OF FINANCIAL POSITION AS AT 30 JUNE 2011
PARENT
Actual Budget Notes Actual Budgetunaudited unaudited
2011 2011 2011 2011$000 $000 $000 $000
ASSETS
Current Assets5,090 3,527 Cash and Cash Equivalents 13 5,090 3,527
770 71 Receivables 14 770 71
5,860 3,598 Total Current Assets 5,860 3,598
Non-Current AssetsProperty, Plant and Equipment
82 102 - Leasehold 15 a) 82 102363 132 - Plant and Equipment 15 a) 363 132445 234 Total Property, Plant and Equipment 445 234
445 234 Total Non-Current Assets 445 234
6,305 3,832 Total Assets 6,305 3,832
LIABILITIES
Current Liabilities998 2,296 Payables 16 998 2,296502 298 Provisions 17 502 298461 0 Other 18 461 0
1,961 2,594 Total Current Liabilities 1,961 2,594
Non-Current Liabilities0 32 Provisions 0 32
0 32 Total Non-Current Liabilities 0 0 32
1,961 2,626 Total Liabilities 1,961 2,626
4,344 1,206 Net Assets 4,344 1,206
EQUITY0 0 Reserves 0 0
4,344 1,206 Accumulated Funds 4,344 1,206
4,344 1,206 Total Equity 4,344 1,206
The accompanying notes form part of these financial statements.
CONSOLIDATION
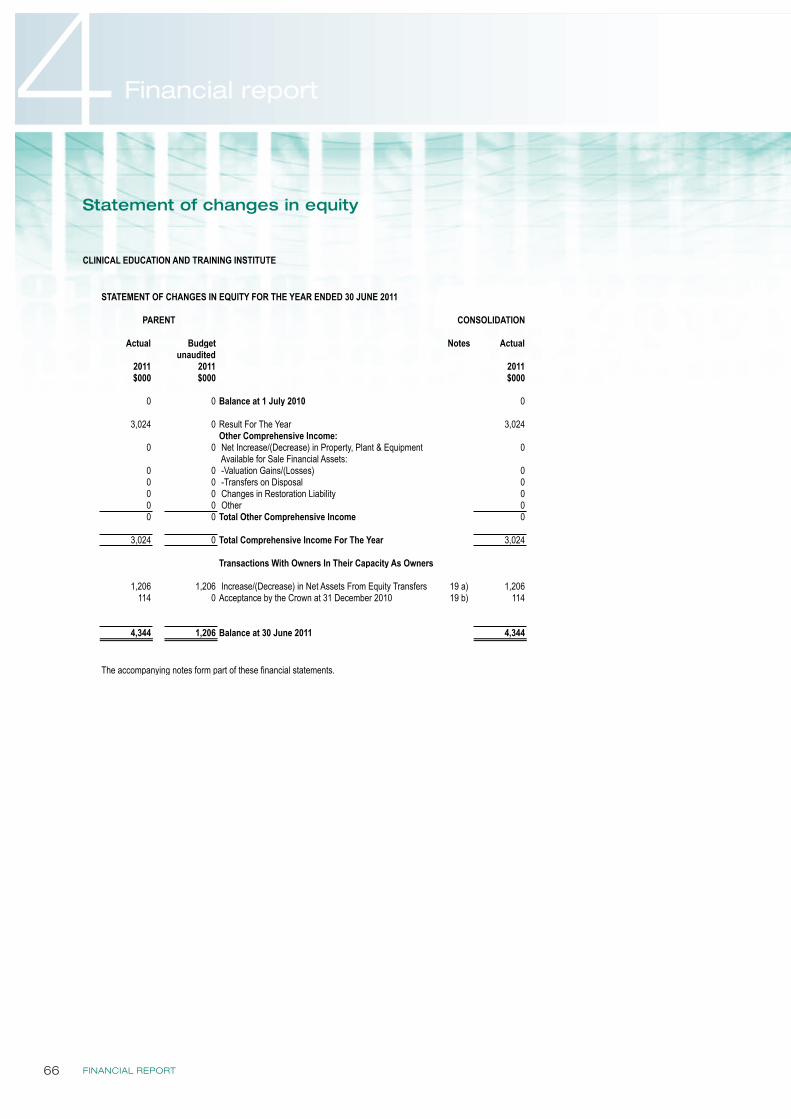
FINANCIAL REPORT66
4 Financial report
Statement of changes in equity
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 5 of 29
STATEMENT OF CHANGES IN EQUITY FOR THE YEAR ENDED 30 JUNE 2011
PARENT
Actual Budget Notes Actualunaudited
2011 2011 2011$000 $000 $000
0 0 Balance at 1 July 2010 0
3,024 0 Result For The Year 3,024Other Comprehensive Income:
0 0 Net Increase/(Decrease) in Property, Plant & Equipment 0 Available for Sale Financial Assets:
0 0 -Valuation Gains/(Losses) 00 0 -Transfers on Disposal 00 0 Changes in Restoration Liability 00 0 Other 00 0 Total Other Comprehensive Income 0
3,024 0 Total Comprehensive Income For The Year 3,024
Transactions With Owners In Their Capacity As Owners
1,206 1,206 Increase/(Decrease) in Net Assets From Equity Transfers 19 a) 1,206114 0 Acceptance by the Crown at 31 December 2010 19 b) 114
4,344 1,206 Balance at 30 June 2011 4,344
The accompanying notes form part of these financial statements.
CONSOLIDATION
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 4 of 29
STATEMENT OF FINANCIAL POSITION AS AT 30 JUNE 2011
PARENT
Actual Budget Notes Actual Budgetunaudited unaudited
2011 2011 2011 2011$000 $000 $000 $000
ASSETS
Current Assets5,090 3,527 Cash and Cash Equivalents 13 5,090 3,527
770 71 Receivables 14 770 71
5,860 3,598 Total Current Assets 5,860 3,598
Non-Current AssetsProperty, Plant and Equipment
82 102 - Leasehold 15 a) 82 102363 132 - Plant and Equipment 15 a) 363 132445 234 Total Property, Plant and Equipment 445 234
445 234 Total Non-Current Assets 445 234
6,305 3,832 Total Assets 6,305 3,832
LIABILITIES
Current Liabilities998 2,296 Payables 16 998 2,296502 298 Provisions 17 502 298461 0 Other 18 461 0
1,961 2,594 Total Current Liabilities 1,961 2,594
Non-Current Liabilities0 32 Provisions 0 32
0 32 Total Non-Current Liabilities 0 0 32
1,961 2,626 Total Liabilities 1,961 2,626
4,344 1,206 Net Assets 4,344 1,206
EQUITY0 0 Reserves 0 0
4,344 1,206 Accumulated Funds 4,344 1,206
4,344 1,206 Total Equity 4,344 1,206
The accompanying notes form part of these financial statements.
CONSOLIDATION
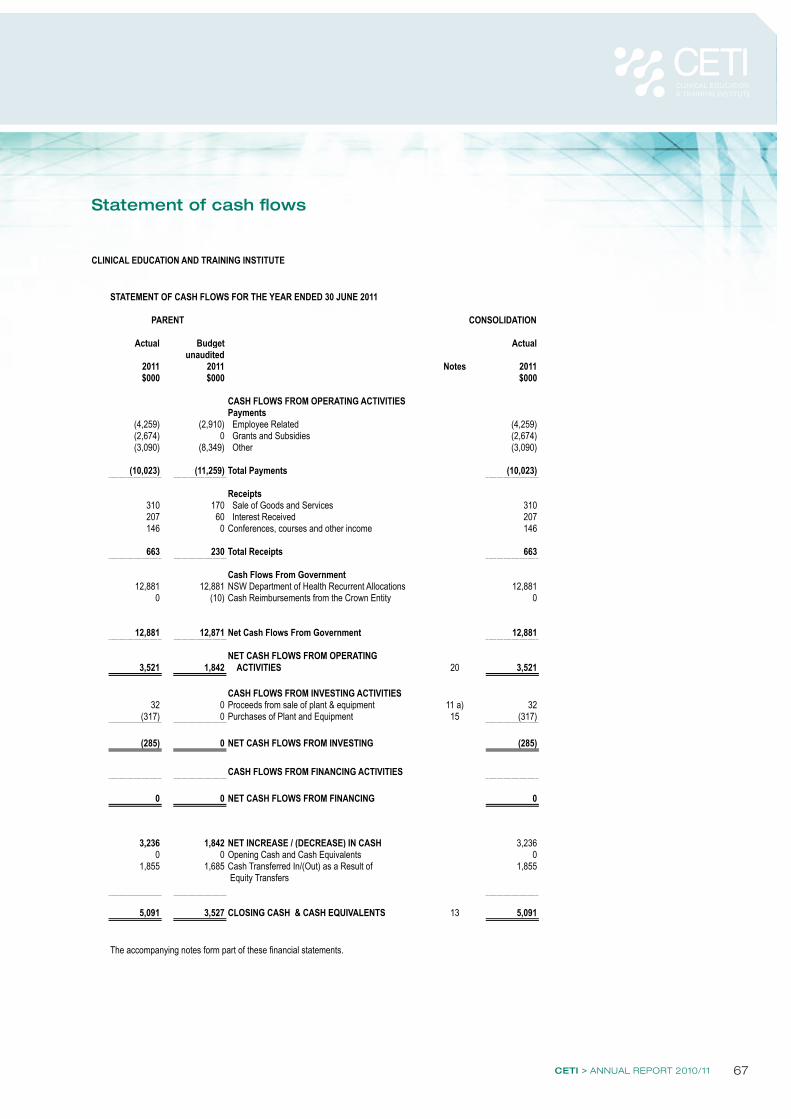
CETI > ANNUAL REPORT 2010/11 67
Statement of cash flows
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 7 of 29
PARENT CONSOLIDATION
Actual Budget Actualunaudited
2011 2011 Notes 2011$000 $000 $000
CASH FLOWS FROM OPERATING ACTIVITIESPayments
(4,259) (2,910) Employee Related (4,259)(2,674) 0 Grants and Subsidies (2,674)(3,090) (8,349) Other (3,090)
(10,023) (11,259) Total Payments (10,023)
Receipts310 170 Sale of Goods and Services 310207 60 Interest Received 207146 0 Conferences, courses and other income 146
663 230 Total Receipts 663
Cash Flows From Government12,881 12,881 NSW Department of Health Recurrent Allocations 12,881
0 (10) Cash Reimbursements from the Crown Entity 0
12,881 12,871 Net Cash Flows From Government 12,881
NET CASH FLOWS FROM OPERATING 3,521 1,842 ACTIVITIES 20 3,521
CASH FLOWS FROM INVESTING ACTIVITIES32 0 Proceeds from sale of plant & equipment 11 a) 32
(317) 0 Purchases of Plant and Equipment 15 (317)
(285) 0 NET CASH FLOWS FROM INVESTING (285)
CASH FLOWS FROM FINANCING ACTIVITIES
0 0 NET CASH FLOWS FROM FINANCING 0
3,236 1,842 NET INCREASE / (DECREASE) IN CASH 3,2360 0 Opening Cash and Cash Equivalents 0
1,855 1,685 Cash Transferred In/(Out) as a Result of 1,855 Equity Transfers
5,091 3,527 CLOSING CASH & CASH EQUIVALENTS 13 5,091
The accompanying notes form part of these financial statements.
STATEMENT OF CASH FLOWS FOR THE YEAR ENDED 30 JUNE 2011
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 4 of 29
STATEMENT OF FINANCIAL POSITION AS AT 30 JUNE 2011
PARENT
Actual Budget Notes Actual Budgetunaudited unaudited
2011 2011 2011 2011$000 $000 $000 $000
ASSETS
Current Assets5,090 3,527 Cash and Cash Equivalents 13 5,090 3,527
770 71 Receivables 14 770 71
5,860 3,598 Total Current Assets 5,860 3,598
Non-Current AssetsProperty, Plant and Equipment
82 102 - Leasehold 15 a) 82 102363 132 - Plant and Equipment 15 a) 363 132445 234 Total Property, Plant and Equipment 445 234
445 234 Total Non-Current Assets 445 234
6,305 3,832 Total Assets 6,305 3,832
LIABILITIES
Current Liabilities998 2,296 Payables 16 998 2,296502 298 Provisions 17 502 298461 0 Other 18 461 0
1,961 2,594 Total Current Liabilities 1,961 2,594
Non-Current Liabilities0 32 Provisions 0 32
0 32 Total Non-Current Liabilities 0 0 32
1,961 2,626 Total Liabilities 1,961 2,626
4,344 1,206 Net Assets 4,344 1,206
EQUITY0 0 Reserves 0 0
4,344 1,206 Accumulated Funds 4,344 1,206
4,344 1,206 Total Equity 4,344 1,206
The accompanying notes form part of these financial statements.
CONSOLIDATION
FINANCIAL REPORT68
4 Financial report
Notes to and forming part of the financial statements
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 9 of 29
Note 1
Note 2
Basis of Preparation
Statement of Compliance
Accounting Standards & Interpretations issued but not yet effective
No new or revised accounting standards or interpretations are adopted earlier than their prescribed date of application. Set out below are changes to be effected, their date of application and the possible impact on the financial statements of the Clinical Education and Training Institute.
Summary of Significant Accounting Policies
Clinical Education and Training Institute's financial statements are general purpose financial statements which have been prepared in accordance with applicable Australian Accounting Standards (which include Australian Accounting Interpretations), the requirements of the Public Finance and Audit Act 1983 and its regulations, the requirements of the Health Services Act 1997 and its regulations including observation of the Accounts and Audit Determination for Public Hospital Organisations.
Property, plant and equipment, investment property, assets (or disposal groups) held for sale and financial assets at "fair value through profit and loss" and available for sale are measured at fair value. Other financial statement items are prepared in accordance with the historical cost convention.
The consolidated entity has a net cost of services of $10,010,000. Notwithstanding that a deficiency exists the financial statements have been prepared on a going concern basis because the activities of the entity are controlled and underwritten by the New South Wales Department of Health.
All amounts are rounded to the nearest one thousand dollars and are expressed in Australian currency.
Judgments, key assumptions and estimations made by management are disclosed in the relevant notes to the financial statements.
Clinical Education and Training Institute Reporting Entity
The Clinical Education and Training Institute was established as a Statutory Corporation in accordance with the Health Services Act 1997 with effect from 1 July 2010. As a reporting entity these financial statements comprise all the operating activities under its control. Clinical Education and Training Institute is a not-for-profit entity (as profit is not its principal objective).
The annual financial statements presented herein consist of the Clinical Education and Training Institute (as the parent entity), the financial statements of the special purpose entity division and the consolidated financial statements of the economic entity. Notes capture both the parent and consolidated values with notes 3, 4, 16,17 and 20 being especially relevant.
In the process of preparing the consolidated financial statements for the economic entity consisting of the controlling and controlled entities, all inter-entity transactions and balances have been eliminated.
The reporting entity is consolidated as part of the NSW Department of Health and the NSW Total State Sector Accounts.
These consolidated financial statements for the year ended 30 June 2011 have been authorised for issue by the Chief Executive on 28 Septmber 2011.
The Clincial Education and Training Institute also controls the Clinical Education and Training Institute Special Purpose Service Entity which was established as a Division of the Government Service on 1 July 2010 in accordance with the Public Sector Employment and Management Act 2002 and the Health Services Act 1997. This Division provides personnel services to enable Clinical Education and Training Institute to excerise its functions.
The consolidated and parent entity's financial statements comply with Australian Accounting Standards which include Australian Accounting Interpretations .
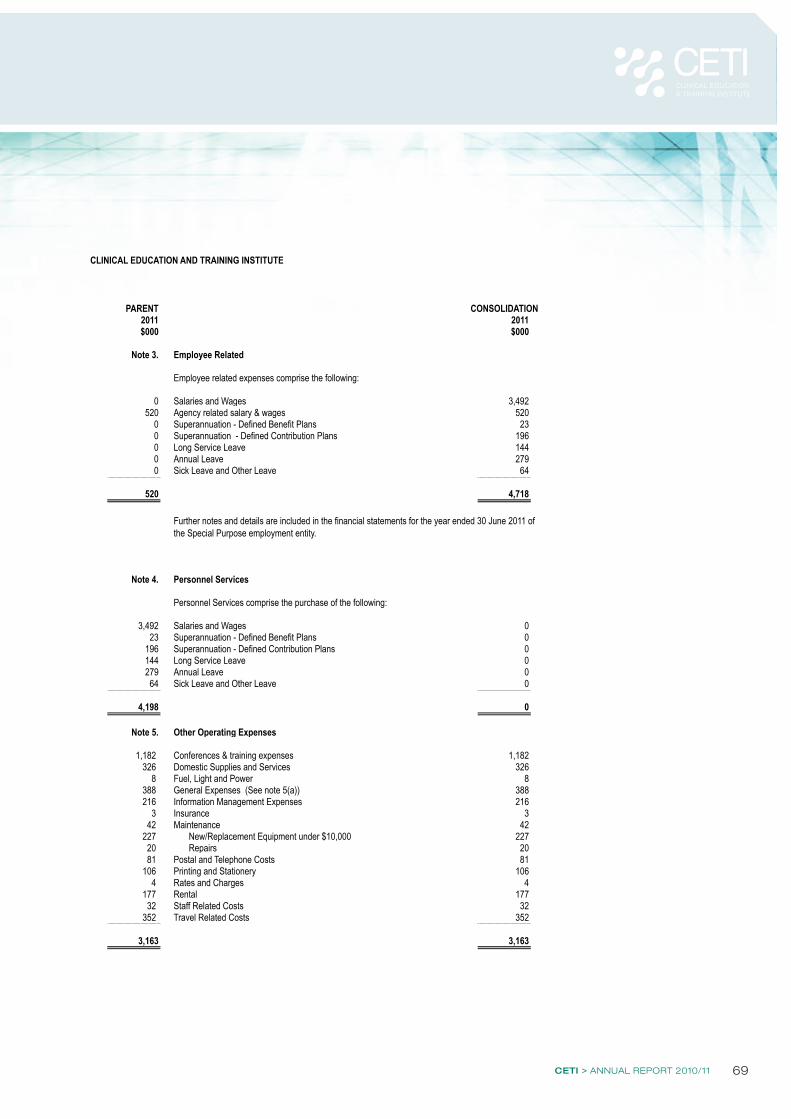
CETI > ANNUAL REPORT 2010/11 69
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 17 of 29
PARENT2011 2011$000 $000
Note 3. Employee Related
Employee related expenses comprise the following:
0 Salaries and Wages 3,492520 Agency related salary & wages 520
0 Superannuation - Defined Benefit Plans 230 Superannuation - Defined Contribution Plans 1960 Long Service Leave 1440 Annual Leave 2790 Sick Leave and Other Leave 64
520 4,718
Note 4. Personnel Services
Personnel Services comprise the purchase of the following:
3,492 Salaries and Wages 023 Superannuation - Defined Benefit Plans 0
196 Superannuation - Defined Contribution Plans 0144 Long Service Leave 0279 Annual Leave 064 Sick Leave and Other Leave 0
4,198 0
Note 5. Other Operating Expenses
1,182 Conferences & training expenses 1,182326 Domestic Supplies and Services 326
8 Fuel, Light and Power 8388 General Expenses (See note 5(a)) 388216 Information Management Expenses 216
3 Insurance 342 Maintenance 42
227 New/Replacement Equipment under $10,000 22720 Repairs 2081 Postal and Telephone Costs 81
106 Printing and Stationery 1064 Rates and Charges 4
177 Rental 17732 Staff Related Costs 32
352 Travel Related Costs 352
3,163 3,163
Further notes and details are included in the financial statements for the year ended 30 June 2011 of the Special Purpose employment entity.
CONSOLIDATION
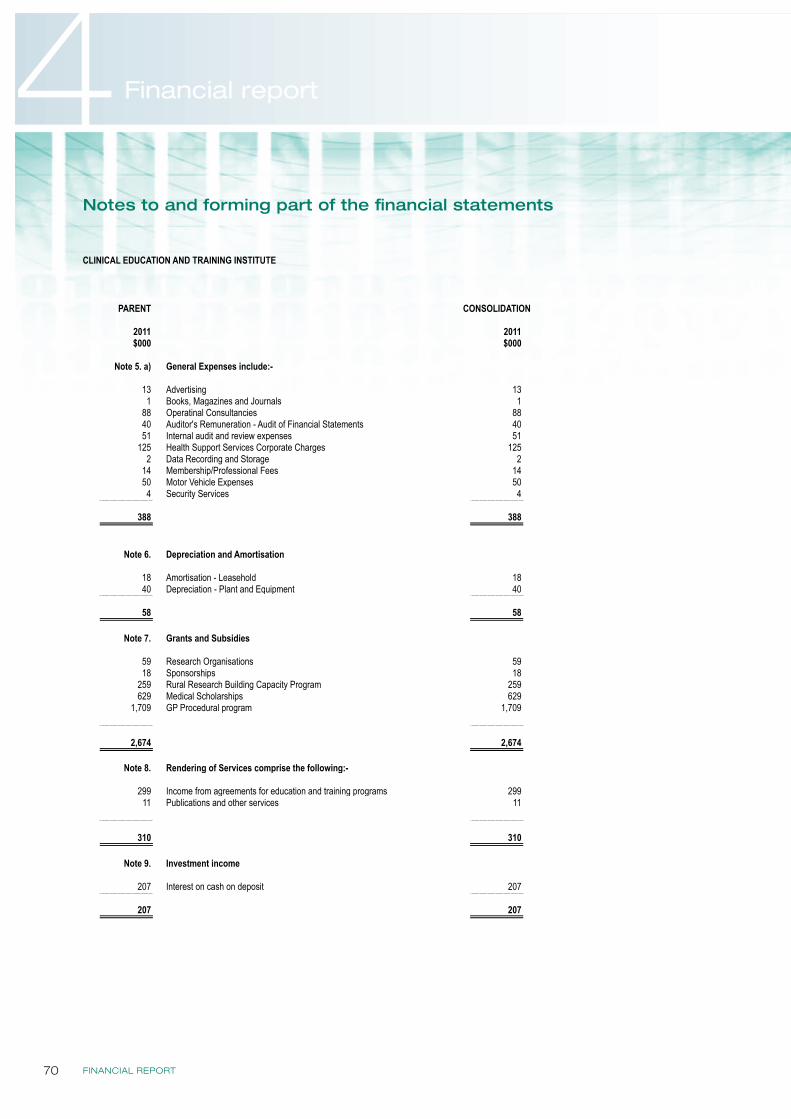
FINANCIAL REPORT70
4 Financial report
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 18 of 29
PARENT
2011 2011$000 $000
Note 5. a) General Expenses include:-
13 Advertising 131 Books, Magazines and Journals 1
88 Operatinal Consultancies 8840 Auditor's Remuneration - Audit of Financial Statements 4051 Internal audit and review expenses 51
125 Health Support Services Corporate Charges 1252 Data Recording and Storage 2
14 Membership/Professional Fees 1450 Motor Vehicle Expenses 504 Security Services 4
388 388
Note 6. Depreciation and Amortisation
18 Amortisation - Leasehold 1840 Depreciation - Plant and Equipment 40
58 58
Note 7. Grants and Subsidies
59 Research Organisations 5918 Sponsorships 18
259 Rural Research Building Capacity Program 259629 Medical Scholarships 629
1,709 GP Procedural program 1,709
2,674 2,674
Note 8. Rendering of Services comprise the following:-
299 Income from agreements for education and training programs 29911 Publications and other services 11
310 310
Note 9. Investment income
207 Interest on cash on deposit 207
207 207
CONSOLIDATION
Notes to and forming part of the financial statements
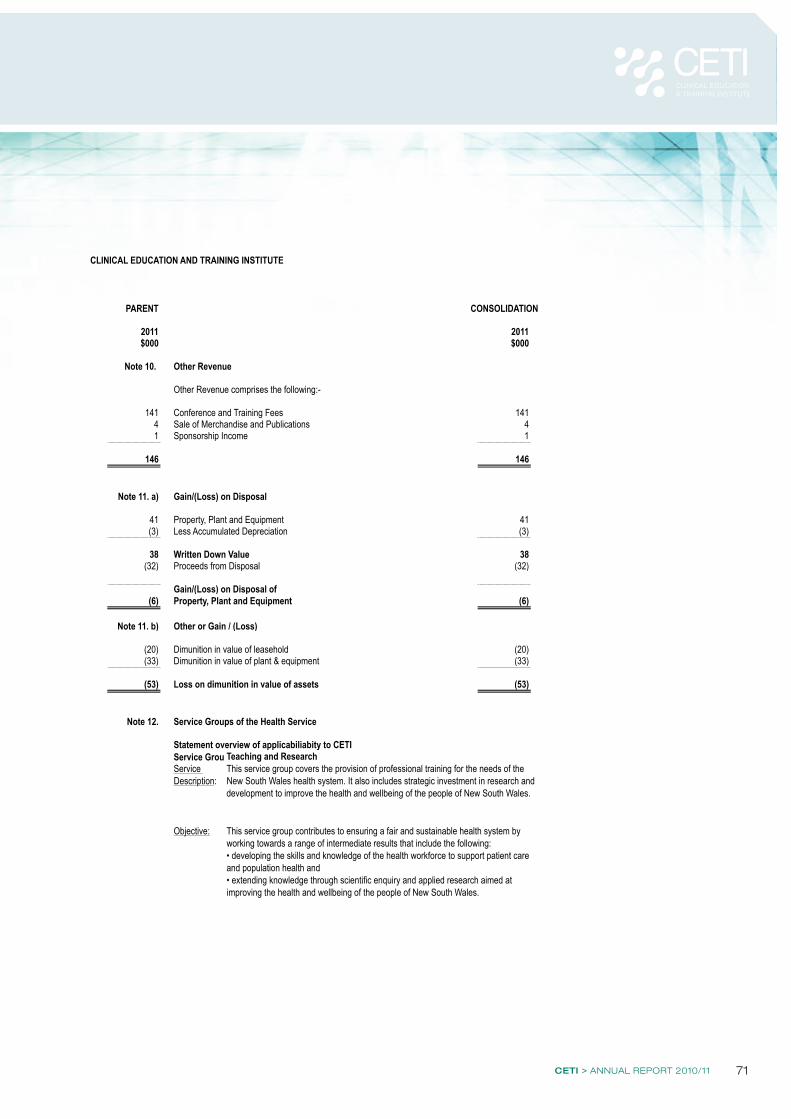
CETI > ANNUAL REPORT 2010/11 71
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 19 of 29
PARENT CONSOLIDATION
2011 2011$000 $000
Note 10. Other Revenue
Other Revenue comprises the following:-
141 Conference and Training Fees 1414 Sale of Merchandise and Publications 41 Sponsorship Income 1
146 146
Note 11. a) Gain/(Loss) on Disposal
41 Property, Plant and Equipment 41(3) Less Accumulated Depreciation (3)
38 Written Down Value 38(32) Proceeds from Disposal (32)
Gain/(Loss) on Disposal of(6) Property, Plant and Equipment (6)
Note 11. b) Other or Gain / (Loss)
(20) Dimunition in value of leasehold (20)(33) Dimunition in value of plant & equipment (33)
(53) Loss on dimunition in value of assets (53)
Note 12. Service Groups of the Health Service
Statement overview of applicabiliabity to CETIService Group 6.1 -Teaching and ResearchService Description:
Objective:
This service group covers the provision of professional training for the needs of the New South Wales health system. It also includes strategic investment in research and development to improve the health and wellbeing of the people of New South Wales.
This service group contributes to ensuring a fair and sustainable health system by working towards a range of intermediate results that include the following:• developing the skills and knowledge of the health workforce to support patient care and population health and• extending knowledge through scientific enquiry and applied research aimed at improving the health and wellbeing of the people of New South Wales.
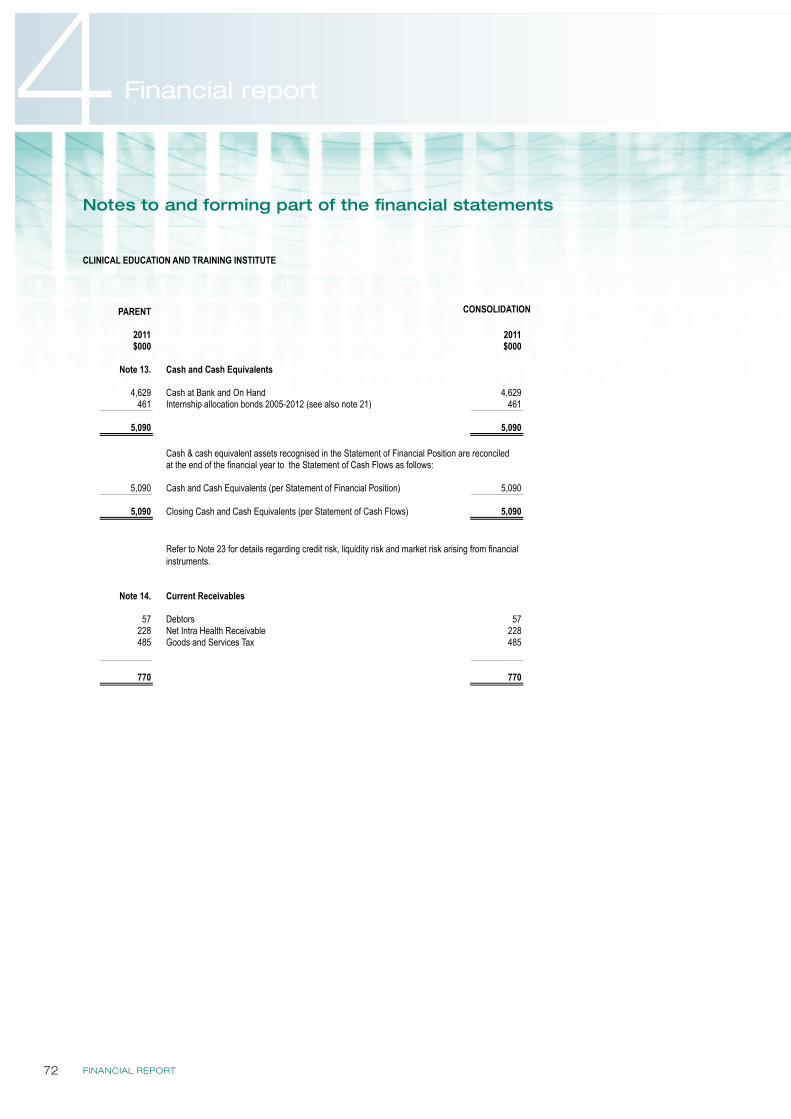
FINANCIAL REPORT72
4 Financial report
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 20 of 29
PARENT
2011 2011$000 $000
Note 13. Cash and Cash Equivalents
4,629 Cash at Bank and On Hand 4,629461 Internship allocation bonds 2005-2012 (see also note 21) 461
5,090 5,090
Cash & cash equivalent assets recognised in the Statement of Financial Position are reconciled at the end of the financial year to the Statement of Cash Flows as follows:
5,090 Cash and Cash Equivalents (per Statement of Financial Position) 5,090
5,090 Closing Cash and Cash Equivalents (per Statement of Cash Flows) 5,090
Note 14. Current Receivables
57 Debtors 57228 Net Intra Health Receivable 228485 Goods and Services Tax 485
770 770
Refer to Note 23 for details regarding credit risk, liquidity risk and market risk arising from financial instruments.
CONSOLIDATION
Notes to and forming part of the financial statements
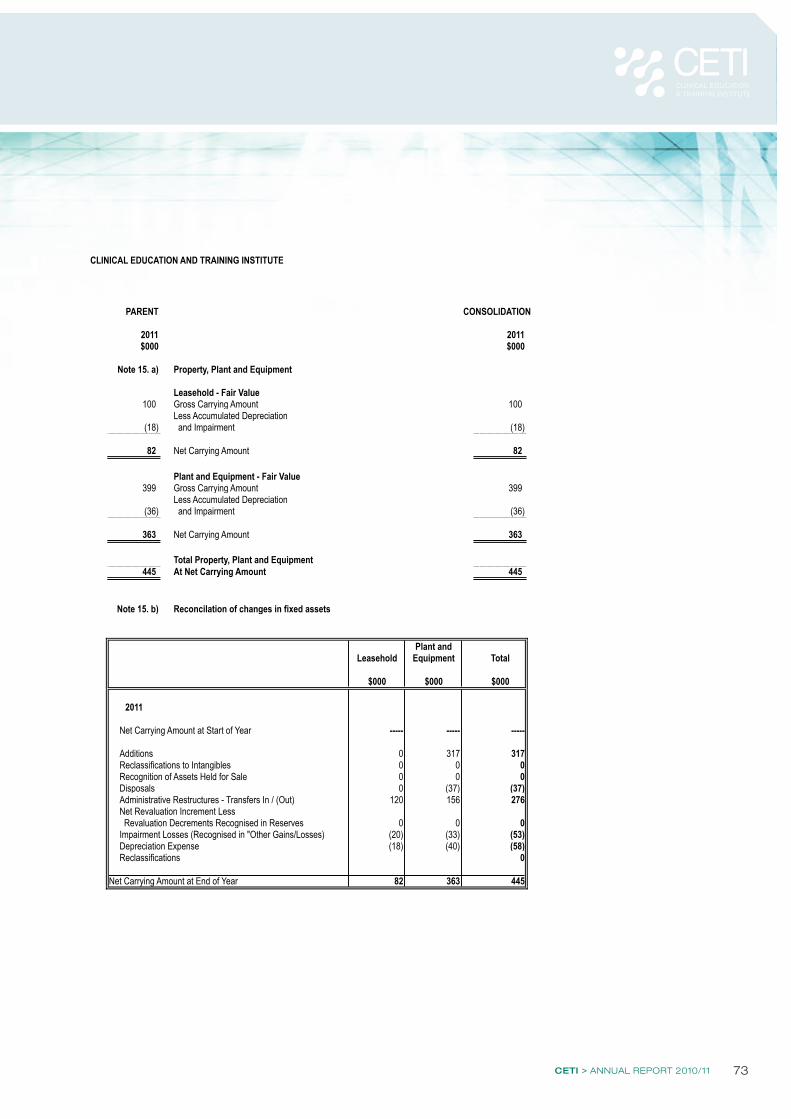
CETI > ANNUAL REPORT 2010/11 73
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 21 of 29
PARENT CONSOLIDATION
2011 2011$000 $000
Note 15. a) Property, Plant and Equipment
Leasehold - Fair Value100 Gross Carrying Amount 100
Less Accumulated Depreciation(18) and Impairment (18)
82 Net Carrying Amount 82
Plant and Equipment - Fair Value399 Gross Carrying Amount 399
Less Accumulated Depreciation(36) and Impairment (36)
363 Net Carrying Amount 363
Total Property, Plant and Equipment445 At Net Carrying Amount 445
Note 15. b) Reconcilation of changes in fixed assets
Plant andLeasehold Equipment Total
$000 $000 $000
2011
Net Carrying Amount at Start of Year ----- ----- -----
Additions 0 317 317Reclassifications to Intangibles 0 0 0Recognition of Assets Held for Sale 0 0 0Disposals 0 (37) (37)Administrative Restructures - Transfers In / (Out) 120 156 276Net Revaluation Increment Less Revaluation Decrements Recognised in Reserves 0 0 0Impairment Losses (Recognised in "Other Gains/Losses) (20) (33) (53)Depreciation Expense (18) (40) (58)Reclassifications 0
Net Carrying Amount at End of Year 82 363 445
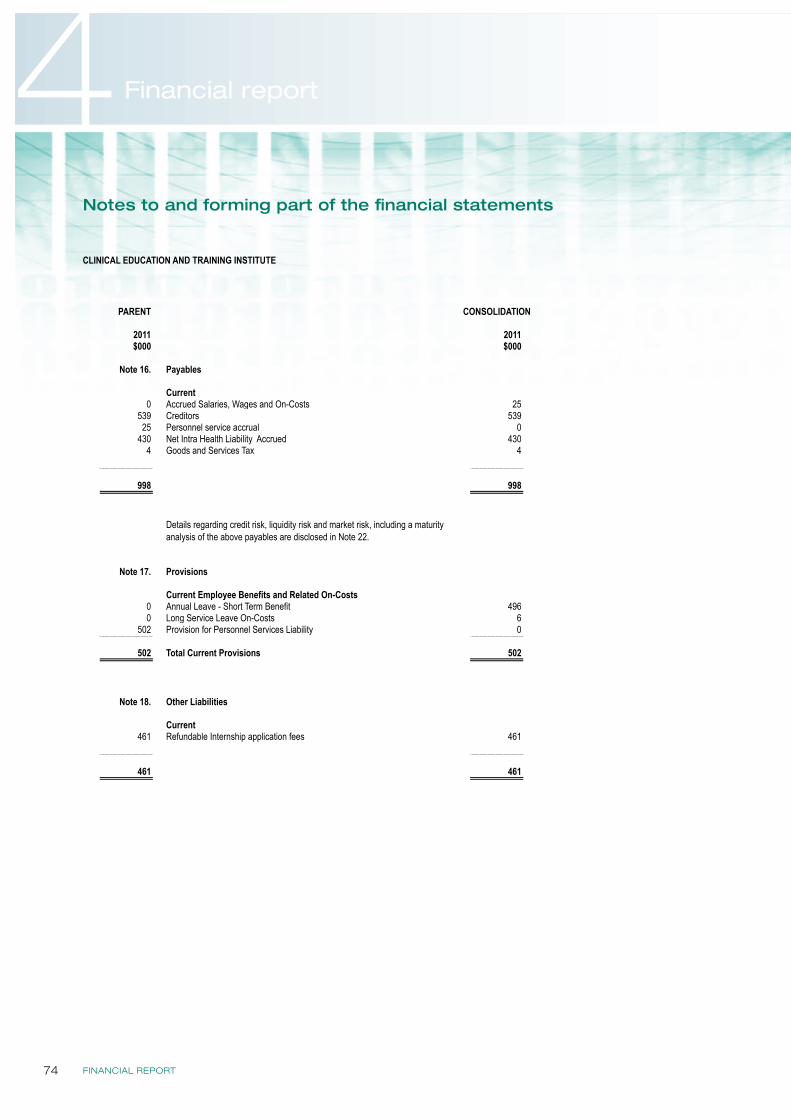
FINANCIAL REPORT74
4 Financial report
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 22 of 29
PARENT
2011 2011$000 $000
Note 16. Payables
Current0 Accrued Salaries, Wages and On-Costs 25
539 Creditors 53925 Personnel service accrual 0
430 Net Intra Health Liability Accrued 4304 Goods and Services Tax 4
998 998
Note 17. Provisions
Current Employee Benefits and Related On-Costs0 Annual Leave - Short Term Benefit 4960 Long Service Leave On-Costs 6
502 Provision for Personnel Services Liability 0
502 Total Current Provisions 502
Note 18. Other Liabilities
Current461 Refundable Internship application fees 461
461 461
CONSOLIDATION
Details regarding credit risk, liquidity risk and market risk, including a maturity analysis of the above payables are disclosed in Note 22.
Notes to and forming part of the financial statements
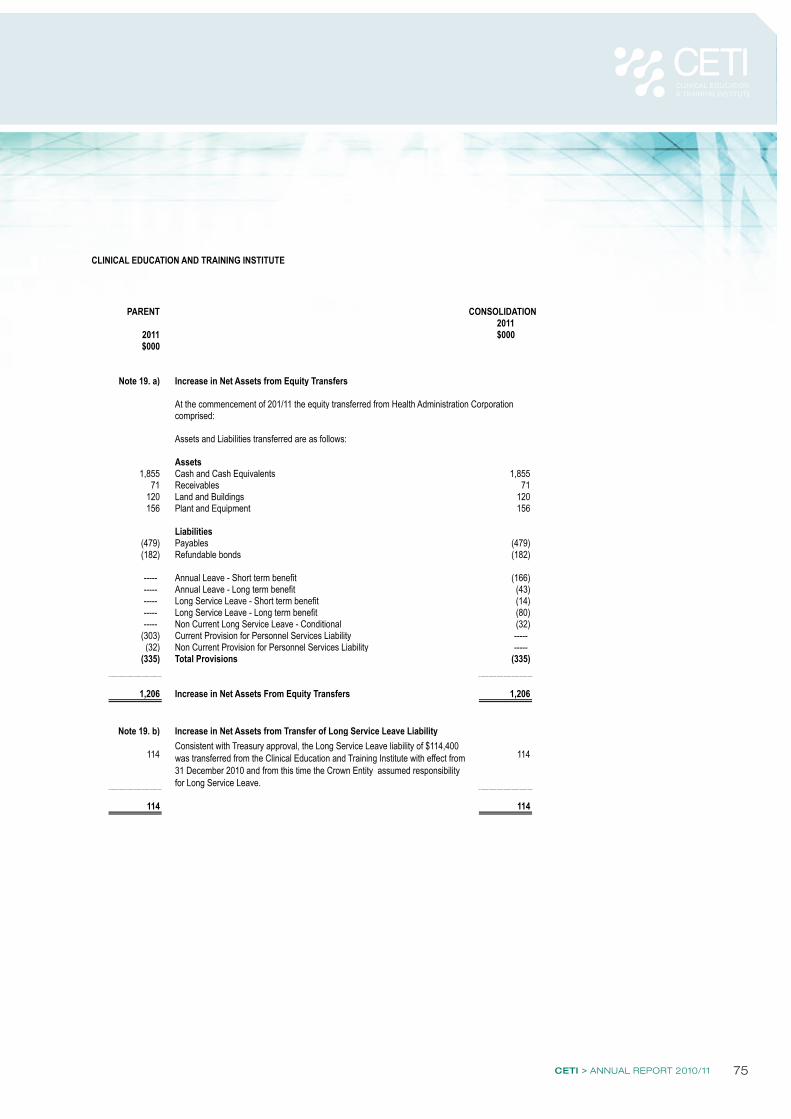
CETI > ANNUAL REPORT 2010/11 75
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 23 of 29
PARENT CONSOLIDATION2011
2011 $000$000
Note 19. a) Increase in Net Assets from Equity Transfers
At the commencement of 201/11 the equity transferred from Health Administration Corporation comprised:
Assets and Liabilities transferred are as follows:
Assets1,855 Cash and Cash Equivalents 1,855
71 Receivables 71120 Land and Buildings 120156 Plant and Equipment 156
Liabilities(479) Payables (479) (182) Refundable bonds (182)
----- Annual Leave - Short term benefit (166) ----- Annual Leave - Long term benefit (43) ----- Long Service Leave - Short term benefit (14) ----- Long Service Leave - Long term benefit (80) ----- Non Current Long Service Leave - Conditional (32)
(303) Current Provision for Personnel Services Liability ----- (32) Non Current Provision for Personnel Services Liability -----
(335) Total Provisions (335)
1,206 Increase in Net Assets From Equity Transfers 1,206
Note 19. b) Increase in Net Assets from Transfer of Long Service Leave Liability
114 114
114 114
Consistent with Treasury approval, the Long Service Leave liability of $114,400 was transferred from the Clinical Education and Training Institute with effect from 31 December 2010 and from this time the Crown Entity assumed responsibility for Long Service Leave.
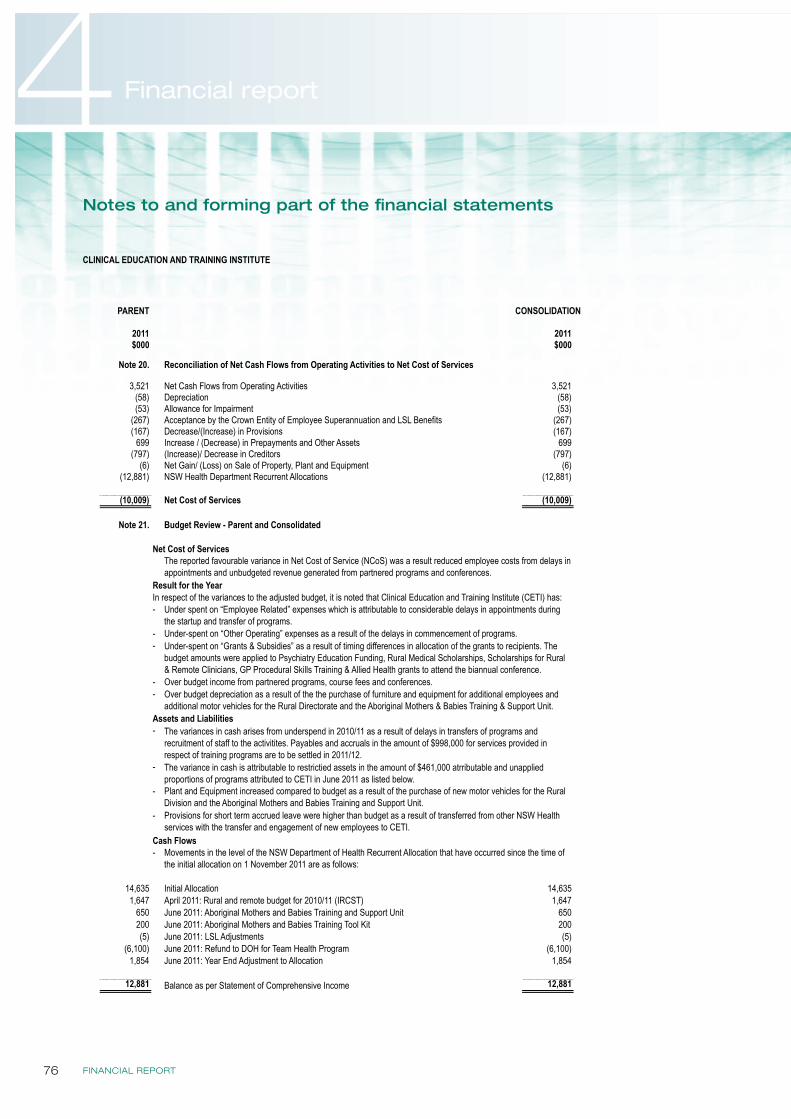
FINANCIAL REPORT76
4 Financial report
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 1 of 1
PARENT
2011 2011$000 $000
Note 20. Reconciliation of Net Cash Flows from Operating Activities to Net Cost of Services
3,521 Net Cash Flows from Operating Activities 3,521(58) Depreciation (58)(53) Allowance for Impairment (53)
(267) Acceptance by the Crown Entity of Employee Superannuation and LSL Benefits (267)(167) Decrease/(Increase) in Provisions (167)
699 Increase / (Decrease) in Prepayments and Other Assets 699(797) (Increase)/ Decrease in Creditors (797)
(6) Net Gain/ (Loss) on Sale of Property, Plant and Equipment (6)(12,881) NSW Health Department Recurrent Allocations (12,881)
(10,009) Net Cost of Services (10,009)
Note 21. Budget Review - Parent and Consolidated
Net Cost of Services
Result for the Year In respect of the variances to the adjusted budget, it is noted that Clinical Education and Training Institute (CETI) has:-
--
--
Assets and Liabilities-
-
-
-
Cash Flows-
14,635 Initial Allocation 14,6351,647 April 2011: Rural and remote budget for 2010/11 (IRCST) 1,647
650 June 2011: Aboriginal Mothers and Babies Training and Support Unit 650200 June 2011: Aboriginal Mothers and Babies Training Tool Kit 200(5) June 2011: LSL Adjustments (5)
(6,100) June 2011: Refund to DOH for Team Health Program (6,100)1,854 June 2011: Year End Adjustment to Allocation 1,854
12,881 Balance as per Statement of Comprehensive Income 12,881
Movements in the level of the NSW Department of Health Recurrent Allocation that have occurred since the time of the initial allocation on 1 November 2011 are as follows:
Over budget income from partnered programs, course fees and conferences.Over budget depreciation as a result of the the purchase of furniture and equipment for additional employees and additional motor vehicles for the Rural Directorate and the Aboriginal Mothers & Babies Training & Support Unit.
The variances in cash arises from underspend in 2010/11 as a result of delays in transfers of programs and recruitment of staff to the activitites. Payables and accruals in the amount of $998,000 for services provided in respect of training programs are to be settled in 2011/12. The variance in cash is attributable to restrictied assets in the amount of $461,000 atrributable and unapplied proportions of programs attributed to CETI in June 2011 as listed below.
CONSOLIDATION
The reported favourable variance in Net Cost of Service (NCoS) was a result reduced employee costs from delays in appointments and unbudgeted revenue generated from partnered programs and conferences.
Plant and Equipment increased compared to budget as a result of the purchase of new motor vehicles for the Rural Division and the Aboriginal Mothers and Babies Training and Support Unit. Provisions for short term accrued leave were higher than budget as a result of transferred from other NSW Health services with the transfer and engagement of new employees to CETI.
Under-spent on “Other Operating” expenses as a result of the delays in commencement of programs. Under-spent on “Grants & Subsidies” as a result of timing differences in allocation of the grants to recipients. The budget amounts were applied to Psychiatry Education Funding, Rural Medical Scholarships, Scholarships for Rural & Remote Clinicians, GP Procedural Skills Training & Allied Health grants to attend the biannual conference.
Under spent on “Employee Related” expenses which is attributable to considerable delays in appointments during the startup and transfer of programs.
Notes to and forming part of the financial statements
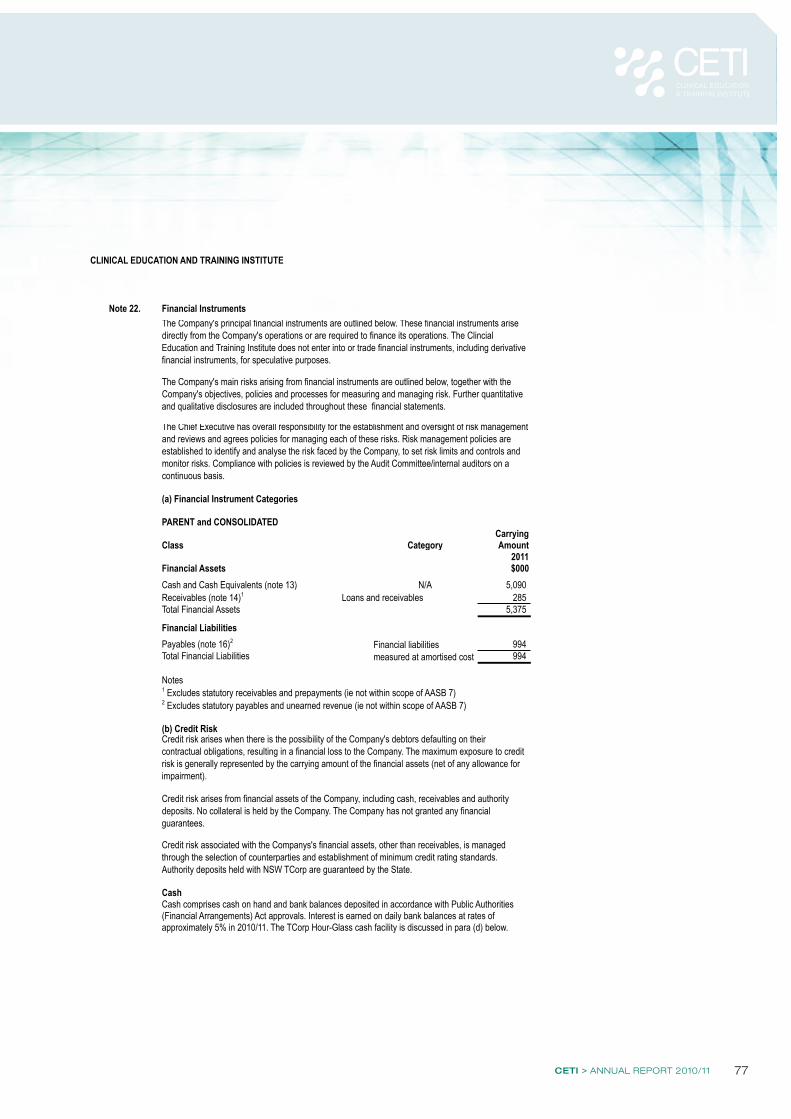
CETI > ANNUAL REPORT 2010/11 77
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 26 of 29
Note 22. Financial Instruments
(a) Financial Instrument Categories
PARENT and CONSOLIDATEDCarrying
Class Amount2011
Financial Assets $000Cash and Cash Equivalents (note 13) 5,090 Receivables (note 14)1 Loans and receivables 285 Total Financial Assets 5,375
Financial LiabilitiesPayables (note 16)2 994 Total Financial Liabilities 994
Notes1 Excludes statutory receivables and prepayments (ie not within scope of AASB 7)2 Excludes statutory payables and unearned revenue (ie not within scope of AASB 7)
(b) Credit Risk
Cash
(Financial Arrangements) Act approvals. Interest is earned on daily bank balances at rates ofapproximately 5% in 2010/11. The TCorp Hour-Glass cash facility is discussed in para (d) below.
Credit risk arises from financial assets of the Company, including cash, receivables and authority deposits. No collateral is held by the Company. The Company has not granted any financial guarantees.
Financial liabilities measured at amortised cost
Cash comprises cash on hand and bank balances deposited in accordance with Public Authorities
Credit risk associated with the Companys's financial assets, other than receivables, is managed through the selection of counterparties and establishment of minimum credit rating standards. Authority deposits held with NSW TCorp are guaranteed by the State.
The Company's principal financial instruments are outlined below. These financial instruments arise directly from the Company's operations or are required to finance its operations. The Clincial Education and Training Institute does not enter into or trade financial instruments, including derivative financial instruments, for speculative purposes.
The Company's main risks arising from financial instruments are outlined below, together with the Company's objectives, policies and processes for measuring and managing risk. Further quantitative and qualitative disclosures are included throughout these financial statements.
The Chief Executive has overall responsibility for the establishment and oversight of risk management and reviews and agrees policies for managing each of these risks. Risk management policies are established to identify and analyse the risk faced by the Company, to set risk limits and controls and monitor risks. Compliance with policies is reviewed by the Audit Committee/internal auditors on a continuous basis.
Credit risk arises when there is the possibility of the Company's debtors defaulting on their contractual obligations, resulting in a financial loss to the Company. The maximum exposure to credit risk is generally represented by the carrying amount of the financial assets (net of any allowance for impairment).
Category
N/A
FINANCIAL REPORT78
4 Financial report
CLINICAL EDUCATION AND TRAINING INSTITUTE
Page 29 of 29
23. Post balance date events
24. Commitments for Expenditure
(a) Capital Commitments
The company has no capital commitements.
(b) Other Expenditure Commitments
The company has no contracted commitments for other expenditures.
(c) Operating Lease Commitments
The company has no non-cancellable operating leases.
25. Contingent Liabilities and Assets
END OF AUDITED FINANCIAL STATEMENTS
Workers Compensation Hindsight Adjustment
Treasury Managed Fund normally calculates hindsight premiums each year. As this was the first year of operations, it is not possible for the Clincial Education and Training Institute to reliably quantify the workers compensation obligation.
PARENT AND CONSOLIDATED
There are no significant issues that have arisen subsequent to balance date that would require these finacnial statements to be amended.
However, consistent with the revised Governance Framework theme of "investment in our people" CETI will be renamed as the Health Education and Training Institute with expanded responsibilities for undergraduate clincial placements, vocational education and training and management and leadership capacity development.
Notes to and forming part of the financial statements
CETI > ANNUAL REPORT 2010/11 79
Certification of financial statements (Special Purpose Entity)
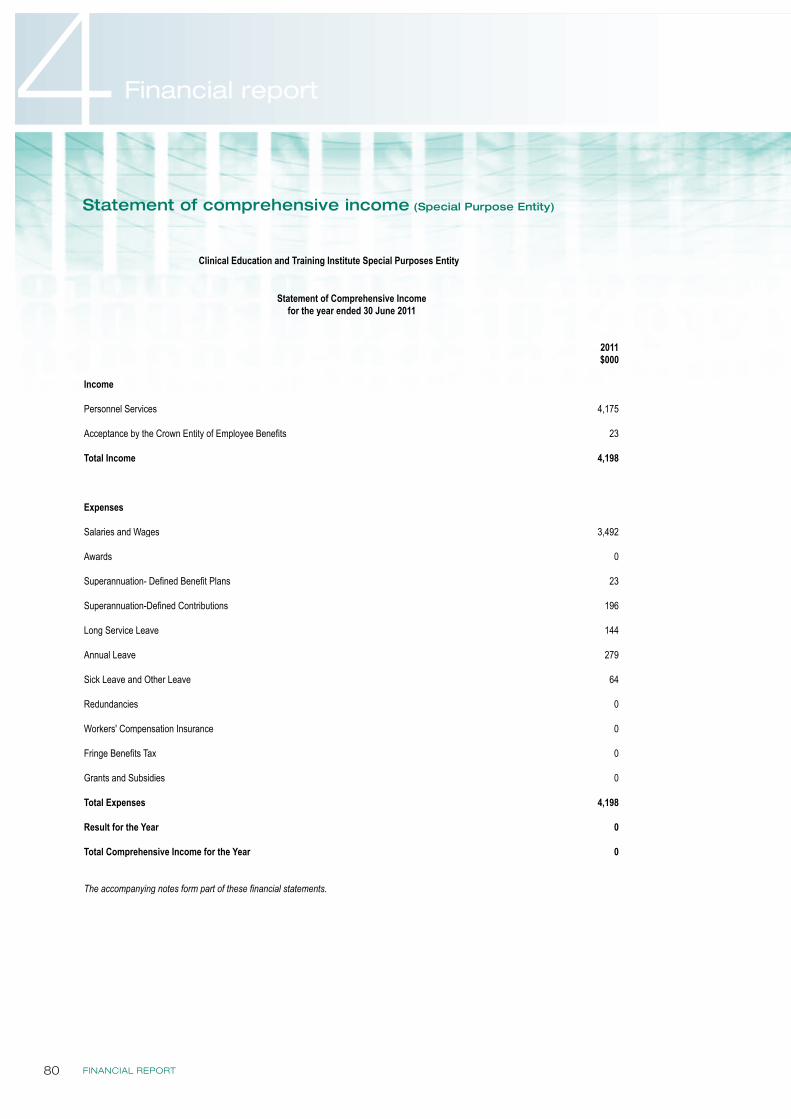
FINANCIAL REPORT80
4 Financial report
Statement of comprehensive income (Special Purpose Entity)
Clinical Education and Training Institute Special Purposes Entity
Page 1 of 1
2011$000
Income
Personnel Services 4,175
Acceptance by the Crown Entity of Employee Benefits 23
Total Income 4,198
Expenses
Salaries and Wages 3,492
Awards 0
Superannuation- Defined Benefit Plans 23
Superannuation-Defined Contributions 196
Long Service Leave 144
Annual Leave 279
Sick Leave and Other Leave 64
Redundancies 0
Workers' Compensation Insurance 0
Fringe Benefits Tax 0
Grants and Subsidies 0
Total Expenses 4,198
Result for the Year 0
Total Comprehensive Income for the Year 0
The accompanying notes form part of these financial statements.
Statement of Comprehensive Incomefor the year ended 30 June 2011
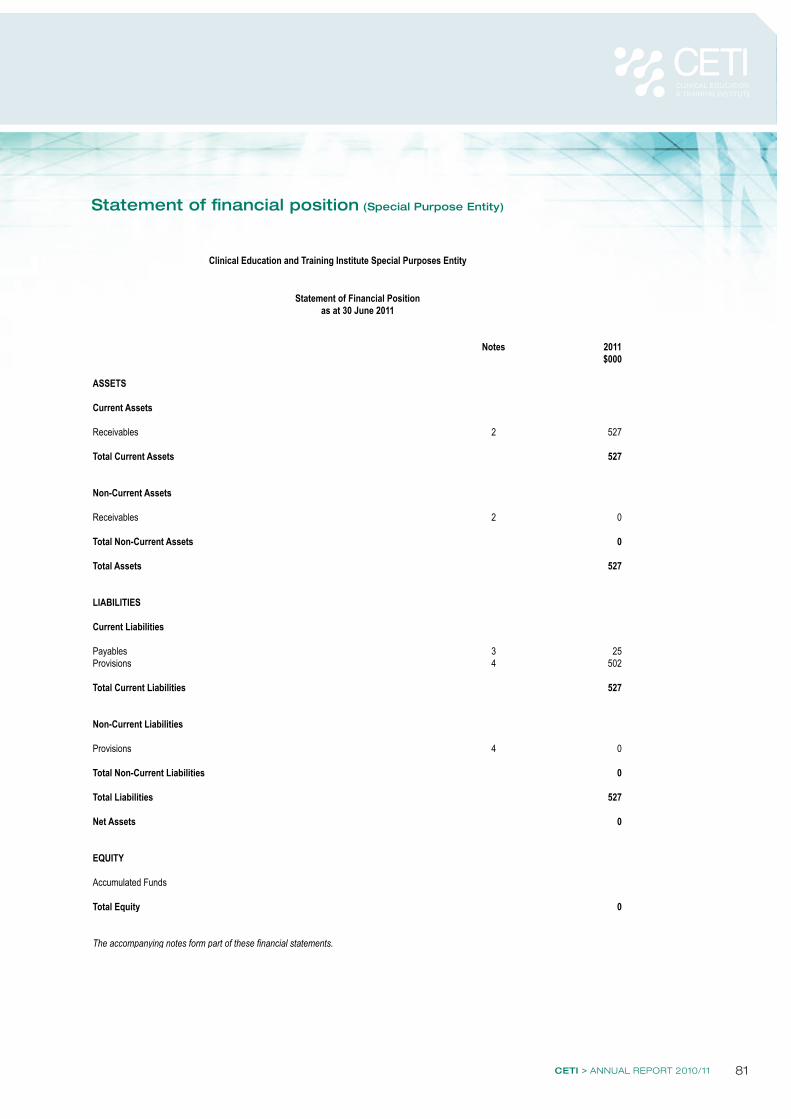
CETI > ANNUAL REPORT 2010/11 81
Statement of financial position (Special Purpose Entity)
Clinical Education and Training Institute Special Purposes Entity
Page 3 of 14
Notes 2011$000
ASSETS
Current Assets
Receivables 2 527
Total Current Assets 527
Non-Current Assets
Receivables 2 0
Total Non-Current Assets 0
Total Assets 527
LIABILITIES
Current Liabilities
Payables 3 25Provisions 4 502
Total Current Liabilities 527
Non-Current Liabilities
Provisions 4 0
Total Non-Current Liabilities 0
Total Liabilities 527
Net Assets 0
EQUITY
Accumulated Funds
Total Equity 0
The accompanying notes form part of these financial statements.
Statement of Financial Positionas at 30 June 2011
FINANCIAL REPORT82
4 Financial report
Certification of changes in equity (Special Purpose Entity)
Clinical Education and Training Institute Special Purposes Entity
Page 4 of 14
2011 $000
Balance at 1 July 0
Result for the Year 0
Total Comprehensive Income for the Year 0
Balance at 30 June 0
The accompanying notes form part of these financial statements.
Statement of Changes in Equityfor the year ended 30 June 2011
CETI > ANNUAL REPORT 2010/11 83
Statement of cash flows (Special Purpose Entity)
Clinical Education and Training Institute Special Purposes Entity
Page 1 of 1
2011$000
Net Cash Flows from Operating Activities 0
Net Cash Flows from Investing Activities 0
Net Cash Flows from Financing Activities 0
Net Increase/(Decrease) in Cash 0
Opening Cash and Cash Equivalents 0
Closing Cash and Cash Equivalents 0
The Clinical Education and Training Institute Special Purpose Service Entity does not hold any cash or cash equivalent assets and therefore there are nil cash flows.
The accompanying notes form part of these financial statements.
Statement of Cash Flowsfor the year ended 30 June 2011
FINANCIAL REPORT84
4 Financial report
Notes to and forming part of the financial statements (Special Purpose Entity)
Clinical Education and Training Institute Special Purposes Entity
Page 6 of 14
1.a)
b)
c)
d)
Management's judgments, key assumptions and estimates are disclosed in the relevant notes to the financial statements.
Basis of Preparation
The Entity's objective is to provide personnel services to the Clinical Education and Training Institute. The reporting entity is consolidated as part of the NSW Department of Health and NSW Total State Sector Accounts. The financial statements were authorised for issue by the Chief Executive on 28 September 2011.
The consolidated and parent entity's financial statements comply with Australian Accounting Standards which include Australian Accounting Interpretations .
Statement of Compliance
Notes to and forming part of the Financial Statements for the year ended 30 June 2011
AASB 2010-07, Financial Instruments,arising from the issuance of AASB 9, Financial Instruments, in AASB 2009-5 in December 2010, has mandatory application from 1 July 2013 and will not be early adopted by the Clinical Education and Training Institute.
AASB 124 and AASB2009-12, Related Party Transactions, have application from 1 July 2011 but are assessed as having no material impact on the Clinical Education and Training Institute.
Accounting Standard/Interpretation
The Entity's financial statements are general purpose financial statements which have been prepared in accordance with the requirements of Australian Accounting Standards (which include Australian Accounting Interpretations), the requirements of the Health Services Act 1997 and its regulations including observation of the Accounts and Audit Determination for Public Health Organisations.
Generally, the historical cost basis of accounting has been adopted and the financial statements do not take into account changing money values or current valuations. However, certain provisions are measured at fair value. See note (j).
The accrual basis of accounting has been adopted in the preparation of the financial statements, except for cash flow information.
New Australian Accounting Standards Issued But Not Effective
SUMMARY OF SIGNIFICANT ACCOUNTING POLICIESClinical Education and Training Institute Special Purpose Service Entity
Comparative Information
Comparative figures are, where appropriate, reclassified to give meaningful comparison with the current year.
All amounts are rounded to the nearest one thousand dollars and are expressed in Australian currency.
No new or revised accounting standards or interpretations are adopted earlier than their prescribed date of application. Set out below are changes to be effected, their date of application and the possible impact on the financial statements of the Clinical Education and Training Institute Special Purpose Service Entity.
The Clinical Education and Training Institute Special Purpose Service Entity "the Entity", is a Division of the Government Service, established pursuant to Part 2 of Schedule 1 to the Public Sector Employment and Management Act 2002 and amendment of the Clinical Education and Training Institutes Act 1997. It is a not-for-profit entity as profit is not its principal objective. It is consolidated as part of the NSW Total State Sector Accounts. It is domiciled in Australia and its principal office is at Gladesville, New South Wales.
CETI > ANNUAL REPORT 2010/11 85
Clinical Education and Training Institute Special Purposes Entity
Page 7 of 14
e)
f)
g)
**
Income is measured at the fair value of the consideration received or receivable. Revenue from the rendering of personnel services is recognised when the service is provided and only to the extent that the associated recoverable expenses are recognised.
Receivables are non-derivative financial assets with fixed or determinable payments that are not quoted in an active market. These financial assets are recognised initially at fair value, usually based on the transaction cost or face value. Subsequent measurement is at amortised cost using the effective interest method, less an allowance for any impairment of receivables. Any changes are accounted for in the statement of comprehensive income when impaired, derecognised or through the amortisation process.
Short-term receivables with no stated interest rate are measured at the original invoice amount where the effect of discounting is immaterial.
AASB 2009-14, Amendments to Australian Interpretation -Prepayment of a Minimum Funding Requirement, has application from 1 July 2011 and principally addresses contributions relating to future service.It has no impact on the Clinical Education and Training Institute.
AASB 2010-04, Annual Improvements,has application from 1July 2011 and is assessed as having no material impact on the Clinical Education and Training Institute.
AASB 2010-5, Editorial Corrections, applies from 1 July 2011 and principally addresses editorial amendments to a range of Australian Accounting Standards and Interpretations.It is assessed as having no impact on the Clinical Education and Training Institute.
AASB 2010-6 , Disclosures on Transfers of Financial Assets, has mandatory application from 1 July 2011 and is assessed as having no impact on the Clinical Education and Training Institute.
AASB 1053 and AASB 2010-2, Application of Tiers of Australian Accounting Standards, have application from 1 July 2013 and may result in a lessening of reporting requirements, dependent on the mandate of Treasury.
AASB 2010-10, Removal of Fixed Dates for First Time Adopters, has application from 1 July 2013 and is assessed as having no impact on the Clinical Education and Training Institute.
AASB 2010-8, Deferred Tax:Recovery of Underlying Assets, has mandatory application from 1 July 2012 but will have no impact on the Clinical Education and Training Institute.
Notes to and forming part of the Financial Statements for the year ended 30 June 2011
where the Entity has not transferred substantially all the risks and rewards,if the Entity has not retained control.
AASB 2010-9, Severe Hyperinflation and Removal of Fixed Dates for First Time Adopters, has application from 1 July 2011 and is assessed as having no impact on the Clinical Education and Training Institute.
De-recognition of Financial Assets and Financial Liabilities
A financial asset is derecognised when the contractual rights to the cash flows from the financial assets expire: or if the agency expire; or if the Entity transfers the financial asset:
where substantially all the risks and rewards have been transferred; or
Where the Entity has neither transferred nor retained substantially all the risks and rewards or transferred control, the asset is recognised to the extent of the Entity's continuing involvement in the asset. A financial liability is derecognised when the obligation specified in the contract is discharged or cancelled or expires.
Receivables
Income Recognition
FINANCIAL REPORT86
4 Financial report
Clinical Education and Training Institute Special Purposes Entity
Page 8 of 14
h)
i)
i)
ii)
Notes to and forming part of the Financial Statements for the year ended 30 June 2011
A payable is recognised when a present obligation arises under a contract or otherwise. It is derecognisedwhen the obligation expires or is discharged, cancelled or substituted.
Payables are recognised initially at fair value, usually based on the transaction cost or face value. Subsequent measurement is at amortised cost using the effective interest method. Short-term payables with no stated interest rate are measured at the original invoice amount where the effect of discounting is immaterial. Payables are recognised for amounts to be paid in the future for goods and services received, whether or not billed to the Entity.
All Annual Leave employee benefits are reported as "Current" as there is an unconditional right to payment. Current liabilities are then classified as "Short Term" and "Long Term" based on past trends and known resignations and retirements. Anticipated payments to be made in the next 12 months are reported as "Short Term".
Long Service Leave and Superannuation
Employee Benefits
Unused non-vesting sick leave does not give rise to a liability as it is not considered probable that sick leave taken in the future will be greater than the benefits accrued in the future.
The outstanding amounts of workers' compensation insurance premiums and fringe benefits tax, which are consequential to employment, are recognised as liabilities and expenses where the employee benefits to which they relate have been recognised.
The superannuation expense for the financial year is determined by using the formulae specified by the NSW Department of Health. The expense for certain superannuation schemes (ie Basic Benefit and First State Super) is calculated as a percentage of the employees' salary. For other superannuation schemes (ie State Superannuation Scheme and State Authorities Superannuation Scheme), the expense is calculated as a multiple of the employees' superannuation contributions.
Liabilities for salaries and wages (including non-monetary benefits), annual leave and paid sick leave that are due within 12 months after the end of the period in which the employees render the service are recognised and measured in respect of employees' services up to the reporting date at undiscounted amounts based on the amounts expected to be paid when the liabilities are settled.
Payables
Payables include accrued wages, salaries and related on-costs (such as payroll deduction liability, fringe benefits tax and workers' compensation insurance) where there is certainty as to the amount and timing of settlement.
Responsibility for Long Service Leave liability transferred to the Crown Entity with effect from 31 December 2010. As is the case with other Budget Sector agencies both the Defined Benefit Superannuation (State Authorities Superannuation Scheme and State Superannuation Scheme) and Long Service Leave liabilities are now assumed by the Crown Entity.
Long Service Leave is measured at present value in accordance with AASB119, Employee Benefits. This is based on the application of certain factors (specified in NSW Treasury Circular 11/06) to employees with five or more years of service, using current rates of pay. These approximate present value.
The Clinical Education and Training Institute's liability for the closed superannuation pool schemes (State Authorities Superannuation Scheme and State Superannuation Scheme) is assumed by the Crown Entity. The Clinical Education and Training Institute accounts for the liability as having been extinguished resulting int he amount shown as part of the non-monetary revenue item described as "Acceptance by the Crown Entity of Employee Benefits". Any liability attached to Superannuation Guarantee Charge cover is reported in Note 3, "Payables".
Salaries and Wages, Annual Leave, Sick Leave and On-Costs
Notes to and forming part of the financial statements (Special Purpose Entity)
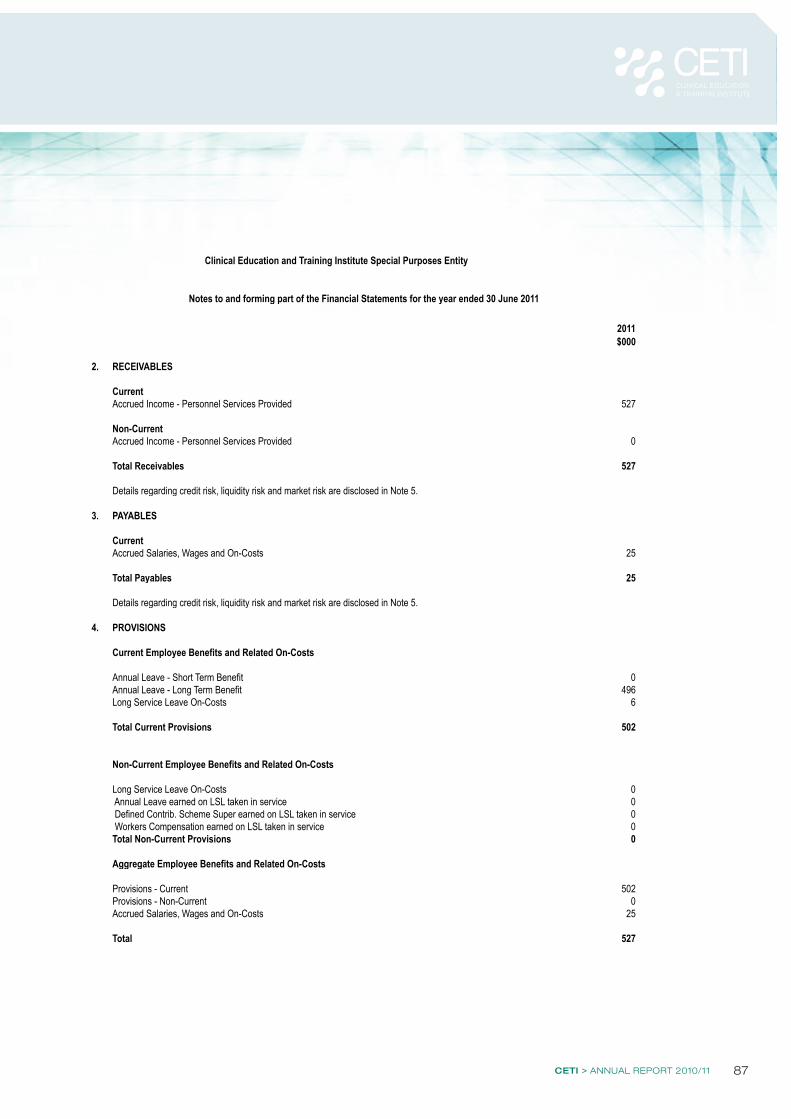
CETI > ANNUAL REPORT 2010/11 87
Clinical Education and Training Institute Special Purposes Entity
Page 9 of 14
2011$000
2. RECEIVABLES
CurrentAccrued Income - Personnel Services Provided 527
Non-CurrentAccrued Income - Personnel Services Provided 0
Total Receivables 527
3. PAYABLES
CurrentAccrued Salaries, Wages and On-Costs 25
Total Payables 25
4. PROVISIONS
Current Employee Benefits and Related On-Costs
Annual Leave - Short Term Benefit 0Annual Leave - Long Term Benefit 496Long Service Leave On-Costs 6
Total Current Provisions 502
Non-Current Employee Benefits and Related On-Costs
Long Service Leave On-Costs 0 Annual Leave earned on LSL taken in service 0 Defined Contrib. Scheme Super earned on LSL taken in service 0 Workers Compensation earned on LSL taken in service 0Total Non-Current Provisions 0
Aggregate Employee Benefits and Related On-Costs
Provisions - Current 502Provisions - Non-Current 0Accrued Salaries, Wages and On-Costs 25
Total 527
Notes to and forming part of the Financial Statements for the year ended 30 June 2011
Details regarding credit risk, liquidity risk and market risk are disclosed in Note 5.
Details regarding credit risk, liquidity risk and market risk are disclosed in Note 5.
FINANCIAL REPORT88
4 Financial report
Clinical Education and Training Institute Special Purposes Entity
Page 1 of 4
Note 5 Financial Instruments
The Chief Executive has overall responsibility for the establishment and oversight of risk managementand reviews and agrees policies for managing each of these risks. The Entity carries minimal risks within
monitor risks. Compliance with policies is reviewed by the Audit Committee/internalauditors of the Parent Entity on a continuous basis.
a) Financial Instruments Categories
2011$000
Financial Assets
Class:Receivables (note 2)1 Receivables measured 526
at amortised costTotal Financial Assets 526
Financial Liabilities
Class:Payables (note 3)₂ Financial liabilities
measured at 24amortised cost
Total Financial Liabilities 24
2 Excludes statutory payables and unearned revenue (i.e. not within scope of AASB7)
b) Credit Risk
Credit risk arises when there is the possibility of the Entity's debtors defaulting on theircontractual obligations, resulting in a financial loss to the Entity. The maximum exposureto credit risk is generally represented by the carrying amount of the financial assets (net of anyallowance for impairment).
Notes to and forming part of the Financial Statements for the year ended 30 June 2011
Financial instruments arise directly from operations or are required to finance its operations. The Entity does not enter into or trade financial instruments, including derivative financial instruments, for speculative purposes.
Category
Category
The Entity's main risks arising from financial instruments are outlined below, together with the Entity's objectives, policies and processes for measuring and managing risk. Further quantitative and qualitative disclosures are included throughout these financial statements.
Total carrying amounts as perthe Statement of Financial Position
its operation as it carries only the value of employee provisions and accrued salaries and wages offset infull by accounts receivable from the Parent Entity. Risk management policies are established by the Parent Entity to identify and analyse the risk faced by the Entity, to set risk limits and controls and
1 Excludes statutory receivables and prepayments, (i.e. not within the scope of AASB 7)
Notes to and forming part of the financial statements (Special Purpose Entity)
CETI > ANNUAL REPORT 2010/11 89
Clinical Education and Training Institute Special Purposes Entity
Page 2 of 4
nor has it granted any financial guarantees.
Receivables - trade debtors
Receivables are restricted to accrued income for personnel services provided and employee leave provisions and are recognised as amounts receivable at balance date. The parent entity of the Clinical Education and Training Institute Special Purpose Service Entity is the sole debtor of the Entity and it is assessed that there is no risk of default. No accounts receivables are classified as "Past Due but not Impaired"
c) Liquidity Risk
Liquidity risk is the risk that the Entity will be unable to meet its payment obligations when they fall due. No such risk exists with the Entity not having any cash flows. All movements that occur in Payablesare fully offset by an increase in Receivables from the Clinical Education and Training Institute parent entity.
d) Market Risk
Market risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in market prices. The Entity's exposures to market risk are considered to be minimaland the Entity has no exposure to foreign currency risk and does not enter into commodity contracts.
Interest rate risk
Exposure to interest rate risk arises primarily through interest bearing liabilities.
that the Entity is not exposed to other price risks.
e) Fair Value
Financial instruments are generally recognised at cost.
The amortised cost of financial instruments recognised in the Statement of Financial Position approximatesfair value because of the short term nature of the financial instruments.
Note 6 Related Parties
Note 7 Post Balance Date Events
No post balance date events have occurred which warrant inclusion in this report.
Notes to and forming part of the Financial Statements for the year ended 30 June 2011
However the Entity has no such liabilities and the interest rate is assessed as Nil. Similarly it is considered
incorporated under the Health Services Act 1997. Transactions and balances in this financial report relate Purpose Service Entity in accordance with Australian Accounting Standards. The controlling entity is
Cash receipts and payments are effected by the Clinical Education and Training Institute on the Entity's behalf.
only to the Entity's function as provider of personnel services to the controlling entity.
The Clinical Education and Training Institute is deemed to control the Clinical Education and Training Institute Special
END OF AUDITED FINANCIAL STATEMENTS
The Entity's total income is sourced from the Clinical Education and Training Institute.
or "Considered Impaired".
Credit risk arises from financial assets of the Entity i.e receivables. No collateral is held by the Entity
APPENDICES90
5 Appendices
Funds granted to non-government community organisationsPurpose Organisation Amount
Promotion of CETI and internship in NSW to Australian Medical Students
Australian Medical Student Association Annual Convention
$1,500
Gold sponsor to promote simulation in learning – a key component of clinical learning and CETI programs
SimHealth Conference $15,000
Promotion of the NSW Building Rural Research Capacity Program
Rural Health Research Colloquium $20,000
Legal changeThe Clinical Education and Training Institute (CETI) was established as a Statutory Corporation in accordance with the Health Services Act 1997 with effect from 1 July 2010. At its commencement CETI took over the activities of the NSW Institute of Medical Education and Training, a unit of the Health Administration Corporation and the NSW Institute of Rural Clinical Services and Teaching (IRCST), a unit of the NSW Department of Health.
Economic or other factorsThere were no economic factors affecting the achievement of objectives in 2010 and 2011. There were limitations resulting from the constraints on recruitment of permanent employees to the programs and responsibilities associated with the functions of CETI. These limitations impacted on the whole of NSW Health during the period of restructuring associated with the changes in state government.
Research and developmentCETI funds research and practice improvement through our Rural Research Capacity Building Program. Staff from all rural LHDs in NSW are invited to participate and are awarded a place based on their readiness to undertake a research project, the relevance of the research to advancing rural health and support from their LHD. The goal of this program is to promote skills in evaluation and research methods while actively contributing to the literature on both innovation and evidence-based practice around rural and remote health care. A total of $318,000 was expended on research programs during 2010-2011.
Human ResourcesCategory Employees Contractors Total
Male 13.0 9.0 22.0
Female 39.0 4.0 43.0
FTE male 10.9 1.8 12.7
FTE female 34.9 1.6 36.5
Sydney Metro 41.0 13.0 54.0
NSW regional 11.0 0.0 11.0
Clinical chairs & directors 2.0 11.0 13.0
HSM5 + 6.0 0.0 6.0
Managers 32.0 1.0 33.0
Support 12.0 1.0 13.0
CETI engages part-time clinical chairs to lead committees and provide expert input. A number of experts also provide their services on a volunteer basis. These vocational and program related committees monitor and evaluate the training programs and standards of practice in delivery, education and continuing professional development.
Compliance requirements
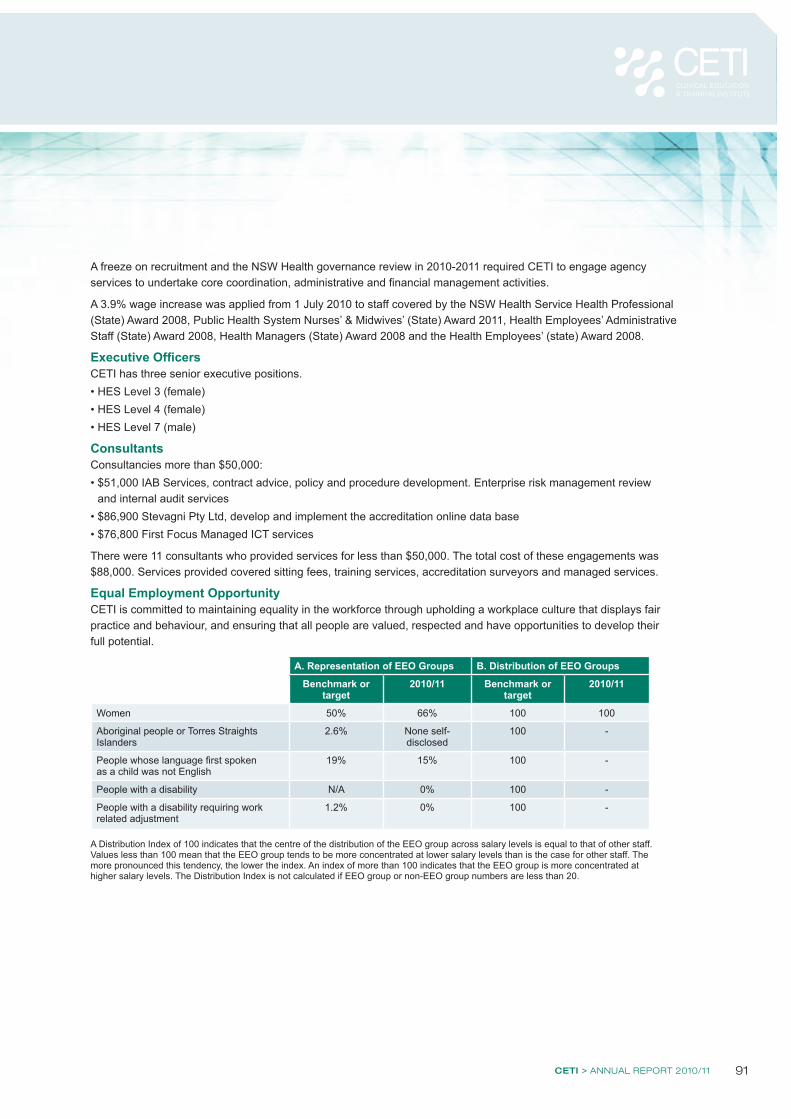
CETI > ANNUAL REPORT 2010/11 91
A freeze on recruitment and the NSW Health governance review in 2010-2011 required CETI to engage agency services to undertake core coordination, administrative and financial management activities.
A 3.9% wage increase was applied from 1 July 2010 to staff covered by the NSW Health Service Health Professional (State) Award 2008, Public Health System Nurses’ & Midwives’ (State) Award 2011, Health Employees’ Administrative Staff (State) Award 2008, Health Managers (State) Award 2008 and the Health Employees’ (state) Award 2008.
Executive OfficersCETI has three senior executive positions. • HES Level 3 (female)• HES Level 4 (female)• HES Level 7 (male)
ConsultantsConsultancies more than $50,000:• $51,000 IAB Services, contract advice, policy and procedure development. Enterprise risk management review
and internal audit services• $86,900 Stevagni Pty Ltd, develop and implement the accreditation online data base• $76,800 First Focus Managed ICT services
There were 11 consultants who provided services for less than $50,000. The total cost of these engagements was $88,000. Services provided covered sitting fees, training services, accreditation surveyors and managed services.
Equal Employment OpportunityCETI is committed to maintaining equality in the workforce through upholding a workplace culture that displays fair practice and behaviour, and ensuring that all people are valued, respected and have opportunities to develop their full potential.
A. Representation of EEO Groups B. Distribution of EEO Groups
Benchmark or target
2010/11 Benchmark or target
2010/11
Women 50% 66% 100 100
Aboriginal people or Torres Straights Islanders
2.6% None self-disclosed
100 -
People whose language first spoken as a child was not English
19% 15% 100 -
People with a disability N/A 0% 100 -
People with a disability requiring work related adjustment
1.2% 0% 100 -
A Distribution Index of 100 indicates that the centre of the distribution of the EEO group across salary levels is equal to that of other staff. Values less than 100 mean that the EEO group tends to be more concentrated at lower salary levels than is the case for other staff. The more pronounced this tendency, the lower the index. An index of more than 100 indicates that the EEO group is more concentrated at higher salary levels. The Distribution Index is not calculated if EEO group or non-EEO group numbers are less than 20.
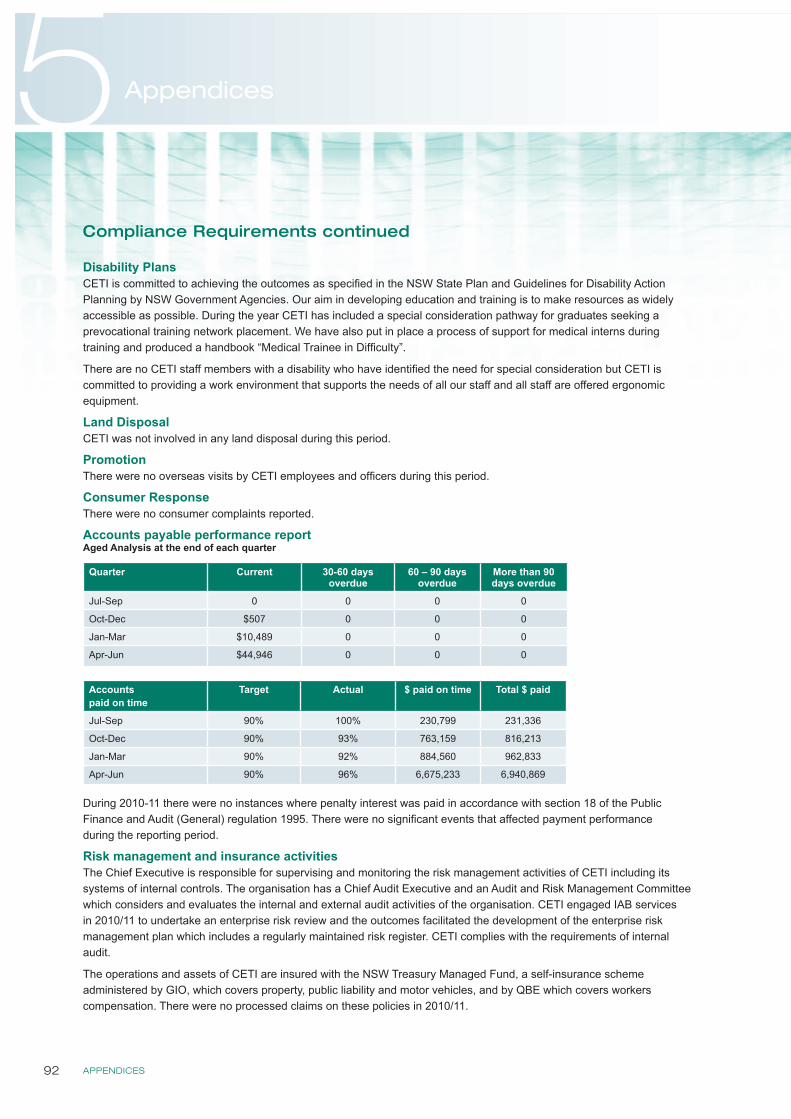
APPENDICES92
5 Appendices
Disability PlansCETI is committed to achieving the outcomes as specified in the NSW State Plan and Guidelines for Disability Action Planning by NSW Government Agencies. Our aim in developing education and training is to make resources as widely accessible as possible. During the year CETI has included a special consideration pathway for graduates seeking a prevocational training network placement. We have also put in place a process of support for medical interns during training and produced a handbook “Medical Trainee in Difficulty”.
There are no CETI staff members with a disability who have identified the need for special consideration but CETI is committed to providing a work environment that supports the needs of all our staff and all staff are offered ergonomic equipment.
Land DisposalCETI was not involved in any land disposal during this period.
PromotionThere were no overseas visits by CETI employees and officers during this period.
Consumer ResponseThere were no consumer complaints reported.
Accounts payable performance reportAged Analysis at the end of each quarter
Quarter Current 30-60 days overdue
60 – 90 days overdue
More than 90 days overdue
Jul-Sep 0 0 0 0
Oct-Dec $507 0 0 0
Jan-Mar $10,489 0 0 0
Apr-Jun $44,946 0 0 0
Accounts paid on time
Target Actual $ paid on time Total $ paid
Jul-Sep 90% 100% 230,799 231,336
Oct-Dec 90% 93% 763,159 816,213
Jan-Mar 90% 92% 884,560 962,833
Apr-Jun 90% 96% 6,675,233 6,940,869
During 2010-11 there were no instances where penalty interest was paid in accordance with section 18 of the Public Finance and Audit (General) regulation 1995. There were no significant events that affected payment performance during the reporting period.
Risk management and insurance activitiesThe Chief Executive is responsible for supervising and monitoring the risk management activities of CETI including its systems of internal controls. The organisation has a Chief Audit Executive and an Audit and Risk Management Committee which considers and evaluates the internal and external audit activities of the organisation. CETI engaged IAB services in 2010/11 to undertake an enterprise risk review and the outcomes facilitated the development of the enterprise risk management plan which includes a regularly maintained risk register. CETI complies with the requirements of internal audit.
The operations and assets of CETI are insured with the NSW Treasury Managed Fund, a self-insurance scheme administered by GIO, which covers property, public liability and motor vehicles, and by QBE which covers workers compensation. There were no processed claims on these policies in 2010/11.
Compliance Requirements continued
CETI > ANNUAL REPORT 2010/11 93
Disclosure of Controlled EntitiesCETI does not have any controlled entities.
Disclosure of subsidiariesCETI does not have any subsidiaries.
Multicultural Policies and Services ProgramCETI endorses the multicultural principles contained within the Community Relations Commission and Principles of Multiculturalism Act 2000 and the policies of NSW Health.
Specific activities undertaken in the period include:• In accordance with NSW Health policy, CETI is committed to applying the Aboriginal Health Impact Statement when
developing or reviewing significant policies and programs, and implement agreed actions to support the delivery of services and programs to Aboriginal people in NSW
• CETI funded, recruited, and managed a Rural Aboriginal Clerical Trainee from January 2011 to May 2011 who was employed by Greater Western Area Health Service (GWAHS) under a special arrangement
• CETI funded, recruited and managed two Aboriginal staff members from February 2011 for our Teaching and Support Unit for Aboriginal Mothers, Babies and Children (TSU). These staff members were employed by GWAHS under a special arrangement
• All staff involved in the TSU actively uphold and apply cultural protocols• CETI makes available special arrangements for Aboriginal medical graduates in our intern allocation process
Our key multicultural strategies for 2011-2012 include the following:• Continue to fund positions for Aboriginal workers• Continue to offer special intern allocation arrangements for Aboriginal medical graduates• Increase the Aboriginal workforce participation rate in the Specialist Training Program (STP)
Occupational Health and SafetyTwo staff reported incidents in 2010-2011. From these one workers compensation claim case commenced with minimal time lost. CETI has appropriate mechanisms in place to ensure a safe and healthy workplace for its staff. Our approach incorporates a range of preventative measures to alleviate potential risks as well as mechanisms to deal effectively with any issues that arise. Regular workplace assessments are undertaken. Staff are required to report any hazards in the workplace and managers are required to initiate rectification of risks.
CETI offered a free vaccination program to staff as a means of reducing the incidence of seasonal flu within the workplace. The program was voluntary and was accessed by 19 of our staff in 2010/11.
CETI promotes a work life balance and ensures that staff access accrued leave regularly as part of this strategy. Staff must take at least one break of two weeks duration each year.
CETI operates in accord with the OH&S requirements of NSW Health and WorkCover NSW. Specifically:• We maintain a register of incidents • We have an OH&S Committee • An OH&S briefing is conducted as part of the orientation process for each new member of staff or contractor • OH&S is a standing item on the agenda of staff meetings
APPENDICES94
5 Appendices
Waste CETI complies with the NSW Government Waste Reduction and Purchasing Policy. Some specific actions taken include:• Our main office has been fitted with sensors to ensure lights are automatically turned off when a space is no longer
occupied after a set time • Staff turn off computers when leaving the office • We have ceased publishing a number of resources in hard copy and now only offer them online or via electronic
distribution to reduce paper usage and energy wasted in distribution• Implementation of an electronic data management system to reduce the volume of paper based records• Default double sided black and white printing on all photocopiers and printers • Recycling bins under desks• Recycling bins located in accessible office positions• Recycling of mobile phones, computer equipment and printer cartridges
Government Information (Public Access) Act 2009 (GIPA)CETI is committed to openness with regard to its information and is a public authority that is required to comply with GIPA obligations. Details of CETI’s structure and functions, and the kind of information it holds and how it may be accessed are contained in our publications guide. CETI makes available to the public all reports and information that it publishes, free of charge, on its website www.ceti.nsw.gov.au. Furthermore, the CETI publication guide on this website informs visitors in general terms:• the role, structure and functions of CETI• the kind of information held by CETI• information that is available to the public• how the information will be made available• whether or not there is a charge to access specific kinds of information
Access to documents, apart from free documents, is made via a request for access under the Government Information (Public Access) Act 2009. There were no access applications during the financial year 2010/11.
Credit card use and certificationIt is affirmed that for the 2010-11 financial year credit card use within CETI was in accordance with the Premier’s Memoranda and Treasurer’s Directions. Credit card use was limited to the settlement of accounts with the travel booking service. The organisation’s credit card policy is documented and statements are periodically lodged with management for consideration.
Compliance Requirements continued
CETI > ANNUAL REPORT 2010/11 95
Internal audit and risk management attestation statement
APPENDICES96
5 Appendices
ACI Agency for Clinical InnovationACRRM Australian College of Rural and Remote MedicineAHPRA Australian Health Practitioner Regulation AgencyAHS Area Health ServiceAMIHS Aboriginal Maternal and Infant Health ServicesBHI Bureau of Health InformationBPT Basic Physician TrainingBSF Building Strong Foundations for Aboriginal Children, Families and CommunitiesBSOC Basic Sciences in Oncology CourseCEC Clinical Excellence CommissionCETI Clinical Education and Training InstituteCTLP NSW Rural and Remote Clinical Team Leadership ProgramDoHA Department of Health and Ageing (Commonwealth)GP General PractitionerGPET General Practice Education and TrainingGWAHS Greater Western Area Health ServiceHSP Hospital Skills ProgramHSPIB Health Services Performance Improvement BranchHWA Health Workforce AustraliaIMET Institute for Medical Education and TrainingIRCST NSW Institute of Rural Clinical Services and TeachingJMO Junior Medical OfficerLEAD Leadership Development ProgramLEAP Future Leaders Development ProgramLHD Local Health DistrictLIFT Learning Innovation and Future TechnologiesLMEP Leadership and Management Essentials ProgramMPS Multi-purpose ServiceNaMO Nursing and Midwifery OfficeNPA-IECD Indigenous Early Childhood Development National Partnership AgreementOH&S Occupational Health and SafetyPEP Physician Education ProgramPGPPP Prevocational GP Placement ProgramPTAP Prevocational Training Allocation ProgramRACGP Royal Australian College of General PractitionersRACP Royal Australasian College of PhysiciansRRCBP Rural Research Capacity Building ProgramSTP Specialist Training ProgramTOTR Teaching on the RunTSU Training and Support Unit for Aboriginal Mothers, Babies and Children
VMO Visiting Medical Officer
Abbreviations
CETI > ANNUAL REPORT 2010/11 97
AccreditationThe process by which CETI evaluates and recognises a hospital institution or network as fulfilling applicable standards. The determination that a hospital or training term meets these standards is also referred to as accreditation of the training.
Area Health Service (AHS)A geographic division of health services in NSW. In 2011 new divisions were formed called Local Health Districts.
Australian Rural Health Research CollaborationThe Collaboration was established to address important inequalities in health between rural and urban communities and is a collaboration of three research centres: The Northern Rivers Centre, Lismore, comprising the Northern Rivers University Department of Rural with the Northern NSW LHD and Southern Cross University; The Australian Centre for Agricultural Health and Safety, Moree, with the Hunter New England LHD; and the Broken Hill Centre for Remote Health Research, comprising the Broken Hill University Department of Rural Health with the Far West LHD. The Collaboration is also affiliated with the School of Rural Health and Southern Cross University.
CapabilityAbility to be developed.
CapacityThe facility or power to produce, perform or deploy.
ClinicianA health practitioner or health service provider.
CompetencyAn individual’s demonstrated capacity to perform a task or skill to an agreed standard.
Consumers People using health services.
FacebookSocial media network that allows organisations to create a common interest user group page where people can view posts and make comments.
Four Pillar Organisations The Garling Report recommended that four centralised health organisations should be set up which were referred to as the “four pillars”. They are the Clinical Education and Training Institute (CETI), The Clinical Excellence Commission (CEC), The Agency for Clinical Innovation (ACI) and the Bureau of Health Information (BHI).
Garling Inquiry Special Commission of Inquiry Acute Care Services in NSW Public Hospitals.
Garling Report Final Report of the Special Commission of Inquiry Acute Care Services in NSW Public Hospitals, Peter Garling SC, November 2008.
Health Workforce Australia (HWA)HWA is an initiative of the Council of Australian Governments (COAG). It was established to meet the future challenges of providing a health workforce that responds to the needs of the Australian community. HWA will develop policy and deliver programs across four main areas—workforce planning, policy and research; clinical education; innovation and reform of the health workforce; and the recruitment and retention of international health professionals. HWA will also consider the adequacy and availability of workforce.
InterprofessionalPeople from different professions working, learning or collaborating together as part of a team and recognizing the unique skills that each person can contribute to influencing excellent patient care.
LinkedInSocial media site designed for professionals to contact colleagues, post questions and find answers.
Local Health District (LHD)In 2011, eight Area Health Services, the existing geographic divisions of health services in NSW, were replaced by 15 geographic divisions called Local Health Districts, two specialty networks and the St Vincent’s Network.
MinisterNSW Minister for Health, responsible for the administration of health legislation within NSW.
Multi-Purpose Service (MPS)Designed for rural and regional areas to combine a range of existing health and aged care services.
NSW HealthNSW Department of Health which monitors the performance of the NSW public health system and supports the statutory role of the NSW Minister for Health.
Glossary
APPENDICES98
5 Appendices
NSW Primary Health Care Research Capacity Building Program (NSW PHC) Funded by the Department of Health and Ageing to develop a capacity in primary health care in NSW to conduct and use the results of research and evaluation. It is a collaboration between seven university departments of the University of Newcastle, University of Sydney, University of New South Wales and the Australian National University. The State Advisory Committee oversees the broad direction and has members from the University Departments, the Royal Australian College of General Practitioners, the NSW Office of the Department of Health and Ageing, the Alliance of NSW Divisions, from NSW Health, allied health and other primary health care sectors.
Nursing Grand RoundsThese sessions provide opportunities for nurses to learn or expand their clinical knowledge base of practice from experienced peers, acknowledging and recognizing nursing expertise in colleagues, but also drawing on other clinical expertise. Nursing Grand Rounds are used as a teaching tool to help gain clinical competence and become more proficient in nursing processes, decrease staff isolation and promote professional development. The sessions include presentations of case studies, presentations of research studies and best practice interventions and care practices, and discussion of practice problems and issues.
Prevocational TrainingPrevocational Training is the base of medical education in which doctors develop competencies after completion of their basic medical qualification. The first two postgraduate years after medical graduation (PGY1 and PGY2) provide a grounding (or basis) for future vocational training. These first two or three years are spent primarily in public hospitals and /or community settings. State Postgraduate Medical Education Councils have been established in all states to oversee training and educational opportunities for junior medical staff in these early postgraduate years.
SuperguideA handbook for supervisors. Currently available for medical supervisors and planned for supervisors of allied health professionals.
Glossary continued
CETI > ANNUAL REPORT 2010/11 99
Aboriginal participation 8, 10-11, 15, 19, 21, 23, 91, 93Accounts payable performance 92Accreditation 3, 4, 5, 8, 15, 19, 21, 22, 32, 44, 45, 91Allied health 4, 5, 6, 8, 9, 10-11, 12, 13, 16, 17, 19, 20, 21, 28, 32Allied Health Directorate 4, 5, 6, 8, 9Allocation 4, 5, 10-11, 21, 23, 32, 45, 93Blended learning 8, 10, 24, 26, 29Centre for Learning and Teaching 4, 5, 7, 9, 10Chief Executive’s report 8Clinical Chair 9, 10, 27, 38-47, 90Collaboration 4, 6, 7, 8, 9, 10-11, 14, 16, 17, 18, 20, 21, 22, 24, 25, 30, 31, 32-33Committees 37-47Communication 4, 7, 8, 11, 14, 15, 17, 18, 25, 27, 29, 30-31, 34Competency 7, 8, 9, 10, 14, 16, 18-20, 21, 33, 42Compliance Requirements 90-95Conferences & forums 13Directorates and centre 5-7Disability plans 92EEO 91E-learning 7, 8, 10, 11, 12, 17, 24, 28-29Evaluation 3, 8, 9, 14, 15, 21, 22, 25, 33, 34, 90Excellence 4, 6, 9, 10, 17, 20, 29Financial performance overview 15Financial Report 48-89Flexible learning 7, 10, 14, 24, 29Four pillars 3, 8, 32Garling 3, 8, 9, 10, 16, 17, 18, 26, 28, 32, 37General Manager’s report 10Goals 14, 16-33Governance 4, 36-38Guidelines 7, 28Human Resources 90Innovation 4, 6, 7, 8, 9, 10-11, 14, 21, 23, 24-25, 29, 90Institute of Medical Education and Training (IMET) 3, 5, 9, 90International graduates 5, 11, 16, 42Interns 4, 5, 8, 10-11, 12, 17, 21-23, 30, 31, 32, 44-45, 90
Knowledge management 10, 14, 28-29Leadership 3, 6, 7, 8, 9, 10-11, 12, 16, 18, 21, 22, 26-27, 32Management and staff 36Management and structure 5, 36-38Medical Directorate 4, 5, 8Multicultural Policies and Services 93Networks 4, 5, 10-11, 12, 13, 16, 18, 19, 20, 21, 22, 23, 24, 26, 28, 29, 30, 31, 32, 33, 34, 37, 38, 40, 43, 44, 46, 92NSW Institute of Rural Clinical Services and Teaching (IRCST) 3, 5, 9, 25, 90Nursing and midwifery 4, 5, 6, 7, 8, 9, 10-11, 19, 21, 24, 25Nursing and Midwifery Directorate 4, 5, 6, 8, 9Nursing Grand Rounds 8, 11, 24, 25Office of CETI 4, 5, 9OH&S 93Operational highlights 10-11Overview of financial performance 15Overview of key achievements against goals 10-11Patient 3, 4, 5, 6, 7, 8, 9, 10-11, 12, 14, 16, 17, 18, 19, 20, 21, 22, 25, 28, 31, 37Prevocational 3, 5, 8, 9, 12, 13, 21-23, 28, 30-31, 32, 34, 44-45, 92Professional development 3, 4, 6, 10-11, 14, 15, 18-20, 41, 90Publications and Resources 12Report against our goals 16-35Research and development 90Risk management 92, 95Rural 3, 4, 5, 8, 9, 10-11, 12, 13, 15, 16, 18-19, 21-23, 24-25, 28-29, 32-33, 90, 93Rural and Remote Directorate 4, 5, 8Scholarship programs 5, 11, 13, 15, 19, 21, 32, 33Simulation 8, 10-11, 17, 24, 90Social media 11, 28-29, 30Stakeholders 4, 7, 8, 9, 10-11, 17, 18, 29, 30, 32, 34, 37Standards 3, 7, 8, 9, 10-11, 14, 24, 26-27, 28-29, 33, 37, 90Superguide 8, 9, 10-11, 12, 20, 21, 28Team Health 7, 8, 9, 10-11, 13, 16-17Technology 4, 7, 8, 9, 16, 24, 28-29Workforce management 10-11, 12, 14, 21-23
Index
APPENDICES100
5 Appendices
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................
Notes

Production details
50 copies were produced. Total external costs for design and print were $9,081 (inclusive of GST).
Edited by: Dr Gaynor Heading and Rod West
Design: Clik Creative www.clikcreative.com.au
Printer: PrintroomThis report is printed on Monza Recycled paper

Clinical Education and Training Institute (CETI)
Building 12 Gladesville Hospital GLADESVILLE NSW 2060
Tel: (02) 9844 6551 Fax: (02) 9844 6544 www.ceti.nsw.gov.au [email protected] Post: Locked Bag 5022 GLADESVILLE NSW 1675