Embed Size (px)
Citation preview

WEEK OF 9/21-9/24
DOMMR

Objectives
Discuss the epidemiology of cervical cancer and methods of screening Will focus specifically on the Pap Smear as a screening
method
Review the Bethesda Classification System for reporting cervical cytology
Discuss when cervical cancer screening should start, how frequent it should be done, and how long to continue
Review the interpretation of cytology seen on pap smears

Cervical Cancer - Epidemiology
• A disease of sexually active women• Risk factors:
– HPV infection– Cigarette smoking– Immunosuppression– Three or more lifetime sexual partners or 1st intercourse before Age
18 – Maternal DES (diethylstilbesterol) exposure during pregnancy – A previous abnormal Pap smear
• 2nd most common female cancer worldwide• Most often a disease of adult women, rarely seen in
adolescents• Most common in developing countries• In 2008, 11,070 new cases of invasive cervical cancer in
the US– 3870 expected cancer related deaths

Cervical Cancer
• Cervical intraepithelial neoplasia (CIN) is the pre-invasive dysplasia of cervical epithelial cells• Precursor of malignant disease
• Categorized by depth and atypicality of cells in the cervical epithelium (CIN 1-3)
• Slow malignant transformation leads to a long latency period
• Some low grade lesions may regress spontaneously– Rates of regression as high as 75% at 5 yrs in adults and
up to 91% at 3 yrs in adolescents

Cervical Cancer Screening
• The Pap smear introduced in 1941 by George Papanicolau who initially used this method to study the estrous cycle of guinea pigs
• Used to identify abnormal cells taken from the transformation zone (junction of ecto- and endocervix)
• Between 50-60 million pap smears done annually in the US– 3.5 million are read as abnormal– 2.5 million undergo diagnostic colposcopy
• An Australian study showed that a 15yr female has a 77% lifetime risk of undergoing at least one colposcopy
• Thin layer (or liquid-based) cervical cytology is also used in the US as another screening method– SurePath, ThinPrep

Pap Smear
• A screening test (used for asymptomatic patients), not diagnostic (to confirm a disease)
• Cannot be used for a definitive diagnosis or to initiate treatment
• Functions to screen for cellular abnormalities associated with an increased risk for cervical cancer
• Goal is to distinguish between lesions likely to progress to carcinoma verses those that aren’t
• Sensitivity and specificity are widely variable• Liquid based cytology has theoretical advantages
(lower incidence of inappropriate fixation and drying artifact) but never proven to have better accuracy

Pap Smear
• The pap smear has never been evaluated in a randomized controlled trials
• Only observational studies have given any evidence of improving mortality from cervical cancer– Screening implemented in Finland, Sweden, Iceland, but not
Norway• Before screening – all with similar rates of cervical cancer• After screening – all countries but Norway saw a decrease in
incidence of cervical cancer
• In the US, invasive cervical cancer is more likely from failure to perform appropriate screening rather than inaccuracies in screening– >50% of women with cervical cancer have never had screening
and another 10% have not had a pap smear in the last 5 yrs

Pap Smear
• Pap smear obtains cytologic results, but not able to assess tissue structure– Diagnosis of CIN or cervical carcinoma requires a
tissue sample, which is obtained by biopsy
• Bethesda system standardized terminology for reporting cervical cytology– First introduced in 1988, revised in 2001
– Now reports on the adequacy of the specimen– ASCUS category changed to ASC (ASC-US, ASC-H)– AGUS category changed to AGC
– Now tells origin of cell and further subcategorizes

Bethesda Classification System
• Atypical Squamous Cells (ASC) • Unspecified (ASC-US) - includes unspecified and favors
benign/inflammation • Cannot exclude HSIL (ASC-H)
• Low-grade squamous intraepithelial lesion (low-grade SIL) • Cellular changes associated with HPV• Mild (slight) dysplasia/CIN 1
• High-grade squamous intraepithelial lesion (high-grade SIL)• Moderate dysplasia/CIN 2• Severe dysplasia/CIN 3• Carcinoma in situ/CIN 3
• Atypical Glandular Cells of Uncertain Significance (AGC) • AGC distinguishes cell origin: endocervical, endometrial, or NOS• Further differentiated into: favors neoplasm, Adenocarcinoma in
situ (AIS), or adenocarcinoma

Bethesda classification
• 2001 revision now subcategorizes ASC into ASC-H and ASC-US– ASC-H comprises 5-10% of ASC overall– Subclassification hopefully allows physicians to more rapidly
evaluate a patient who may have CIN 2, 3
• There is some correlation between pap smear cytology results and biopsy results– i.e. LSIL cytology would yield CIN 1 histology– Of patients with LSIL, 45%CIN 1, 33% had no identifiable
pathology, 16% had CIN 2, 3
• Most common cytologic abnormality is ASC-US, seen in 3-4% of pap smears– LSIL seen in 2% of pap smears, HSIL in 0.5-1% of pap
smears

Atypical Glandular Cells
• Important to differentiate AGC (atypical glandular cells) from ASC (atypical squamous cells)
• AGC is a significant marker for neoplasia• AGC associated with premalignant or
malignant lesion 10-40% of the time• All with AGC should be referred for
colposcopy• Women >35yrs should also have endometrial
biopsy

Pap Smears
When should screening start? At age 21 or 3 yrs after first sexual intercourse
(whichever comes first)
How often should I screen for cervical cancer? Originally, annual screening was implemented in the
US More recently this frequency has been reconsidered

Frequency of pap smear screening
• “Protection from cervical cancer remained high up to 3 yrs after a negative pap smear”
• “Rates of severe cervical cytology (CIN 2 or worse) within 2 yrs of a normal pap smear was negligible (1 case per 4895 person-yrs of follow up)”
• “Duration of protection from a negative pap smear was greater with older age”– 55-69yrs – q 5yr screening was strongly protective and annual
screening had little advantage – Same results were not seen in women 20-39yrs
• “Using Markov model after 3yrs of negative pap smears, comparing annual vs triennial screening would detect:”– 3 more cases of cervical cancer per 100,000 women age 30-44– 1 more case per 100,000 women age 45-59– No extra cases in women age 60-64

When should screening end?
• More controversy on when you should stop screening – should we be screening after the age of 65yrs?
• Highest mortality from cervical cancer seen in older women who have never been screened. Yet, it is rare to see high grade lesions in older women who have been screened
• Mortality increase after age 65, but benefit of screening declines with age

When should screening end?
• No current screening guidelines• The decision is individualized • Dependent on:
– Life expectancy– Prior screening results– HPV status– Current sexual activity
• Generally, a women > 65yrs with 3 negative pap smears in the last 10 yrs, with no other risk factors needs no further screening

What if my patient had a hysterectomy?
Small risk of cervical cancer in patients with prior hysterectomy in which cervix was taken out
Certain groups at higher risk: Intact cervix post hysterectomy Hysterectomy done because of uterine or cervical
cancer Exposure to DES in utero

So what are the recommendations?
Cervical cancer screening guidelines from: USPSTF, ACS, ACOG
Regarding what type of screening: ACS and ACOG allow liquid base cytology and/or
routine HPV testing (for women >30yrs) USPSTF makes no recommendation on alternate
screening tests due to insufficient evidence

Age to initiate screening
Age to discontinue screening
Screening interval for cervical cytology
Post hysterectomy for benign disease
ACS (2002)
3 years after onset of sexual intercourse, or by age 21
Women may choose, if 70 years and 3 negative tests and no positive tests within last 10 years
Annual for conventional cytology: every 2 years for liquid-based cytology; for age >30, every 2 to 3 years after 3 normal consecutive smears and no increased risk
Not Indicated
ACOG (2003)
3 years after onset of sexual intercourse, or by age 21
Inconclusive evidence
Annual for age <30; for age >30, every 2 to 3 years after 3 normal consecutive smears, no history CIN 2 or 3, and no increased risk
Women may decline testing
USPSTF (2003)
3 years after onset of sexual intercourse, or by age 21
Age 65, if not at high risk
At least every 3 years Not indicated
Around the world, starting age for screening ranges from 18-30 while end age ranges from 58-70 (or indefinitely in Germany)

The Cervical Cytology Report
• Specimen type (pap smear, liquid based cytology)
• Specimen adequacy– Satisfactory
• Includes 8000-12,000 squamous cells and at least 10 well-preserved endocervical cells (or squamous metaplastic cells)– This indicates adequate sampling of the transition zone
– Endocervical cells not present• Repeat in 12 months or 6 months if certain risk factors
– Unsatisfactory• More than 75% of the cells are uninterpretable• Should always be repeated in 2-4 months
• Interpretation of result

ASC
Slightly enlarged nucleus, small perinuclear halo

ASC: ASC-US
• Most common abnormality on pap smear• Often associated with spontaneously,
resolving, self-limited disease• Reflexive HPV testing (**Preferred**)
– If positive, immediate referral to colposcopy – If negative, repeat cervical cytology in 12 months
• Repeat Cytology at 6 and 12 months– If normal, continue routine screening– If abnormal, immediate referral to colposcopy
• Immediate referral for colposcopy

ASC-US – Special Populations
• Adolescents (<20yrs)– High prevalence of HPV infection, very low risk of invasive
cervical cancer• Reflex HPV testing would lead to a high rate of colposcopy
– Should have follow up cytology at 12 months• HSIL colposcopy• LSIL or less repeat cytology at 12 months if ASC-US
remains at 24 months or now higher grade colposcopy
• Pregnancy– Never do endocervical curettage (ECC)– Can see increase in squamous metaplasia with pregnancy
• Infection/reactive changes, postmenopausal, immunosuppression: no difference

ASC-H
Refer for colposcopy and ECCNo HPV testing indicated initiallyIf colposcopy shows CIN 1 follow up
cytology in 6 and 12 months or HPV testing If cytology shows again shows ASC-US (or greater) or
HPV is positive colposcopy

LSIL
Dysplastic nuclear changes, binucleation

LSIL
Premenopausal 12-16% risk of CIN 2, 3 Colposcopy/biopsy is preferred method of follow up Reflex HPV testing is not helpful
77% of women with LSIL will have a positive HPV, so colposcopy referrals would not be reduced
These women get treated the same as someone with ASC-US with positive HPV testing colposcopy

LSIL – Special Populations
• Adolescents– Likely ASC-US representing transient HPV infection– Initial colposcopy deferred (risk of invasive cervical cancer is
near zero)– Repeat cytology in 12 months
• If HSIL colposcopy• If ASC-US repeat in 12 months ASC-US or higher grade lesion
colposcopy• Pregnant
– Colposcopy (can be deferred 6 months post-partum)– No ECC
• Post menopausal – 3 options– Immediate colposcopy– Reflex HPV testing – low rate of HPV in this population vs
adolescents so HPV testing can reduce rate of colposcopy– Repeat cytology in 6 and 12 months

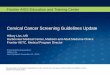
HSIL
Enlarged nucleus, less cytoplasm (increased N:C ratio). Irregular nuclear membrane

HSIL
• Over 50% will have CIN 2 or greater, 2% have invasive cancer
• Recommend either:• Colposcopy of entire cervix and vagina with biopsy of all visible
lesions and ECC • Unsatisfactory colposcopy
• Need diagnostic excisional procedure • Loop electrosurgical excision procedure (LEEP), conization
• Diagnostic excisional procedure• CIN 1 or less
– Will require further evaluation given the high prevalence of CIN 2 or greater in HSIL
– Diagnostic excisional procedure, repeat cytology and colposcopy at 6 and 12 months, review cytology, colposcopy and biopsy reports
• CIN 2, 3• Need excisional procedure

HSIL – Special Populations
• Adolescents– Colposcopy with ECC– If CIN I or less colposcopy with ECC q 6 months for
the next 2 years
• Pregnant– Colposcopy– CIN 2 or greater biopsy but not ECC– Often see spontaneous regression of CIN 2, 3 lesions

Review
• When should testing begin?• At age 21 or 3yrs after onset of sexual intercourse
• Annual screening until 3 consecutive negative pap smears. Then. . .– If <30yrs, repeat annually– If >30yrs, repeat 3 yrs– More frequently if at increased risk
• Screening can end if >65 and have had 3 negative pap smears in the last 10yrs– Possible exceptions: favorable life expectancy who are
sexually active with a new partner

Review
Cervical Cytology Report includes: Specimen type, specimen adequacy, interpretation of
result ASC (ASC-US, ASC-H) LSIL HSIL AGC

Review
ASC-US Usually do reflex HPV testing next, although can repeat
cytology or do colposcopy
ASC-H Referral for colposcopy and ECC
LSIL Generally go straight to colposcopy unless an adolescent,
who would get HPV testing first
HSIL Straight to colposcopy Consider diagnostic excisional procedure

Follow up of Patient
22y F who is currently sexually active with a new partner in the last month. Her last pap smear was 2 years ago and was normal. Pap smear done at this visit showed ASC-US
Reflex HPV testing was negativeWill repeat cytology in 12 months

Follow Up of Patient
63y F with history of HTN and hypothyroidism who presents for routine exam. Last pap smear was 3 years ago and was normal, although she has had a positive pap-smear with ASC-US in the past.
Pap smear done at this visit showed HSILWill refer for colposcopy