Embed Size (px)
Citation preview
CERVICAL DISC PROLAPSE
PRESENTOR:DR BALAJI.BMODERATOR:PROF DR K.PRAKASAM
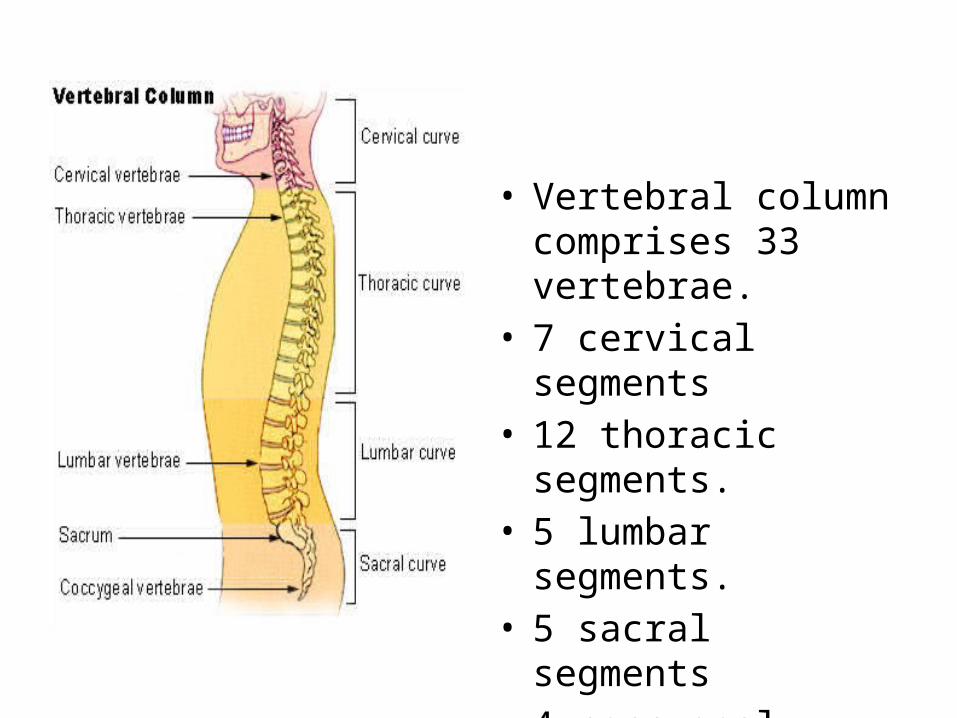
• Vertebral column comprises 33 vertebrae.
• 7 cervical segments• 12 thoracic segments.• 5 lumbar segments.• 5 sacral segments• 4 coccygeal segments.• The sacral and
coccygeal are fused.
• The disc is composed of two vertebral end plates with a central nulecus pulposus and outer ring of anulus fibrosus.
• Vertebral end plate are 1mm thick sheets made of fibrocartilage and hyaline cartilage.
• There are totally about 23 disc throughout the spine.
• As age increases hyaline cartilage gets converted in to fibrocartilage.
Anatomy of spine joints
• Individual vertebrae are connected to each other by facet joints.
• The interbody joints contain a specialized structures called intervertebral discs.
• The discs are found throughout the vertebrae except for the first and second vertebrae.
• The nucleus pulposus contains 80 to 90% of water.
• Proteoglycan constituting 65% and collagen constituting about 15 to 20 % of the dry weight.
• The annulus fibrous layer consists of about 12 concentric layer of lamellae with alternate layer of collagen.
• Annulus fibrous consists of about• 60 to 70% of water.• 50 to 60% of collagen• 20% of proteoglycan.
• Herniation of the cervical disc was identified by key in the year 1838.
• Common in men.• Factors associated with injury are• Frequent lifting of heavy objects on the job• Cigarette Smoking • Frequent diving from a board.
pathopysiology
• Physiological annular degeneration.• Frank extrusion of nuclear material• As the degeneration proceeds there is
hypermobility of the segment resulting of the instability or degenerative arthritic change.
• Internal disruption of the disc with annular tears results in disc prolapse.
• Pain radiating to the arm or chest• Numbness in the fingers• Motor weakness of the arm.• Mimics cardiac disease with chest and arm
pain.• Vertebral artery compression results in
dizziness, tinnitus, blurring of vision and retroocular pain.
• C5 nerve root compression motor : weakness of the deltoid and biceps. sensory: upper lateral arm and elbow.
• C6 nerve root compression motor: weakness of the biceps and extensor
carpi radialis brevis and longus. sensory: lateral forearm, thumb and index finger
• C7 nerve root compressionmotor: weakness of the triceps, wrist flexion and finger extension.sensory: middle finger
• C8 nerve root compressionmotor: weakness of the interossei and finger flexors and flexor carpi ulnaris.sensory: ulnar border of the arm.
Odom classification
• Type I : unilateral soft disc protrusion with nerve root compression.
• Type II : foraminal spur or hard disc with nerve root compression.
• Type III: medial soft disc protrusion with spinal root compression.
• Type IV : transverse ridge or cervical spondylosis with spinal cord compression.
Confirmatory imaging
• X-ray.• CT• MRI• Myelogram• Postmyelogram CT
TREATMENT
• Conservative management: • Rest • Massage• Ice• Antiinflammatory agents with active
mobilization.• Cervical traction with weight less than 10 lbs.• Cervical braces.
OPERATIVE TREATMENT
• Indications of surgery • Failure of non-operative pain management• Increasing and significant neurological deficit• Cervical myelopathy
• Soft lateral discs are easily removed with the posterior approach
• Soft central or hard discs are treated with anterior approach
• Spinal fusion are preceded with anterior approach with bone grafting.
• Use of bone graft the collapse of the disc space and maintains adequate foraminal disc.
• Posterior approach: midline incision is made on the spinous process.
• Ligamentum nuchae are divided, subperiosteal division of the paravertebral muscles.
• With high speed burr minimal bone is removed.• Ligamentum flavum is excised• With help of microscope the herniated nucleus
pulposus is removed.
• Minimally invasive posterior approach to the cervical spine.
• Indications:• Radiculopathy• Lateral disc herniation• Foramnial stenosis• Persistent or recurrent nerve root symptoms.
• contraindications:• Pure axial neck pain without neurologic
symptoms.• Cervical instability• Symptomatic central disc herniation• Kyphotic deformity that would make posterior
decompression.
• ANTERIOR APPROACH TO THE CERVICAL DISCS• Three basic technique done are• Cloward technique.• Smith-Robinson technique.• Bailey-badgley technqiue.
• Cloward technique involves making a round hole centered at the disc space. A slightly larger, round iliac crest into the disc space hole.
• Smith robinson technique it involves inserting a cortical strut of iliac crest into the disc space after removing the disc and cartilaginous endplate.
• The Bailey-badgley technique involves the creation of slot in superior and inferior vertebral bodies.
• This technique is most applicable to reconstruction when one or more vertbrae are excised.
• Biomechanically the smith robinson technique provides the greatest stability and least risk of extrusion.
ANTERIOR APPROACH• Patient positioned supine, with bolster placed
under the shoulder.• A 5-8 cms long transverse skin incision is made
on skin crease ipsilateral to the radiculopathy.• Skin, subcutaneous tissue and platysma muscle
are incised.• Blunt dissection to access the anterior column
of the cervical spine.
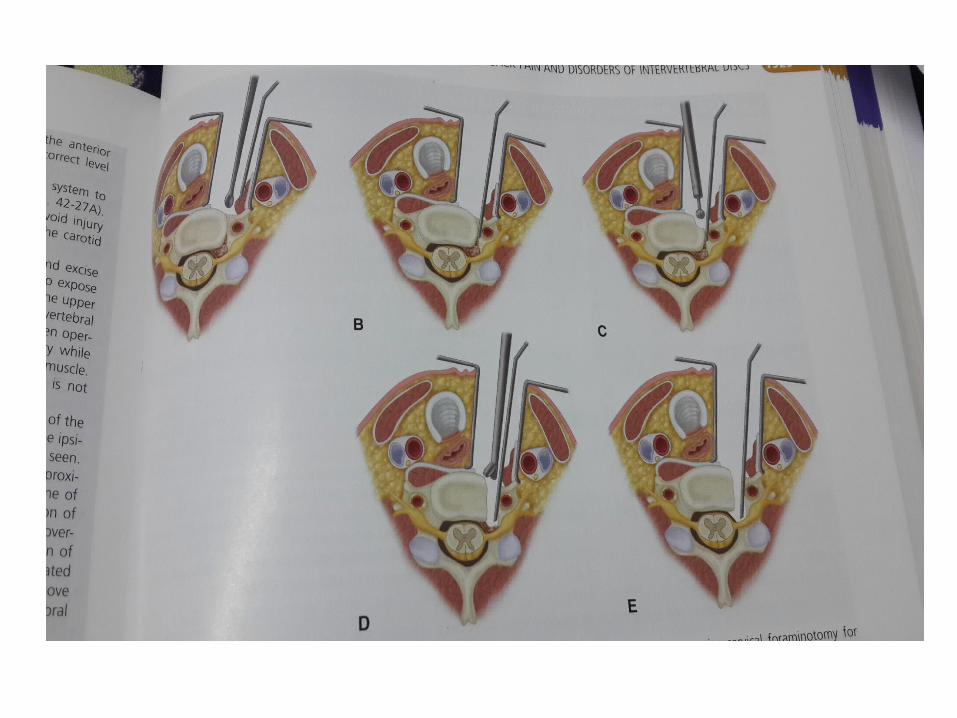
• Carotid artery and sternocleidomastoid muscle are retracted laterally and the muscle, trachea and esophagus medial.
• Prevertebral fascia is split to expose the anterior column of the cervical spine.
• longus colli muscle is identified and medial portion of the muscle is excised to expose transverse process.
• using a high speed drill, a drill is made between uncovertebral joint.
• Posterior longitudinal ligament is exposed and the lateral remnant of the uncinate process are dissceted.
• The remaining uncinate process is removed and decompression of the nerve root is done.
• A portion of the posterior longitudinal ligament is removed to find hidden ruptured disc.
CERVICAL DISC ARTHROPLASTY
• The primary argument favoring these device is that adjacent segment degeneration is minimized.
• Maintenance of motion is better with arthroplasty.
• Complication includes implant migration, heterotrophic ossification and recurrent radiculopathy.

THANK YOU